Artículos
Efficacy and tolerability of melatonin versus topiramate in migraine prevention
Eficacia y tolerabilidad de la melatonina frente al topiramato en la prevención de la migraña
Efficacy and tolerability of melatonin versus topiramate in migraine prevention
Archivos Venezolanos de Farmacología y Terapéutica, vol. 40, núm. 1, pp. 27-32, 2021
Sociedad Venezolana de Farmacología Clínica y Terapéutica

Esta obra está bajo una Licencia Creative Commons Atribución-SinDerivar 4.0 Internacional.
Recepción: 28 Diciembre 2020
Aprobación: 15 Enero 2021
Publicación: 10 Febrero 2021
Abstract:
Background: Migraine is one of the common neurological diseases. the aims of this study are to compare the effectiveness and tolerability of Topiramate and Melatonin drugs as monotherapy in the prophylaxis of migraine and to support the use of Melatonin as a preventive therapy.
Materials and Methods: a prospective, comparative study, in which 200 Patients diagnosed with migraine were enrolled. Monthly headache frequency, headache severity, mean attack duration in hours, and disability, were assessed at the baseline and at the end of 3rd month of follow up. Tolerability measures including the incidence of adverse events were recorded also.
Results: Forty patients withdrew from the study, the analysis was performed for the remaining cases, 160 patients, (76 in topiramate group and 84 in melatonin group). There was a significant improvement in the clinical response after 3 months of treatment in all parameters, and without significant differences between both groups.
Conclusion: this study showed that the Melatonin is effective as, if not superior to, Topiramate for episodic migraine prophylaxis. Moreover, it is more tolerated and has less adverse events than Topiramate.
Keywords: Migraine, Topiramate, Melatonin.
Resumen:
Antecedentes: la migraña es una de las enfermedades neurológicas más frecuentes. los objetivos de este estudio son comparar la eficacia y la tolerabilidad de los fármacos topiramato y melatonina como monoterapia en la profilaxis de la migraña y apoyar el uso de melatonina como terapia preventiva.
Materiales y métodos: estudio prospectivo, comparativo, en el que se inscribieron 200 pacientes diagnosticados de migraña. La frecuencia mensual de los dolores de cabeza, la gravedad del dolor de cabeza, la duración media del ataque en horas y la discapacidad se evaluaron al inicio y al final del tercer mes de seguimiento. También se registraron las medidas de tolerabilidad, incluida la incidencia de eventos adversos.
Resultados: Cuarenta pacientes se retiraron del estudio, el análisis se realizó para los casos restantes, 160 pacientes, (76 en el grupo de topiramato y 84 en el grupo de melatonina). Hubo una mejora significativa en la respuesta clínica a los 3 meses de tratamiento en todos los parámetros, y sin diferencias significativas entre ambos grupos.
Conclusión: este estudio mostró que la melatonina es eficaz, si no superior, al topiramato para la profilaxis de la migraña episódica. Además, es más tolerado y tiene menos efectos adversos que el topiramato.
Palabras clave: migraña, topiramato, melatonina.
Introduction:
Migraine is one of the common neurological diseases and it is characterized by throbbing unilateral headache attacks, that are associated with phonophobia, photophobia, nausea, and vomiting, and it is exacerbated by physical activity1.
Effective treatment of migraine starts with making a correct diagnosis, excluding the alternate causes, addressing the impact on the patient's life and educating the patient regarding therapeutic options, treatment duration, adverse effects profile and effects of psychosocial roles as part of the management2.
The pharmacologic types of treatment include abortive (acute) and preventive (prophylactic) therapy. These two types differ significantly in their mechanisms as abortive treatment is used to attenuate symptoms of the attacks whereas Preventive therapy is used to reduce headache frequency, severity, or duration3. Additional benefits for Preventive therapy, it may improve the ability of the patients to function, enhance the response to the acute treatments and reduce the costs of health care2.
However, because of the variety of migraine characteristics among patients and over time within the individuals and because most preventive treatments are not designed for migraine specifically and may have variable efficacies and adverse events or interactions. therefore, optimizing the treatment for each patient remained challenging and the use of these preventive medications or taking a maximum efficacy from them appeared only in few migraine patients1.
The use of evidence-based treatments is important to the success of migraine prevention2. There are several studies interested in finding other preventive drugs with fewer side effects and more effectiveness.
Topiramate was first approved in 1996 as an antiepileptic drug and was later approved in 2004 for migraine prophylaxis in adults4.
Melatonin has an analgesic mechanism and it can prevent the attacks by its ruling on neural pathways and neurotransmitters, for example, inhibiting dopamine release, limiting nitric oxide synthesis, and antagonizing excitotoxicity. Also, Melatonin can regulate the brain blood flow by suppressing Calcitonin gene-related peptide (CGRP) release. Lastly, it is reported that Melatonin levels are decreased in patients with migraine5,6.
Not many studies have been conducted to compare the effectiveness of Melatonin with topiramate, So the aims of this study are to compare the effectiveness and tolerability of these drugs as monotherapy in the prophylaxis of migraine and to support the use of Melatonin as preventive therapy.
Materials and Methods:
A prospective, open-label comparative study, in which 200 Patients diagnosed with migraine attending neurological consultation in teaching hospitals in Iraq, during the 1st ten months of 2020, were enrolled after obtaining informed consent and Institutional Ethics Committee approval.
Inclusion Criteria: 1. Patients aged between 18 to 65 years from both genders, fulfilling migraine diagnostic criteria according to the International Classification of Headache Disorders, experiencing more than 2 attacks/ month. Exclusion Criteria1. Any Patient was < 18 or > 65 years old. 2. If there was use of any prophylactic medication in the last 3 months.
3. If the migraine diagnosis was not definitely confirmed or there were other primary headaches (tension-type, cluster headache, etc) or secondary headaches in the same patient.
4. Any Pregnant and lactating woman.
5.If the Patient was allergic to any of the study medications 6. If the patient has any significant vascular (including uncontrolled hypertension), cardiac, neurological, renal, hepatic, or respiratory diseases. 7. Any Patient who has a major psychiatric disease and undergoing treatment.
8. Any patient who has medication overuse (taking ergotamine, triptan, nonsteroidal anti-inflammatory drugs, opioid, or combined analgesic medications for more than ten days per month, or taking simple analgesia for >15 days per month for more than three months.
The included patients were 200 and divided into 2 groups equally and each group received one of the prophylactic agents (Topiramate tablet 25 mg twice daily and melatonin tablet 3 mg once daily for three months). Use of acute migraine medication was permitted for breakthrough migraine attacks
§ Data regarding patients’ age, gender, age at onset of migraine, and family history of migraine were collected.
§ the number of migraine attacks (Monthly headache frequency), its severity (using Global assessment of migraine severity (GAMS))7, Headache duration in hours, and disability (using Migraine Disability Assessment (MIDAS) questionnaire in which there is 4 grades as follow: I ( 0-5) for Little or No Disability, II (6-10) for Mild Disability, III ( 11-20 ) for Moderate Disability and IV (21 or >) for Severe Disability ) were assessed and recorded at the baseline and at the end of 3rd month of follow up8.
§ Tolerability measures included the incidence of adverse events, involving those that led to the premature withdrawal from the study or serious adverse events that cause disability, those which were life-threatening; or required hospitalization. The adverse events were recorded if they were considered to be related to study medication.
Statistical Analysis: All collected information was entered in excel sheet and analyzed using IBM SPSS Statistics version 25 software, 2019. Descriptive statistics, Chi-square test, Fisher exact test, paired and unpaired-t-test were used.
RESULTS:
Demographic data
The number of patients who were randomized to treatment was 200. Treatment groups presented similar demographic and baseline clinical characteristics (Table 1). There were no significant differences in all variables.
Forty patients withdrew from the study, the analysis was performed for the remaining cases, 160 patients, (76 in topiramate group and 84 in melatonin group) (figure 1)
Table 1. Comparison of characteristics of patients in groups
| Group data | Total | Topiramate | Melatonin | P value* | |
| N. | 200 | 100 | 100 | ||
| Age in years (mean ± SD) | 31.36±9.53 | 31.77± 9.48 | 30.95 ± 9.61 | 0.544 | |
| Onset age of migraine (mean ± SD) | 24.92±8.68 | 25.67± 8.63 | 24.17± 8.70 | 0.222 | |
| Monthly headache frequency (mean ±SD) | 6.92±2.56 | 7.07 ± 2.56 | 6.77 ± 2.57 | 0.409 | |
| Severity of headache (mean ±SD) | 3.92±1.65 | 3.80 ± 1.63 | 4.03 ± 1.67 | 0.325 | |
| Headache duration in hours (mean ±SD) | 10.15±11.34 | 10.38 ± 11.68 | 9.92 ± 11.04 | 0.775 | |
| Headache disability: MIDAS (mean ±SD) | 13.98±7.68 | 13.68 ± 7.75 | 14.28 ± 7.63 | 0.581 | |
| Sex | M | 64 | 34 | 30 | 0.54 |
| F | 136 | 66 | 70 | ||
*Significant P value at < 0.05.
N.: Number, SD: Standard Deviation, M: Male, F: Female.
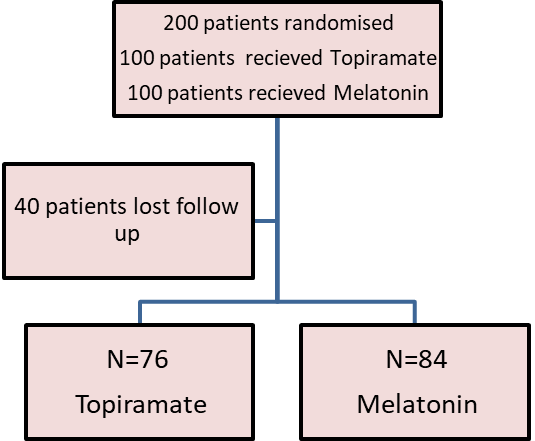
Figure 1:
the distribution of patients whose included in the study.
Clinical efficacy Measures:
The efficacy of both drugs was assisted by comparing the frequency of the number of migraine headache days per month, severity, mean duration of headache, and disability from the attacks at zero time and after 3 months of therapy, we found that there was a significant improvement in all parameters, in both groups, p <0.05. (Table 2)
Table 2. Comparison of headache characteristics before and after treatment in Topiramate and Melatonin groups:
| Group data | Topiramate | Melatonin | ||||
| Before treatment (mean±SD) | after treatment (mean±SD) | P value* | Before treatment (mean±SD) | after treatment (mean±SD) | P value* | |
| monthly headache frequency | 7.07 ± 2.56 | 3.82±1.97 | 0.000* | 6.77±2.57 | 3.71±1.88 | 0.000* |
| Severity of headache | 3.80 ± 1.63 | 2.57±1.54 | 0.000* | 4.03±1.67 | 2.49±1.47 | 0.000* |
| Headache duration in hours | 10.38±11.68 | 6.71 ± 7.47 | 0.017* | 9.92 ± 11.04 | 6.27 ± 6.68 | 0.008* |
| Headache disability: MIDAS | 13.68±7.75 | 10.16±7.67 | 0.003* | 14.28 ± 7.63 | 10.00±7.41 | 0.000* |
Also, there were no significant differences in all parameters at the baseline (as mentioned in table1) and in the clinical response after 3 months between both groups, p> 0.05. (Table 3)
Table 3. Comparison of clinical response in both groups
| Group data | Before treatment | P value* | After treatment | P value* | ||
| Topiramate (n=100) | Melatonin(n=100) | Topiramate(n=76) | Melatonin(n=84) | |||
| (mean±SD) | (mean±SD) | (mean±SD) | (mean±SD) | |||
| monthly headache frequency | 7.07±2.56 | 6.77±2.57 | 0.409 | 3.82±1.97 | 3.71±1.88 | 0.718 |
| Severity of headache | 3.80±1.63 | 4.03±1.67 | 0. 325 | 2.42±1.48 | 2.38±1.43 | 0.737 |
| Headache duration in hours | 10.38±11.68 | 9.92±11.04 | 0. 775 | 6.71±7.47 | 6.27±6.68 | 0.694 |
| Headache disability: MIDAS | 13.68±7.75 | 14.28±7.63 | 0.581 | 10.16±7.67 | 10.00±7.41 | 0.893 |
The percentages of complete and well responders (in which there were ≥ 50% reduction in attack frequency), after 3 months of treatment, were more prominent in the Melatonin group (38 from 84 patients (45.2%)) than of topiramate group (31 from 76 patients (40.8%)), but statistically, this difference was not significant, table 4. those with complete responses were higher in Topiramate group than in the Melatonin group (9.2 vs. 8.3%), (7 patients in both groups).
Three patients (3.9%) experienced worsening of their headache in the Topiramate group, while one patient (1.1%) experienced that in the Melatonin group.
The percentage of patients with responder rates (≥ 50% reduction) in migraine severity was 35.5% in the Topiramate group and 40.5% in the Melatonin group. But there is no statistical difference between them, table 4.
Table (4) Comparison of the responder rate between topiramate and melatonin groups
| The responder rate | Topiramate (%)76 (100%) | Melatonin (%) 84(100%) | P value* | |
| Frequency | ≥ 50% reduction | 31 (40.8%) | 38 (45.2%) | 0.57 |
| < 50% reduction | 45(59.2%) | 46(54.8%) | ||
| Severity | ≥ 50% reduction | 27(35.5%) | 34(40.5%) | 0.52 |
| < 50% reduction | 49(64.5%) | 50(59.5%) | ||
The percentages of patients who had a reduction in mean headache duration were about 51% in both groups (39/76 in topiramate group and 43/84 in melatonin group), while those with ≥ 50% reductions in mean duration were 26.3% (20/76) in the Topiramate group and 31% (26/84) in the Melatonin group. The differences between the two groups were not statistically significant, Table 3.
According to MIDAS, there was a reduction in mean scores from 13.68 ± 7.75 to 10.16 ± 7.67 in the Topiramate group, and from 14.28 ± 7.63 to 10.00 ± 7.41 in the Melatonin group, table 2. The differences in the reduction of disability between the two groups were not statistically significant, Table 3.
Tolerability and safety:
Forty patients were withdrawn from the study, adverse events occurrence was the most common reason for premature withdrawal for all randomized patients (Table 5)
Table (5): the side effects in both treatment groups
| Side effects | Topiramate(N=76)(%) | Melatonin(N=84)(%) | P value* |
| Sleepiness | 15(19.7) | 15(17.8) | 0.760 |
| Dizziness | 7(9.2) | 10(11.9) | 0.580 |
| Paresthesia | 30(39.4) | ------ | 0.000* |
| Anorexia | 13(17.1) | ------ | 0.000* |
| Fatigability | 7(9.2) | 5(5.9) | 0.434 |
| Dry mouth | 2(2.6) | ------ | 0.134 |
| Diarrhea | 3(3.9) | ------ | 0.066 |
| Worsening headache | 3(3.9) | 1(1.1) | 0.264 |
| Constipation | ------ | 1(1.1) | 0.340 |
| concentration/attention difficulties | 10(13.1) | 3(3.5) | 0.026* |
| Tremor | 3(3.9) | ------ | 0.066 |
Tolerability was evaluated according to adverse events that are reported by the patients, where 127 adverse events recorded by 77 patients, most of them (72.4%) occurred in the Topiramate group, the most common adverse events were Paresthesia (39.4%) in the Topiramate group (ameliorated with potassium supplements) and sleepiness in both groups.
DISCUSSION:
Melatonin and migraine are linked in several ways and the physiological effects of Melatonin prove the effectiveness of it in the prophylaxis of chronic headaches5,9,10.
The present study was a prospective, comparative study, in which the effectiveness of Topiramate and Melatonin in a migraine prophylaxis, their tolerability and the disability associated with migraine before and after treatment were compared.
200 patients participated in this study, the mean age of patients was about 30 years, 136 (68%) of them were female. These findings suggest that migraine is more common in females and at the mean age of thirties, these findings are supported by many studies like of Kelman L, who found that "a total of 86.3% patients were female and mean age was 37.7 years +/- 11.7 years"11.
Clinical efficacy:
Effective migraine prevention depends on Patient expectations as well as treating clinicians, most clinicians accept evidence-based expectations of reducing attack frequency and severity by 50%.
Therefore, the goal of appropriate preventive treatment is improvement the quality of care for migraine patients by a 50% reduction in the attack frequency and severity, and by the improvement of the Performance and productivity12.
160 patients (76 in the topiramate group and 84 in the melatonin group) completed the study. Melatonin was at least as effective as Topiramate in the reduction of the monthly rate of migraine episodes from prospective baseline to the end of the treatment phase. There were no statistically significant differences between both groups in any of the prescribed efficacy variables.
The responder rate (≥50% reduction in attack frequency) in the Topiramate group was 40.8%, and this is compatible with (Brandes JL et al, 2004 and Silberstein SD et al, 2004)13,14, in which the responder rates were 39% and 35.9%, respectively, in patients on 50 mg daily dose (as in this study) but it was higher with 100 mg (49% and 54.0%) and 200 mg (47% and 52.3%). This mean that 50 mg is still effective but it is not the optimal dose of Topiramate, although the side effects are more common with larger doses and these may lead to stopping intake this medication by many patients in our society.
The mean duration of migraine episodes was 10.38 ± 11.68 and 9.92 ± 11.04 in Topiramate and Melatonin groups respectively, while it was around 18 -19 hours in other studies (Long R et al,2018; Gonçalves AL et al, 2016; Peres M et al, 2004; Dodick DW et al,2009)5,6,10,15, This deference may be related to early intake of acute abortive medication at the beginning of episodes in our society, and according to bits of advice given to those patients during the follow-up period, which definitely will decrease the duration of the attack. There was a significant reduction in mean duration in both groups, in the Topiramate group (as in Melatonin), 51% had shorter headache duration, and this compatible with Lampl et al, 200416, (64%), but it is not compatible with many studies which either show no significant reduction of duration with Topiramate as in Freitage, 200317, (only 30%) or only with 200 mg/day dose as in Brandes et al, 200413. In the Melatonin group, there was a greater percentage (although it is not statistically significant) of patients with ≥ 50% reduction in the mean duration than those of the Topiramate group. The result was compatible with (Peres M et al, 2004, and Gonçalves AL et al, 2016)6,10, in which, there was a significant reduction of headache duration in comparison to placebo.
According to the MIDAS questionnaire, the baseline scores were compatible with Ebrahimi-Monfared M et al,2017., after 3 months of treatment, there was a significant reduction in mean MIDAS in both groups, in addition, there was a reduction in percentages of patients with moderate to severe disabilities (in melatonin group more than topiramate), these support the melatonin role in reducing disability and this is compatible with many studies. Ebrahimi-Monfared M et al, 2017., and Fallah R et al,201818.
In general, our data supports Melatonin’s therapeutic role in migraine prevention and it can reduce migraine frequency, severity and headache duration, in addition to its role in improving patient function and reducing disability.
Tolerability:
40 patients lost the follow up, mostly due to adverse events or strong improvement in their condition as they thought no more follow up was necessary or may be due to other causes including socioeconomic matters.
The majority of the adverse events were either mild or moderate in intensity and no serious event was reported during the study period. Among patients who used topiramate, there were no reports of glaucoma (primary or secondary), renal stones, or acute myopia in any patients, which if accrue, necessitate discontinuation of the drug. There were no clinically important mean changes in laboratory values or vital signs.
Some of the adverse effects have a significant frequency in the Topiramate group in comparison to the Melatonin group such as Paresthesia (the most frequent side effects), Anorexia, and concentration/attention difficulties. Paresthesia is reported in 39% only, this percentage is less than that reported by Silberstein SD19, (50%), this is may be due to the use of 50 mg (not 100 mg) daily dose in the current study and this results is compatible with Adelman J et al20.
The most frequent adverse events in the Melatonin group was Sleepiness, and this compatible with other studies (Fallah R et al,2018, and Long R et al,2019)5,18.
Melatonin was more tolerable than Topiramate, as most of adverse effects (92 versus 35) and numbers of patients those lost the follow up (24 versus 16) or experienced worsening of headache (3 versus 1) occur in the Topiramate group.
The results showed that both drugs were effective, and melatonin was more tolerated than topiramate.
Several limitations were reported in this study including study design (open label), lack of control group, lack of long-term follow-up and short term treatment, and poor assessment of sleep quality. Where the effect of Melatonin may be more significant in patients with decreased melatonin production and migraine associated with delayed sleep syndrome (Alstadhaug et al., 2010; Peres, 2011)21,22. Lastly, to reduce the occurrence of side effects, the Topiramate dosage used in this study (50 mg/d) was lower than recommended (100 mg/d) (Silberstein SD, 2015; Gonçalves AL et al, 2016)2,6, which may have contributed to the lower efficacy observed in the topiramate treatment group. However, dosages of 25mg/d have been demonstrated to be effective, in Asian populations23.
Future studies are warranted to confirm the efficacy of melatonin in treating migraine patients.
Conclusion:
This study showed that the Melatonin is effective as, if not superior to, Topiramate for episodic migraine prophylaxis. Moreover, it is more tolerated and has less adverse events than Topiramate.
Acknowledgments
I extend my thanks to the colleagues in the Nineveh medical college and Baghdad teaching hospital, and I would like to thank all friends for their support for us in completing this study.
References
1. Charles J, Rapoport A. The American Headache Society’s Position Statement on Integrating New Migraine Treatments into Clinical Practice – Comments. Headache: The Journal of Head and Face Pain. 2019;59(4):629-629.
2. Silberstein S. Preventive Migraine Treatment. CONTINUUM: Lifelong Learning in Neurology. 2015;21:973-989.
3. He A, Song D, Zhang L, Li C. Unveiling the relative efficacy, safety and tolerability of prophylactic medications for migraine: pairwise and network-meta analysis. The Journal of Headache and Pain. 2017;18(1).
4. Nadin C. Topiramate: the evidence for its therapeutic value in the prevention of migraine. Core Evid. 2005;1(2):103-124.
5. Long R, Zhu Y, Zhou S. Therapeutic role of melatonin in migraine prophylaxis: A systematic review. Medicine (Baltimore). 2019 Jan;98(3):e14099.
6. Gonçalves AL, Martini Ferreira A, Ribeiro RT, Zukerman E, Cipolla-Neto J, Peres MF. Randomised clinical trial comparing melatonin 3 mg, amitriptyline 25 mg and placebo for migraine prevention. J Neurol Neurosurg Psychiatry. 2016;87(10):1127-1132.
7. Sajobi T, Amoozegar F, Wang M, Wiebe N, Fiest K, Patten S et al. Global assessment of migraine severity measure: preliminary evidence of construct validity. BMC Neurology. 2019;19(1).
8. Mourad D, Hajj A, Hallit S, Ghossoub M, Khabbaz LR. Validation of the Arabic Version of the Migraine Disability Assessment Scale Among Lebanese Patients with Migraine. J Oral Facial Pain Headache. 2019 Winter;33(1):47–53.
9. Ebrahimi-Monfared M, Sharafkhah M, Abdolrazaghnejad A, Mohammadbeigi A, Faraji F. Use of melatonin versus valproic acid in prophylaxis of migraine patients: A double-blind randomized clinical trial. Restorative Neurology and Neuroscience. 2017;35(4):385-393.
10. Peres MF, Zukerman E, da Cunha Tanuri F, Moreira FR, Cipolla-Neto J. Melatonin, 3 mg, is effective for migraine prevention. Neurology. 2004 Aug 24;63(4):757.
11. Kelman L. Migraine changes with age: IMPACT on migraine classification. Headache. 2006 Jul-Aug;46(7):1161-1171.
12. Dekker F, Neven AK, Andriesse B, Kernick D, Ferrari MD, Assendelft WJ. Prophylactic treatment of migraine by GPs: a qualitative study. Br J Gen Pract. 2012;62(597):268-274
13. Brandes JL, Saper JR, Diamond M, Couch JR, Lewis DW, Schmitt J et al; MIGR-002 Study Group. Topiramate for migraine prevention: a randomized controlled trial. JAMA. 2004 Feb 25;291(8):965-73.
14. Silberstein SD, Neto W, Schmitt J, Jacobs D; MIGR-001 Study Group. Topiramate in Migraine Prevention: Results of a Large Controlled Trial. Arch Neurol. 2004;61(4):490–495. doi:10.1001/archneur.61.4.490
15. Dodick DW, Freitag F, Banks J, Saper J, Xiang J, Rupnow M et al; CAPSS-277 Investigator Group. Topiramate versus amitriptyline in migraine prevention: a 26-week, multicenter, randomized, double-blind, double-dummy, parallel-group noninferiority trial in adult migrainous. Clin Ther. 2009 Mar;31(3):542-559.
16. Lampl C, Bonelli S, Ransmayr G. Efficacy of topiramate in migraine aura prophylaxis: preliminary results of 12 patients. Headache. 2004 Feb;44(2):174-176.
17. Freitag FG. Topiramate prophylaxis in patients suffering from migraine with aura: results from a randomized, double-blind, placebo-controlled trial. Adv Stud Med. 2003;3:S562–S564.
18. Fallah R, Fazelishoroki F, Sekhavat L. A Randomized Clinical Trial of Efficacy of Melatonin and Amitriptyline in Migraine Prophylaxis of Children. Iran J Child Neurol. Winter 2018; 12(1):47-54.
19. Silberstein SD. Topiramate in Migraine Prevention: A 2016 Perspective. Headache. 2017 Jan;57(1):165-178.
20. Adelman J, Freitag FG, Lainez M, Shi Y, Ascher S, Mao L et al. Analysis of safety and tolerability data obtained from over 1,500 patients receiving topiramate for migraine prevention in controlled trials. Pain Med. 2008 Mar;9(2):175-185.
21. Alstadhaug KB, Odeh F, Salvesen R, Bekkelund SI. Prophylaxis of migraine with melatonin: a randomized controlled trial. Neurology. 2010 Oct 26;75(17):1527-1532.
22. Peres M. Melatonin for Migraine Prevention. Current Pain and Headache Reports. 2011;15(5):334-335.
23. Lo YL, Lum SY, Fook-Chong S, Siow HC. A pilot study of topiramate dosages for migraine prophylaxis in an Asian population. J Headache Pain. 2010 Apr;11(2):175-178.
Notas de autor
waseem.qasim@uoninevah.edu.iq