Artículos
Barbiturates and valproates in the pharmacotherapy of epilepsy: clinical and psychological interactions
Barbitúricos y valproatos en la farmacoterapia de la epilepsia: interacciones clínicas y psicológicas
Barbiturates and valproates in the pharmacotherapy of epilepsy: clinical and psychological interactions
Archivos Venezolanos de Farmacología y Terapéutica, vol. 40, núm. 8, pp. 792-798, 2021
Sociedad Venezolana de Farmacología Clínica y Terapéutica

Esta obra está bajo una Licencia Creative Commons Atribución-SinDerivar 4.0 Internacional.
Recepción: 28 Junio 2021
Aprobación: 15 Agosto 2021
Publicación: 30 Noviembre 2021
Abstract: This paper analyzes the indicators of somatization, obsessive-compulsive disorders, interpersonal sensitivity, anxiety, depression, phobic manifestations, paranoia, and psychoticism in the context of pharmacotherapy of epilepsy with barbiturates and valproates. Pharmacological therapy for epilepsy should rely on a rationally adjusted regimen with antiepileptic medicines being patient-tailored and targeted; it should have high efficiency and safety in relation to social functioning and quality of patients’ life. The research findings show that the studied group of patients with epilepsy, exposed to valproate or barbiturate therapy, is characterized by heterogeneous clinical-psychopathological and pathopsychological features. Clinico-psychopathologically, barbiturates reveal severe affective disorders and psychopathic behavior in patients with epilepsy; pathopsychological examination refers to the prominence of indicators on the scales of somatization, depression, and psychoticism, expressed in the form of somatic complaints, individual organs and systems’ disorders, and accompanied by mental equivalents, in particular on the side of the cardiovascular system, musculoskeletal system, gastrointestinal tract, etc.; depressive manifestations are also evident, reflecting the depth of affective disorders, dysphorias, suicidal tendencies, low mental activity with cognitive signs of depression, and the inclination to an avoidant, isolated lifestyle. Clinically, valproate therapy showed a predominantly neurotic character of mental changes; pathopsychological examination revealed the prevalence of obsessive-compulsive disorders, alternated with the anxiety, somatic and cognitive manifestations of anxiety.
Keywords: barbiturates, epilepsy, pharmacotherapy, psychopharmacotherapy, valproates.
Resumen: Este artículo analiza los indicadores de somatización, trastornos obsesivo compulsivos, sensibilidad interpersonal, ansiedad, depresión, manifestaciones fóbicas, paranoia y psicoticismo en el contexto de la farmacoterapia de la epilepsia con barbitúricos y valproatos. La terapia farmacológica para la epilepsia debe basarse en un régimen ajustado racionalmente con medicamentos antiepilépticos adaptados y dirigidos al paciente; debe tener una alta eficiencia y seguridad en relación con el funcionamiento social y la calidad de vida de los pacientes. Los resultados de la investigación muestran que el grupo estudiado de pacientes con epilepsia, expuestos a la terapia con valproato o barbitúricos, se caracteriza por características clínico-psicopatológicas y fisiopatológicas heterogéneas. Clínico-psicopatológicamente, los barbitúricos revelan graves trastornos afectivos y comportamientos psicopáticos en los pacientes con epilepsia. El examen fisiopatológico se refiere a la prominencia de indicadores en las escalas de somatización, depresión y psicoticismo, expresados en forma de quejas somáticas, trastornos de órganos y sistemas individuales, y acompañados de equivalentes mentales, en particular en el lado del sistema cardiovascular, musculoesquelético. sistema, tracto gastrointestinal, etc.; Las manifestaciones depresivas también son evidentes, reflejando la profundidad de los trastornos afectivos, las disforias, las tendencias suicidas, la baja actividad mental con signos cognitivos de depresión y la inclinación a un estilo de vida evitativo y aislado. Clínicamente, la terapia con valproato mostró un carácter predominantemente neurótico de cambios mentales. El examen fisiopatológico reveló la prevalencia de trastornos obsesivo-compulsivos, alternando con ansiedad, manifestaciones somáticas y cognitivas de ansiedad.
Palabras clave: barbitúricos, epilepsia, farmacoterapia, psicofarmacoterapia, valproatos.
Introduction
One of the most common psychoneurological diseases is epilepsy22. According to the new definition of the International Antiepileptic League 2014, epilepsy is a brain disease that reveals itself in any of the following conditions:
1. At least two unprovoked (or reflex) epileptic seizures with an interval of more than 24 hours.
2. One unprovoked (or reflex) epileptic seizure and the probability of repeated seizures corresponding to the overall risk of recurrence (equal to or more than 60%) after two unprovoked epileptic seizures in the next ten years.
3. Diagnosis of the epileptic syndrome.
The main goal of antiepileptic therapy is to keep the upper hand on seizures, which implies reducing the frequency of seizures, reducing their duration and minimizing the development of generalized seizures, and as a result, induction of remission. The main and leading role in the treatment of patients with epilepsy is played by anti-seizure medication, which requires a fairly long time to be taken1.
At present time, pharmacological therapy for epilepsy should rely on a rationally adjusted regimen. Antiepileptic drugs are patient-tailored and targeted. There are many factors to consider: gender, age of the patient, the nature of seizures, frequency of seizures, disease duration, comorbidities; it is also important to consider the way of life of a patient and his/her preferences5,7,23,30.
Epilepsy is a chronic disease that, in most cases, requires prolong and continuous antiepileptic therapy. It is established that to go into complete remission it takes at least 5 years of anticonvulsant therapy starting from the moment of the last seizure of any type. Only then can we talk about remission and withdrawal from antiepileptic medication16.
In patients with epilepsy, many mental processes change during the disease: attention36, memory, thinking37,38, emotional and volitional disorders are revealed 34, 35. Therefore, in clinical trials of epilepsy, a large role is assigned to psychological research aimed at diagnosing the impaired and retained aspects of the psychic setup40.
For a larger number of patients with epilepsy, the prognosis is relatively favorable, although some patients still fail to go into complete remission, despite being treated with several antiepileptic drugs. This is attributed to the development of pharmacological resistance and so-called pharmacoresistant epilepsy7,20,21,25. The mechanism of resistance is still poorly understood, however, as a result of observations, some factors have been identified that explain the development of this condition. These include: first, violation of the medication regimen, alcohol abuse; an important point is an early start of taking antiepileptic drugs, the seizure type, poorly adjusted dosage of drugs, and a high frequency of seizures during the diagnosis of pathology22.
To date, no consensus has been formed on the most rational treatment regimen for epilepsy. Although monotherapy remains the preferred method of treatment with antiepileptic drugs for pharmacoresistant and newly diagnosed epilepsy, there is no substantial evidence in favor of monotherapy or polytherapy for epilepsy. When choosing each pharmacotherapy regimen, there may be positive and negative aspects, so it is important to tailor the regimen to the specific case. The advantages of monotherapy over polytherapy are not yet confirmed, and they lose their significance against a combination of drugs that have a synergistic interaction17,18.
Initially, all patients are recommended to prescribe one antiepileptic drug (monotherapy). If the initial treatment was unsuccessful, the monotherapy can be retained using another drug. However, one should be careful when switching from one drug to another. If one antiepileptic drug does not work due to side effects or ongoing seizures, one should start taking the second drug (which may be an alternative drug of the first or second line) and bring it to an adequate or maximum tolerated dose and then gradually reduce the dose of the first drug. Combined therapy will be effective only if a long-lasting monotherapy with antiepileptic drugs does not lead to the elimination of seizures. If attempts to use combined therapy do not bring noticeable results, one should return to the regimen (monotherapy or combined therapy), which turned out to be the most acceptable in terms of achieving an optimal balance between efficiency, low frequency of seizures, and development of side effects17,18,27.
Over time new drugs appear that are used in monotherapy and have an advantage over the combined therapy. At present time, the combined therapy of lamotrigine and valproate is the only well-documented synergistic scheme19,24,28.
There was a survey that focused on the opinion of experts during the choice of antiepileptic drugs with reference to various indicators. Valproate is considered the first-line therapy (drug of choice) for genetically determined generalized tonic-clonic seizures epilepsy, except for women of childbearing age. Particular preference was given to lamotrigine and levetiracetam, prescribed for generalized tonic-clonic and myoclonic seizures, for the initial treatment of focal seizures, and like the drug of choice for epilepsy for women of childbearing age and the elderly26.
In elderly people, treatment of epilepsy is significantly difficult because of the presence of concomitant somatic diseases, the probability of drug interactions, as well as differences in pharmacokinetics and pharmacodynamics. Many antiepileptic drugs are widely used for various types of seizures and convulsive disorders. However, there is limited concrete evidence for the efficacy, safety, and tolerability of these treatments in the elderly6,8. Lamotrigine and levetiracetam have been sufficiently studied and have optimal evidence of safety, efficiency, and tolerability in the older age group. There are also findings confirming the safety, tolerability, and efficiency of topiramate, zonisamide, perampanel, lacosamide, oxcarbazepine, and eslicarbazapine14,16.
Drug safety in the treatment of antiepileptic drugs should seek an optimal balance between efficiency and side effects or toxicity. An important safety point for women is the risk of sudden seizures. The effect of antiepileptic drugs may be arrested due to interaction with oral contraceptives with an estrogen component. For lamotrigine and valproate, which are metabolized by uridine-5ʹ-diphospho-glycosyltransferase enzymes, the serum concentration decreases. On the other hand, inducing enzymes of anticonvulsants (carbamazepine, oxcarbazepine, phenytoin, phenobarbital, topiramate, felbamate, and perampanel) in combination with oral contraceptives can lead to unplanned pregnancy26. Accordingly, women of childbearing age (including young girls who may need treatment at childbearing age) are not recommended to prescribe sodium valproate, except in cases when other options are ineffective or not tolerated, and there are no pregnancy prevention program14,17.
With a long-lasting, recurrent course of epilepsy, in most cases, there occurs a disturbance of cognitive functions in patients. These disorders can be explained by several reasons: the direct origin of the epileptic syndrome, the epileptic seizure itself, and the antiepileptic therapy mechanism, namely, the side effects of these drugs. Practically all anti-seizure drugs, from different groups, with different mechanisms of action, to some extent, have a negative impact on the mental status of patients. Antiepileptic drugs with an inhibitory effect, have the most adverse effect on the cognitive-emotional sphere, these include barbiturates and benzodiazepines. Various findings emphasize that barbiturates have a negative impact on children's intellectual abilities. Drugs containing valproic acid, on the contrary, have the least pronounced effect on the emotional and volitional sphere of patients. Levetiracetam, brivaracetam, lamotrigine has the most positive effect on the patient's cognitive status. In patients with partial epilepsy, levetiracetam can significantly improve the patient's attention span. The degree of severity of cognitive impairment is individual and depends on the initial psychological status, level of intelligence, and milieu.
Therefore, it can be concluded that developers of antiepileptic drugs have recently set a goal to achieve high drug effectiveness, excluding the development of resistance to therapy and reducing the side effects of drugs. New antiepileptic drugs that target synaptic endings are well tolerated and provide the best progress in the control over epileptic seizures. They have a positive impact on the social functioning and quality of life of patients with epilepsy32.
Many antiepileptic drugs (AED) have a multiple-factor mechanism of action, impacting one or another (sometimes) several ion channels and simultaneously transmitter systems. Valproic acid and its salt, sodium valproate, are derivatives of a group of double-stranded fatty acids. Valproic acid suppresses the enzyme GABA transferase and, as a result, increases the content of the inhibitory neurotransmitter – gamma-aminobutyric acid (GABA) – in the nervous system. When GABA accumulates in the central structures of the brain, the threshold of excitability and the level of convulsive readiness decreases. Valproates also prevent an excess Na+ flow into the cell and counteract the paroxysmal depolarization shift of the membrane potential of the epileptogenic neuron. High tolerability to valproic acid is determined by the fact that it is almost completely metabolized in the liver, mainly in the mitochondria by β-oxidation and glucuronidation, slowing down hepatic metabolism. Valproates have a high ability to bind to plasma proteins. Barbiturates are derivatives of barbituric acid. When they interact with the chorionic part of the GABA-benzodiazepine receptor, it increases the duration of ion channels’ opening for Cl.. This activates the benzodiazepine part of the GABA-BD receptor and increases the inhibitory potential of the GABA-ergic system. Barbiturates also inhibit the rapid discharge of potential-dependent sodium channels. The poor tolerability of barbiturates is determined by the fact that their prolonged use causes the accumulation of these slowly metabolizing drugs since they are inductors of microsomal liver enzymes. With severe accumulation, chronic intoxication occurs. Apart from that, they have auto-and heteroinducing activity.
The development of new antiepileptic drugs is a significant problem, as in recent years there has been an increase in the number of patients with uncontrolled forms of epilepsy. The development of second-and third-generation antiepileptic drugs aimed at synaptic transmission does not solve the problem of developing pharmacoresistance. Therefore, new drugs are required that would directly handle the cause of primary and secondary epilepsy, and not only suppress the symptoms of acute seizures7.
New antiepileptic drugs have allowed many patients to better tolerate and individualize treatment. Brivaracetam and perampanel are the latest approved anti-seizure medications that are being administered for various forms of epilepsy. Both drugs showed comparable results in randomized controlled trials and proved to be well tolerated. Brivaracetam is an analog of levetiracetam, which binds to the protein of synaptic vesicles and reduces the release of excitatory neurotransmitters, has a high and selective affinity, a faster time of penetration into the brain. Brivaracetam is effective for uncontrolled seizures without secondary generalization or with partial onset, as well as in the form of additional therapy. This drug is highly effective and safe, and in the future can be used as a frontline monotherapy for partial seizures3,13, 24.
Perampanel has a special and selective mechanism of action on the receptors of α-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid and is recommended for use in focal and generalized epilepsy. This is the latest Russian drug with a unique mechanism of broad-spectrum, highly effective, has minimal side effects, good tolerability, and can be used as monotherapy or addition in the treatment of generalized epilepsy and status epilepticus3.
Materials and Methods
The sample of the survey was constituted of 317 patients aged between 18 and 65 years old. When determining the form of the disease and the structure of the leading paroxysmal syndrome. The International League Against Epilepsy Classification of the Epilepsies (ILAE 2017) seizure types were utilized. The survey focused on patients mainly with focal epilepsy, with a disease length of up to 30 years. In the study sample, able-bodied patients accounted for 59.9 %, disabled – 40.1% of patients, most patients had secondary special and secondary education (77.9% of patients). The survey involved patients without severe cognitive impairment. The diagnosis in the examined patients was verified against results of clinical-neurological, psychopathological, pathopsychological, electroencephalographic examinations, and brain computed tomography. The survey employed the psychodiagnostic technique «Symptom checklist» (SCL-90-R), developed by Derogatis et al.10,11. This technique reveals the levels of an unfavorable psychological state to diagnose the psychosomatic status and, accordingly, reflects such indicators as true somatic manifestations and their psychological equivalents, various types of obsessive disorders (obsessive drives, obsessive fears, obsessive states), anxiety-depressive states, interpersonal sensitivity, aggressive manifestations, paranoid tendencies, psychotic disorders.
Statistical Methods. To divide patients according to neurobiological, clinical, psychopathological, pathopsychological, and social characteristics into homogeneous groups, based on the values of some measure of similarity between objects, the cluster analysis was made using the k–means method. Other hierarchical methods employed in the research were the “nearest neighbor” method, the “furthest neighbor” method, the pair-group method using arithmetic averages, and the centroid method. The final clusterization was completed with the help of the k-means method, which implied breaking the totality of objects into a previously known number of clusters to minimize the sum of intraclass variances. The following values were used to describe the results: median (Me), the value of the lower and upper quartile (Q1 and Q3). To assess clusterization, we employed significance levels of differences between the obtained centers for each of the p variables. Moreover, the significance of value differences in the groups obtained by cluster analysis was examined using the Mann-Whitney U test for independent samples and the confidence interval of the difference between medians (CI dMe). In multiple comparisons, the Bonferroni correction was employed to correct the corresponding p-values. In the first case, the differences were considered significant at p <0,0526. The practical implementation of the above methods was supplemented with the applied statistical software package Statistica 10.0 22, 27.
Ethical aspect. The research surveyed patients who gave consent and signed informed consent statements.
Results and discussion
The clusterization utilized in the survey has effectuated the division of all patients into two clusters, accounting for the dependence between the indicators of the studied scales and the options of pharmacotherapy. The first cluster was represented by patients whose pharmacotherapy structure included barbiturates (benzonal, hexamidine, phenobarbital) – 43,2% of patients, the second cluster was composed of patients taking valproates (valproic acid, depakine chrono, convulex) – 56,8% of patients.
Clinico-psychopathologically, patients taking barbiturates (cluster 1) had severe cerebrastenic disorders combined with dysphoric, psychopathic, and cognitive disorders as dominating side-effects. Patients taking valproates (cluster 2) mainly had disorders of the secondary neurotic level in the form of affective lability with anxiety-phobic disorders occurring on an asthenic background (Figure 1).
Fig. 1. Medians of the SCL-90 scales in patients taking barbiturates and valproates
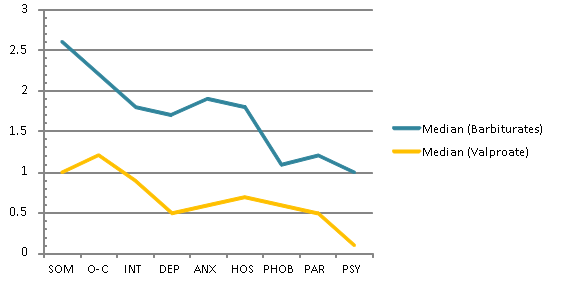
Fig. 1.
Medians of the SCL-90 scales in patients taking barbiturates and valproates
The results of the examination of patients taking barbiturates (cluster 1) and those taking valproates (cluster 2) with reference to SCL-90-R are shown in Table 1.
Table 1. Values of the SCL-90 scales, in patients taking barbiturates (TB=137) and valproates (TV=180), respectively
| Scales | Меb(Quantiles 25%, 75%) | Меv(Quantiles 25%, 75%) | U | Z | p-level | Z adjusted | p-level |
| SOM | 2.6 (1.3, 2.9) | 1 (0.6, 1.5) | 1674 | 6.7 | 0.0000 | 6.7 | 0.0000 |
| O-C | 2.2 (1.4, 2.5) | 1.2 (0.6, 1.8) | 2333 | 5.4 | 0.0000 | 5.4 | 0.0000 |
| INT | 1.8 (1.1, 2) | 0.9 (0.4, 1.3) | 1991 | 6.1 | 0.0000 | 6.1 | 0.0000 |
| DEP | 1.7 (1.3, 1.9) | 0.5 (0.3, 1.3) | 2237 | 5.6 | 0.0000 | 5.6 | 0.0000 |
| ANX | 1.9 (1.1, 2.2) | 0.6 (0.3, 1) | 1674 | 6.7 | 0.0000 | 6.7 | 0.0000 |
| HOS | 1.8 (1.5, 2.5) | 0.7 (0.3, 1.2) | 1054 | 7.9 | 0.0000 | 7.9 | 0.0000 |
| PHOB | 1.1 (1, 2.9) | 0.6 (0.3, 1.1) | 1935 | 6.2 | 0.0000 | 6.2 | 0.0000 |
| PAR | 1.2 (1.2, 1.3) | 0.5 (0.2, 1.2) | 2407 | 5.3 | 0.0000 | 5.3 | 0.0000 |
| PSY | 1 (0.7, 2.1) | 0.1 (0, 0.5) | 1959 | 6.1 | 0.0000 | 6.4 | 0.0000 |
| DOP1 | 10 (6, 10) | 3 (3, 10) | 2834 | 4.5 | 0.0000 | 4.6 | 0.0000 |
| GSI | 0.24 (0.2, 0.3) | 0.1 (0.1, 0.2) | 2117 | 5.8 | 0.0000 | 5.9 | 0.0000 |
| PSI | 82 (72, 86) | 68 (52, 77.5) | 2376 | 5.4 | 0.0000 | 5.4 | 0.0000 |
| PSDI | 0.3 (0.2, 0.3) | 0.16 (0.1, 0.3) | 2148 | 5.8 | 0.0000 | 5.8 | 0.0000 |
The data shown in the table indicate that there are significant differences in the following scales: somatization, depression, anxiety, obsessive fears (phobias), psychoticism.
In patients taking barbiturates (cluster 1), the somatization is prevalent (Me=2.6, Q1=1.3, Q3=2.9, p=0.0001), which reflects the manifestations of somatic disorders and complaints, as well as their mental equivalents from the cardiovascular system, musculoskeletal system, gastrointestinal tract organs, and other body systems; the depressive manifestations has a distinct manifestation as well (Me=1.7, Q1=1.3, Q3=1.9, p=0.0001), which reflects the pathology of the emotional sphere of the psychic setup in the form of affective disorders.
In patients taking valproates (cluster 1), the obsessive-compulsive disorders (IU=1.2, Q1=0.6, Q3=1.8, p=0.001) are prevalent, alternating with somatic and cognitive manifestations of anxiety.
The level of depression according to the SCL-90 in patients taking valproates is statistically significantly lower than that of patients taking barbiturates (U = 2237, Z = 5.6, p = 0.0001). In patients taking barbiturates (cluster 2), the most evident are indicators referring to the depression scale i.e. in the form of states of depression, dysphoria, suicidal tendencies, decreased mental activity with cognitive manifestations of depression (Figure 2).
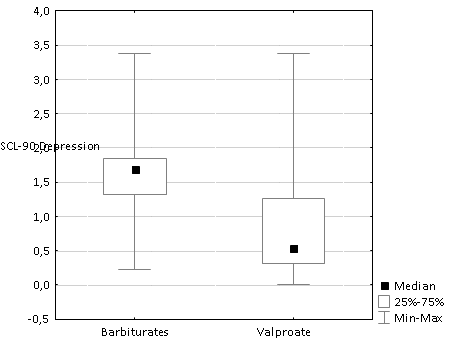
Fig. 2.
Medians of the SCL-90 Depression scale for patients taking barbiturates and valproates respectively
Indicators of paranoid disorders in the form of hostile behavior, suspicion to surrounding people, events in personal and public life (Me=0.5, Q1=0.2, Q3=1.2, p=0.0001), as well as psychoticism (Me=0.1, Q1=0, Q3=0.5, p=0.0001), are less prevalent in patients taking valproates, in comparison with paranoid ideation (Me=1.2, Q1=1.2,Q3=1.3,p=0.0001) and psychoticism (IU=1.0, Q1=0.7, Q3=2.1, p=0.0001), in patients taking barbiturates.
Conclusion
Rational, adequate psychopharmacotherapy is facilitative of reduction and complete elimination of seizures, inducing long-lasting remission, elimination of severe mental disorders; it also improves the social functioning and quality of life of patients with epilepsy.
This research effort looks into a comprehensive clinical and psychological assessment of patients with epilepsy, taking into account the indicators of clinical, psychopathological, and pathopsychological examinations with reference to the type of pharmacotherapy. The research findings allowed us to establish that the studied group of patients with epilepsy, undergoing either valproate therapy or barbiturate therapy, is characterized by heterogeneous clinical-psychopathological and pathopsychological features.
Clinico-psychopathologically barbiturates reveal severe affective disorders and psychopathic behavior in patients with epilepsy; pathopsychological examination defines a high degree of indicators pertaining to the scales of somatization, depression and psychoticism, which is expressed in the form of somatic complaints and disorders of the functions of individual organs and systems, accompanied by mental equivalents, in particular, from the cardiovascular system, musculoskeletal system, gastrointestinal tract, etc.; the indicator of depressive manifestations is also clearly identifiable, which reflects the depth of affective disorders, dysphorias, suicidal tendencies, decreased mental activity with cognitive manifestations of depression, and the inclination to an avoidant, isolated lifestyle. Valproate therapy showed a predominantly neurotic nature of mental changes in the clinical course of the disease; pathopsychological trial revealed the prevalence of obsessive-compulsive disorders indicator, alternated with the anxiety, somatic and cognitive manifestations of anxiety.
The obtained results significantly supplement the available findings on the pharmacotherapy of epilepsy and open up new opportunities for implementing treatment and rehabilitation measures in patients with epilepsy. The safety of medication when administering antiepileptic drugs should seek the achievement of an optimal balance between effectiveness and side effects or toxicity. The prototype medications development should rely on such drugs as perampanel, brivaracetam, eslicarbazepine, which can be used to handle various forms of epilepsy. Perampanel is a promising highly effective drug with favorable effects on partial and secondary generalized seizures. Brivaracetam is a derivative of levetiracetam, it’s a safe and effective alternative, prescribed especially for patients with behavioral side effects and administered as a complementary therapy for uncontrolled partial seizures with secondary generalization, focal and secondary generalized tonic-clonic seizures. In the future, it can be used as a first-line monotherapy for partial seizures. Lamotrigine and levetiracetam are the best options when effectiveness, safety, and tolerability are concerned, and optimal for the treatment of focal epilepsy in children and adults.
Therefore, the creation of new antiepileptic medications will allow individualizing the treatment of patients with epilepsy, to achieve high efficacy of the drug, excluding the development of resistance to therapy, to reduce the side effects, and to facilitate the improved social functioning and quality of life of patients with epilepsy.
References
1. Agrawal, N. Treatment of psychoses in patients with epilepsy: an update / N. Agrawal, M. Mula // Therapeutic Advances in Psychopharmacology – 2019.
2. Amirkhanian M. G. Antiepileptic pharmacotherapy is the leading factor in the induced pathomorphosis of epilepsy / M. G. Amirkhanian // Epilepsy and paroxysmal conditions – 2018. – 10(2). – Рр. 59 – 73.
3. Azizova, R., Features of clinical course of epilepsy associated with anxiety and depressive disorders / R. Azizova, O. Umirkulov // European science review. – 2018. – № 9-10-2.
4. Bertrand de Toffol et al. Pharmacotherapy in patients with epilepsy and psychosis / Bertrand de Toffol [et al.] // Epilepsy & Behavior – 2018. – №8. – Pр. 54–60.
5. Birru, E. M. Drug therapy of epileptic seizures among adult epileptic outpatients of University of Gondar Referral and Teaching Hospital, Gondar, Northwest Ethiopia / E. M. Birru, M. Shafi, M. Geta // Neuropsychiatr Dis Treat. – 2016. – №12. – Рр. 3213–3219.
6. Byung, In Lee Clinical opinion: Earlier employment of polytherapy in sequential pharmacotherapy of epilepsy / Byung In Lee, Kang Min Park, Sung Eun Kim, Kyoung Heo // Epilepsy Research. – 2019. – Рр. 156.
7. Campos, M.S. Efficacy and Tolerability of Antiepileptic Drugs in Patients with Focal Epilepsy / M. S. Campos, L. R. Ayres, M. R. S. Morelo, F. A. Marques, L. R. L. Pereira // Systematic Review and Network Meta‐analyses. Pharmacotherapy. – 2016. – №36. – Рр. 1255–1271.
8. Landmark & Svein I Johannessen, C. J. Pharmacotherapy in epilepsy – does gender affect safety? / C. J. Landmark & Svein I Johannessen // Expert Opinion on Drug Safety. – 2016. – № 15:1. – Рр. 1-4.
9. Chaudhary, N. et al. Frequencies of CYP2C9 polymorphisms in North Indian population and their association with drug levels in children on phenytoin monotherapy / N. Chaudhary, M. Kabra, S. Gulati [et al.] // BMC Pediatrics. – 2016. – №16:66.
10. Derogatis, L. R. Neurotic symptom dimensions as perceived by psychiatrists and patients of various social classes / R. S. Lipman, L. Covi [et al.] // Arch. Gen. Psychiatr – 1971. – Vol. 24. – Р.454–464.
11. Derogatis, L.R. Confirmation of the dimensional structure of the SCL–90: a study in construct validation / L. R. Derogatis, P. A. Cleary // Clinical Psychol. –1977. – Vol. 33. – Р. 981–989.
12. Dzharashtieva, Dzan-Pago, Modern methods of pharmacotherapy of generalized forms of epilepsy / А. Bulgakova, Р. Shevchenko, S. Karpov, I. Vishlova // European science review. – 2017. – №3-4.
13. Farrokh, S. Use of Newer Anticonvulsants for the Treatment of Status Epilepticus / S. Farrokh, J. Bon, M. Erdman // Tesoro Pharmacotherapy – 2019. – 39. – Рр. 297-316.
14. Grynkiv, I. O. Cost analysis of epilepsy pharmacotherapy by valproic acid and carbamazepine / I. O. Grynkiv, O. B. Blavatska, O. M. Zaliska // Farmatsevtychnyi Zhurnal. 2018. – № 2. – Рр. 21-29.
15. Holtkamp, M. Pharmacotherapy for Refractory and Super-Refractory Status / M. Holtkamp // Epilepticus in Adults. Drugs 78. – 2018. – Рр. 307–326.
16. Milovanović, Jasmina R. et al. Evaluation of brivaracetam: a new drug to treat epilepsy / Milovanović, Jasmina R. [et al.] // Expert Opinion on Pharmacotherapy. – 2017. – 18:13, Рр. 1381-1389.
17. Jerry, J. Shih et al. Epilepsy treatment in adults and adolescents: Expert opinion / Jerry J. Shih [et al.] // Epilepsy & Behavior. – 2017. – № 69. – Pр. 186-222.
18. Juan, C. et al. Clinical guideline: antiepileptic drugs of choice for epileptic syndromes and epilepsies in pediatric patients / С. Juan [et al.] // Mex Neuroci. –2019. – 20(2), Рр. 89-96.
19. Kantae, V., Krekels, E. H. J., Esdonk, M. J. V. et al. Integration of pharmacometabolomics with pharmacokinetics and pharmacodynamics: towards personalized drug therapy / V. Kantae, E. H. J. Krekels, M. J. V. Esdonk, [et al.] // Metabolomics. – 2017. – 13(1), Р. 9.
20. Kopciuch, D., Barciszewska, A., Fliciński, J. et al. Analysis of pharmacotherapy regimen and costs in patients with drug-resistant epilepsy following vagus nerve stimulation therapy: a single-center study (Poland). / D. Kopciuch, A., Barciszewska, J. Fliciński [et al.] // Acta Neurol Belg. – 2020. – Рр. 120, 115–122.
21. Kumar, J. Sleep Related Epilepsy and Pharmacotherapy / J. Kumar, A. Solaiman, P. Mahakkanukrauh, R. Mohamed // An Insight. Front. Pharmacol. – 2018. – № 9. – Р. 1088.
22.Lang, T. A. Kak opisat' statistiku v meditsine. Annotirovannoye rukovodstvo dlya avtorov, redaktorov i retsenzentov [How to describe the statistics in medicine. An annotated guide to authors, editors and reviewers]. / T. A. Lang // Moscow: Practical medicine. – 2011.
23. Lance, W., Máire, O’Dwyer, Shankar, R. New anti-seizure medication for elderly epileptic patients / W. Lance, O’Dwyer Máire, R. Shankar // Expert Opinion on Pharmacotherapy. – 2019. – № 20:13, Р. 1601-1608.
24. Laurent, M. W., Bauer, S., Rosenow F., Strzelczyk, A. Recent advances in the pharmacotherapy of epilepsy: brivaracetam and perampanel as broad-spectrum antiseizure drugs for the treatment of epilepsies and status epilepticus/ М. W. Laurent, S. Bauer, F. Rosenow, А. Strzelczyk // Expert Opinion on Pharmacotherapy. – 2014. – Р. 1755-1765.
25. Li, H., Wang, B., Chang C., Wu M., Xu Y., Jiang Y. The Roles of Variants in Human Multidrug Resistance (MDR1) Gene and Their Haplotypes on Antiepileptic Drugs Response: A Meta-Analysis of 57 Studies. / H. Li, B. Wang, C. Chang, M. Wu, Xu Y., Y. Jiang // PLoS ONE.– 2015. – № 10(3).
26 . Loughman, A., Bowden, S., D'Souza, W. Cognitive functioning in general idiopathic epilepsies: a systematic review and meta-analysis /A. Loughman, S. Bowden, W. D'Souza / Neuroscience. Biobehavior Review. – 2014. – № 43. Р. 20-34.
27. Nasledov, A. Matematicheskiye metody v psikhologicheskom issledovanii. Analiz I interpretatsiya dannykh. Rukovodstvo [Mathematical methods in a psychological research. Analysis and interpretation of data. Tutorial]. / A. Nasledov. – Saint Petersburg: Rech Publ. – 2014.
28. Pharmacological treatment of epilepsy // Epilepsy, NICE. – 2020. – Рр. 1-12.
29. Powell, G., Marson, A. Pharmacotherapy for Medication-Resistant Epilepsy. /In J. Stern, R. Sankar, M. Sperling (Eds.), // Medication-Resistant Epilepsy: Diagnosis and Treatment Cambridge: Cambridge University Press. – 2020. – Рp. 179-186.
30. Ramzi, S. et al. Pharmacists' knowledge of issues in pharmacotherapy of epilepsy using antiepileptic drugs / S. Ramzi [et al.] // A cross-sectional study in Palestinian pharmacy practice. – 2017. – P. 39-44.
31. Rupa, J. et al. Depression in patients receiving pharmacotherapy for epilepsy: An audit in a tertiary care center / J. Rupa [et al.] // Pharmacological Reports. – 2019. – P. 848-854
32. Schulze-Bonhage, A. A. Review of pharmacotherapy for treating focal epilepsy: where are we now and how will treatment develop? / Schulze-Bonhage, A. A. // Expert Opinion on Pharmacotherapy – 2017. – 18:17. – Рр. 1845-1853.
33. Shlomo Shinnar, M. D., et al. Randomized Trial of Three Anticonvulsant Medications for Status Epilepticus / M. D. Shlomo Shinnar [et al.] // N Engl J Med. – 2019. – 381:2103-2113.
34.Tokareva, N.G., Zheleznova, E.V. Spetsifika lokusa kontrolya bol'nykh epilepsiyey [Specifics of locus of control in patients with epilepsy]. Vestnik Ural'skoy meditsinskoy akademicheskoy nauki. [Bulletin of the Ural Medical Academic Science]. –2014. – №3:49, Р.60-62.
35. Tokareva, N.G., Zheleznova, E.V. Kliniko-psikhologicheskaya otsenka emotsional'nykh rasstroystv u bol'nykh epilepsiyey [Clinico-psychological assessment of emotional disorders in patients with epilepsy]. Zhurnal nauchnykh rabot Zdorov'ye i obrazovaniye v XXI veke. [Journal of scientific papers Health and Education in the XXI century]. – 2016. – № 18:2. – Р. 214-216.
36.Tokareva, N.G., Zheleznova, E.V. Kliniko-psikhologicheskaya otsenka vnimaniya patsiyentov s epilepsiyey. [Clinico-psychological assessment of attention in patients with epilepsy]. Zhurnal nauchnykh rabot Zdorov'ye i obrazovaniye v XXI veke. [Journal of scientific papers Health and Education in the XXI century]. 2016. – №18: 1. – Р.28-30.
37. Tokareva, N.G., Zheleznova, E.V. Klinicheskaya otsenka spellinga u bol'nykh epilepsiyey [Clinical assessment of spelling in patients with epilepsy]. Zhurnal nauchnykh rabot Zdorov'ye i obrazovaniye v XXI veke. [Journal of scientific papers Health and Education in the XXI century]. – 2016. – № 18:1. – Р. 31-33.
38.Tokareva, N.G., Zheleznova, E.V. Kliniko-psikhologicheskaya otsenka aleksitimii u bol'nykh epilepsiyey podrostkovogo vozrasta [Clinico-psychological assessment of alexithymia in adolescent epilepsy patients]. Detskaya i podrostkova reabilitatsiya. [Childhood and teenage rehabilitation]. –2016. – №2:27. –Р.29-31.
39. Willems, L.M., Bauer, S., Jahnke, K. et al. Therapeutic Options for Patients with Refractory Status Epilepticus in Palliative Settings or with a Limitation of Life-Sustaining Therapies / L. M. Willems, S. Bauer, K. [et al.] // A Systematic Review. CNS Drugs. – 2020. – №34, Р. 801–826.
40. Zheleznova, E.V., Tokareva, N.G. Kliniko-psikhologicheskiye kharakteristiki rasstroystv funktsionirovaniya pri epilepsii [Clinico-psychological characteristics of the functioning disorders in epilepsy]. Rossiyskiy psikhiatricheskiy zhurnal. [Russian Psychiatric Journal]. – 2017. – №3. – Р.27-32.
41. Zeng, Q. Y, Fan, T. T., P. Zhu, et al. Comparative Long-Term Effectiveness of a Monotherapy with Five Antiepileptic Drugs for Focal Epilepsy in Adult Patients / Q. Y. Zeng, T. T. Fan, P. Zhu [et al.] // A Prospective Cohort Study. PLoS One. – 2015. – 6;10(7).