Artículos
Assessing the possible impact of patient’s demographic data on coronavirus symptoms
Evaluación del posible impacto de los datos demográficos del paciente sobre los síntomas del coronavirus
Assessing the possible impact of patient’s demographic data on coronavirus symptoms
Archivos Venezolanos de Farmacología y Terapéutica, vol. 40, núm. 8, pp. 806-810, 2021
Sociedad Venezolana de Farmacología Clínica y Terapéutica

Esta obra está bajo una Licencia Creative Commons Atribución-SinDerivar 4.0 Internacional.
Recepción: 28 Junio 2021
Aprobación: 15 Agosto 2021
Publicación: 30 Noviembre 2021
Abstract: Background and objective: A novel COVID-19 condition emerged in December 2019 and has held a dangerous prognosis. It started as an epidemic in China, particularly in Wuhan city. The ages of individuals prone to infection range from one-month-old to above 90 years. However, fewer cases were reported in kids and newborns. Peoples susceptible to infection are the aged, those taking immunosuppressive agents. Usually, Coronavirus holds flu symptoms, including fever (80-90%), dry cough (50%), and lethargy (20-40%); other symptoms include diarrhea. This survey intended to assess the impact of patients’ gender, age, and living circumstances on Coronavirus infection symptoms and evaluate a relationship amongst symptoms of patients with Coronavirus infection. Method: In the present survey, the authors have adopted a quantitative survey method, relying upon face-to-face personal interviews, to receive information from the internal hospital consultant in Iraq. The span of data collection was three weeks. One hundred patients were randomly engaged in this research. The study was carried on special closed topics regarding the patients’ demographic data (age and gender) and some common signs of COVID-19 “sore throat, fever, shortness of breath, headache, dry cough, wet cough, arthralgia, as well as diarrhea”. Results: A sum of 100 cases participated in this research. The reliability value was (0.733). The Chi-Square test revealed no statistically substantial connection between symptoms of Coronavirus among cases and the patients' demographics data (gender and age). Furthermore, the Chi-Square test explained that there was no statistically vital connection amongst symptoms of cases of Coronavirus (shortness of breath & Dry cough, Sore throat & Dry cough, fever & headache, shortness of breath & sore throat) (p > 0.05). Nonetheless, there was a statistically significant correlation amongst symptoms of cases of Coronavirus (sore throat & wet cough, fever & diarrhea, shortness of breath & wet cough) (p < 0.05). Conclusion: There was a negligible influence of the age of the patient on the sharpness of symptoms. Besides, the symptoms of Coronavirus in males were not remarkably different from those in females. Nevertheless, there was a notable association between fever and diarrhea, wet cough and shortness of breath, and wet cough and sore throat.
Keywords: Coronavirus, demographic data, age, gender, symptoms.
Resumen: Antecedentes y objetivo: una nueva condición de COVID-19 surgió en diciembre de 2019 y ha tenido un pronóstico peligroso. Comenzó como una epidemia en China, particularmente en la ciudad de Wuhan. Las edades de las personas propensas a la infección varían desde un mes hasta más de 90 años. Sin embargo, se informaron menos casos en niños y recién nacidos. Las personas susceptibles a la infección son los ancianos, los que toman agentes inmunosupresores. Por lo general, el coronavirus presenta síntomas de la gripe, que incluyen fiebre (80-90%), tos seca (50%) y letargo (20-40%); otros síntomas incluyen diarrea. Esta encuesta tenía como objetivo evaluar el impacto del sexo, la edad y las circunstancias de vida de los pacientes en los síntomas de la infección por coronavirus y evaluar la relación entre los síntomas de los pacientes con infección por coronavirus. Método: En la presente encuesta, los autores han adoptado un método de encuesta cuantitativo, basándose en entrevistas personales cara a cara, para recibir información del consultor interno del hospital en Irak. El lapso de recopilación de datos fue de tres semanas. Cien pacientes participaron aleatoriamente en esta investigación. El estudio se llevó a cabo sobre temas especiales cerrados con respecto a los datos demográficos de los pacientes (edad y sexo) y algunos signos comunes de COVID-19 “dolor de garganta, fiebre, dificultad para respirar, dolor de cabeza, tos seca, tos húmeda, artralgia, así como Diarrea". Resultados: En esta investigación participaron un total de 100 casos. El valor de fiabilidad fue (0,733). La prueba de Chi-Cuadrado no reveló una conexión estadísticamente sustancial entre los síntomas del coronavirus entre los casos y los datos demográficos de los pacientes (sexo y edad). Además, la prueba de Chi-Cuadrado explicó que no había una conexión estadísticamente vital entre los síntomas de los casos de coronavirus (dificultad para respirar y tos seca, dolor de garganta y tos seca, fiebre y dolor de cabeza, dificultad para respirar y dolor de garganta) (p> 0,05)). No obstante, hubo una correlación estadísticamente significativa entre los síntomas de los casos de coronavirus (dolor de garganta y tos húmeda, fiebre y diarrea, dificultad para respirar y tos húmeda) (p <0.05). Conclusión: Hubo una influencia insignificante de la edad del paciente en la agudeza de los síntomas. Además, los síntomas del coronavirus en los hombres no fueron muy diferentes de los de las mujeres. Sin embargo, hubo una asociación notable entre fiebre y diarrea, tos húmeda y dificultad para respirar, tos húmeda y dolor de garganta.
Palabras clave: Coronavirus, datos demográficos, edad, sexo, síntomasact.
Introduction
A novel coronavirus infection disease 2019 (COVID-19) appeared in December of 2019, and it has a life-threatening prognosis1. It began as an epidemic in China, especially in Wuhan city.2but due to the rapid transmission of the disease, it was stated by WHO as a pandemic3. COVID-19 has reached almost every country worldwide in less than 24 weeks by travels and community contact.4
Although the initial cases of the coronavirus have been associated with the Huanan South China Seafood Market, the origin remains unknown. It was thought either a person-to-person transmission or maybe animal sources like a bat5.
The ages of people susceptible to infection range from a one-month-old to more than 90 years, but fewer cases were documented in children and infants6. Peoples most likely to infect are the elderly, those taking immunosuppressive agents. Individuals with hypertension are also at great risk7.
The incubation period of COVID ranges from 2 to 14 days8. Detection of the incubation period permits for precise monitoring and controlling of disease9.
The COVID-19 is transmitted by the expelled droplets during sneezing or speaking within a distance not exceeding two-meter, or by direct contact with exposed surfaces10.
Generally, COVID-19 has flu-like symptoms; including fever (80-90%), dry cough (50%), and lethargy (20-40%), other symptoms include diarrhea.
In some patients particularly the elderly, symptoms may lead to chest pain, pneumonia, and fatigue. Beyond approximately 7 days, it can progress to difficulty breathing, with 20% of patients needing hospital admission.
In approximately 5% of patients, COVID-19 rarely leads to a runny nose, sneezing, or sore throat. In China, 80.9% of patients with COVID-19 have mild symptoms; with flu-like symptoms; and recover at home without the need of hospital intervention. The percentage of death increases as getting older11.
When the virus, the single-stranded RNA-based virus, gets access via the mucus membranes, it enters the host cell utilizing type 2 transmembrane serine protease (TMPRSS2) and ACE2 receptor protein. This process leads to fusion and endocytosis with the host cell12-14. Then, the viral proteins are synthesized by the translation of virus RNA. With the help of RNA-dependent RNA polymerase, new RNA is produced for the new virions. After that, the affected cell undergoes lysis and releases a new virions load into the patients' body.
Massive pro-inflammatory cytokines were released, followed by the resultant infection, which causes a cytokine storm15. The cytokines storm results in changes that destroy the pulmonary tissue, leading to hypoxemia, which has a bad prognosis such as lymphopenia along with end-stage multiorgan failure and death16.
The Chinese health authority has declared that the whole number of confirmed infected cases in china has counted 76,936, from these cases, 2,442 people have died of the disease as of Feb 23 most of them were old and two-thirds were males, however, there is no detailed data has been reported17. In the Chinese series of studies, the mortality rate is 0.5% in patients younger than 50 years, 2% (50–59 years), 4% (60–69 years), 8% (70–79 years), and 16% (80 years)11. This suggests the question: Are men more vulnerable to acquiring worse symptoms and dying from COVID-19? Is the severity of symptoms increasing as get older?
So, this survey study aimed to evaluate the effect of patients’ gender and age on COVID-2019 infection symptoms and to assess if there is a correlation among symptoms of patients with COVID-19 infection.
In this study we used a quantitative survey methodology, depending on face-to-face personal interviews, to obtain data from the internal hospital consultant in Iraq. The duration of data collection was three weeks. 100 patients randomly participated in this study. The survey was included on specific closed questions about the patients’ demographic data (age and gender) and some general symptoms of COVID-19 “fever, headache, sore throat, dry cough, wet cough, shortness of breath, arthralgia, and diarrhea”.
Statistical analysis
SPSS-20 (IBM-USA) was applied to test the results. A descriptive content analysis was used to analyze the data of this study. Nonparametric statistics chi-square test was used to determine the independence of variables. Statistical significance was considered for P < 0.05.
Results
A total of 100 patients, 72 (72%) were male and 28 (28%) were female. In addition, most of the patients, (n=62, 62%) were aged 30-49 years while those with older age (70-89 years) constituted only 1% (n=1) of all patients table (1).
| Table 1. Demographic variables of study patients (n=100). | |
| Variables | Patients no. (%) |
| Gender | |
| Male | 72 (72) |
| Female | 28 (28) |
| Age (years) | |
| 10-29 | 18 (18) |
| 30-49 | 62 (62) |
| 50-69 | 19 (19) |
| 70-89 | 1 (1) |
Cronbach alpha was applied to detect the reliability of this study. Its value was (0.733), indicating that the survey study is highly reliable, accurate, and stable.
Results of the Chi-Square test showed that there was no statistically significant association between symptoms of COVID-19 disease among patients and the patient's demographics data (gender and age) since Chi-Square had a p-value (0.911, 0.989) respectively > 0.05 (p < 0.05), Table 2 and 3.
| Table 2. Chi-Square test results for symptoms of COVID-19 and patients’ gender (n=100). | |||||
| Symptoms | Gender | Total patients, n (%) | P-value | ||
| Male, n (%) | Female, n (%) | 0.911 | |||
| Fever | 59 (70.2) | 25 (29.8) | 84 (84) | ||
| Headache | 53 (65.4) | 28 (34.6) | 81 (81) | ||
| Sore throat | 54 (77.1) | 16 (22.9) | 70 (70) | ||
| Cough | Wet cough | 26 (30.2) | 11(12.8) | 86 (86) | |
| Dry cough | 34 (39.5) | 15 (17.4) | |||
| Shortness of breath | 41 (69.5) | 18 (30.5) | 59 (59) | ||
| Arthralgia | 43 (68.3) | 20 (31.7) | 63 (63) | ||
| Diarrhea | 31 (72.1) | 12 (27.9) | 43 (43) | ||
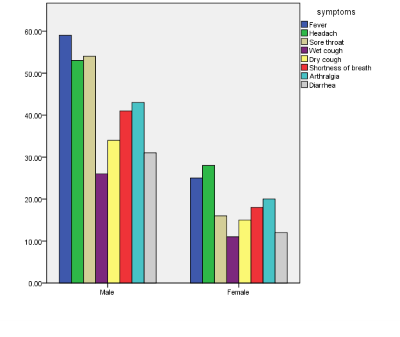
Figure 1.
Chi-Square test results for symptoms of COVID-19 and patients’ gender.
| Table 3. Chi-Square test results for symptoms of COVID-19 and patients' age (n=100). | |||||||
| Symptoms | Age | Total patients, n (%) | P-value | ||||
| 10-29n (%) | 30-49n (%) | 50-69n (%) | 70-89n (%) | 0.989 | |||
| Fever | 16 (19) | 52 (61.9) | 15 (17.9) | 1 (1.2) | 84 (84) | ||
| Headache | 14 (17.3) | 52 (64.2) | 14 (17.3) | 1 (1.2) | 81 (81) | ||
| Sore throat | 12 (17.1) | 48 (68.6) | 10 (14.3) | 0 (0) | 70 (70) | ||
| Cough | Wet cough | 5 (5.8) | 23 (26.7) | 8 (9.3) | 1 (1.2) | 86 (86) | |
| Dry cough | 12 (14) | 30 (34.9) | 7 (8.1) | 0 (0) | |||
| Shortness of breath | 13 (16.9) | 53 (68.8) | 10 (13) | 1 (1.3) | 59 (59) | ||
| Arthralgia | 13 (20.6) | 38 (60.3) | 11 (17.5) | 1 (1.6) | 63 (63) | ||
| Diarrhea | 8 (18.6) | 31 (72.1) | 4 (9.3) | 0 (0) | 43 (43) | ||
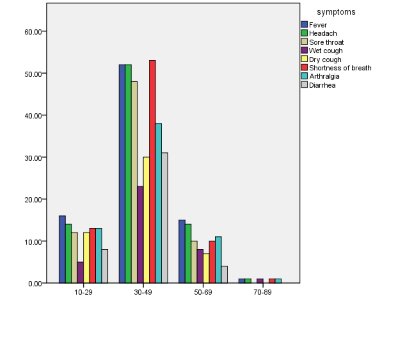
Figure 2.
Chi-Square test results for symptoms of COVID-19 and patients age
Results of the Chi-Square test showed that there was no statistically significant association among symptoms of patients of COVID-19 disease in each respective group (fever & headache, Sore throat & Dry cough, shortness of breath & Dry cough, Shortness of breath & sore throat) since Chi-Square had a p-value (0.815, 0.054, 0.336, 0.333) respectively but there was a statistically significant association among symptoms of patients of COVID-19 disease in each group (fever & diarrhea, sore throat & wet cough shortness of breath & wet cough) since Chi-Square had p-value (0.000, 0.001, 0.025) respectively < 0.05 (p < 0.05), Table 4.
| Table 4. Chi-Square test showed non-significant results among patients' symptoms of COVID-19 (n=100). | ||||
| Symptoms | Total patients, n (%) | Symptoms | Total patients, n (%) | p-value |
| Fever | 84 (84) | Diarrhea | 43 (43) | 0.000 |
| Headache | 81 (81) | 0.815 | ||
| Sore throat | 70 (70) | Wet cough | 37 (37) | 0.001 |
| Dry cough | 49 (49) | 0.054 | ||
| Shortness of breath | 59 (59) | Wet cough | 37 (37) | 0.025 |
| Dry cough | 49 (49) | 0.336 | ||
| Sore throat | 70 (70) | 0.333 | ||
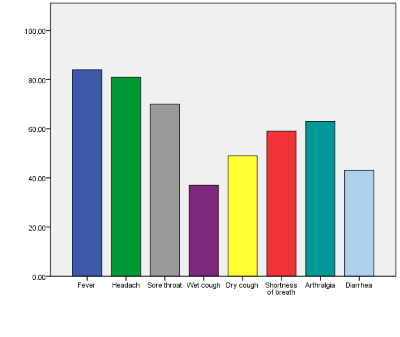
Figure 3.
Discussion
This study was complemented pointing at assessing the effect of age and gender on symptoms of COVID 19 infection among all 100 patients in Babylon province tested between September 27 and October 20, 2020. In addition, it had evaluated the prevalence and correlation among symptoms. We established that a total of 72% of these patients who were detected with clinical COVID-19 were male and 28% were female. Our findings provoked that most of the patients were aged 30-49 years.
Based on our study, the most abundant symptoms among the patients were cough (86%), fever (84%), headache (81%), sore throat (70%), and (63%) arthralgia. Moreover. Only 43% of patients suffered from diarrhea. Our results are harmonious with previous reports provoking that most of the COVID-19 diagnosed patients had cough and fever18. We found that the age and gender of patients did not affect the manifestations of the disease (Chi-Square had a p-value greater than 0.05 for age and gender) and this finding did not consistent with a previous study which was indicated that the males had a worse prognosis of COVID-19 than females. Mainly due to estrogen having a protective effect against inflammation19,20. Moreover, older people were more prone to adverse outcomes of COVID-1921. Our study viewed that patients who suffered from fever accompanied with diarrhea (Chi-Square was 0.0001). However, Diarrhea was the most frequently confirmed GI symptom of COVID-19 owing to the presence of the target receptor for SARS-CoV-2 which was Angiotensin-converting enzyme II (ACE-2) in the gastrointestinal tract22. Several previous reports provoked that most coronaviruses diagnosed patients presented with fever which pointed to the location of the target cells in the lower airway23,24. Our study assessed that there was a significant correlation between a symptom of wet cough and shortness of breath and wet cough and sore throat (Chi-Square were 0.025 and 0.001 respectively). It is worth pointing that the wet cough and shortness of breath were the pulmonary symptoms of COVID-19. The consequences of the entry of the SARS-CoV-2 virus to the alveolar cells (type I & II) through ACE-2 receptors were a cascade of pro-inflammatory cytokines motivation25,26.
This study has some limitations. First, it included only 100 patients. Second, only 72 males and 28 females were included for assessing the effect of gender on symptoms of COVID 19 infection. Third, only one patient aged (70-89) was included in this study. This was because of the urgent circumstances and the seriousness of direct contact with COVID-19 infected patients to collect more data. It could affect the analysis s and any possible outcomes. Therefore, more clinical and vital researches considering the assessment of the effect of gender and age on symptoms of COVID 19 infection is required in the future.
Conclusion
This study postulates an indication of the prevalence of the COVID-19 outbreak. The useful screening method for the diagnosis of COVID-19 is the symptoms. Most patients suffered from cough, fever, headache, and sore throat. Moreover, some patients suffered from diarrhea. There was an insignificant impact of the age of the patient on the severity of symptoms. Furthermore, the symptoms of COVID-19 in males were not noteworthy diverse from that in females. However, there was a significant correlation between fever and diarrhea, wet cough and shortness of breath, and wet cough and sore throat.
References
1. Rodriguez-Morales AJ, Bonilla-Aldana DK, Balbin-Ramon GJ, Rabaan AA, Sah R, Paniz-Mondolfi A, et al. History is repeating itself: probable zoonotic spillover as the cause of the 2019 novel coronavirus epidemic. Infez Med. 2020; 28:3–5.
2. Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. China Novel Coronavirus Investigating and Research Team, A novel coronavirus from patients with pneumonia in China, 2019, N. Engl. J. Med. 2020;382 (8):727–733.
3. World Health Organization. https://www.who.int/dg/speeches/detail/whodirector- general-s-opening-remarks-at-the-mission-briefing-on-covid-19—12-march-2020. (accessed May 16, 2020).
4. Dong E, Du H, Gardner L. An interactive web-based dashboard to track COVID-19 in real-time. Lancet Infect Dis:2020;20:533–534.
5. Zhou P, Yang X-L, Wang X-G, Hu B, Zhang L, Zhang W, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin, Nature. 2020;579(7798):270–273.
6. Dong Y, Mo X, Hu Y, Qi X, Jiang F, Jiang Z, et al. Epidemiology of COVID-19 among children in China. Pediatrics. 2020;145(6):e20200702
7. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 Novel Coronavirusinfected pneumonia in Wuhan, China. JAMA. 2020;323:1061–1069.
8. Backer JA, Klinkenberg D, Wallinga J. Incubation period of 2019 novel coronavirus (2019-nCoV) infections among travelers from Wuhan, China, 20–28 January 2020. Eurosurveillance. 2020;25:2000062.
9. Lauer SA, Grantz KH, Bi Q, Jones FK, Zheng Q, Meredith HR, et al. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: estimation and application. Ann Int Med. 2020;172:577–582.
10. Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382:727–33.
11. Ortiz-Prado E, Simbaña-Rivera K, Gómez- Barreno L, Rubio-Neira M, Guaman LP, Kyriakidis NC, et al. Clinical, molecular, and epidemiological characterization of the SARS-CoV-2 virus and the Coronavirus Disease 2019 (COVID-19), a comprehensive literature review. Elsevier. 2020; 98:115094.
12. Fehr AR, Perlman S. Coronaviruses: An overview of their replication and pathogenesis. In: Coronaviruses: Methods and Protocols (New York: Springer). 2015;1282:1-23.
13. Chen Y, Liu Q, Guo D. Emerging coronaviruses: Genome structure, replication, and pathogenesis. J Med Virol. 2020;92:418–23.
14. Hoffmann M, Kleine-Weber H, Schroeder S, Mü MA, Drosten C, Pö S. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020;181:271–80.
15. Cheng VCC, Chan JFW, To KKW, Yuen KY. Clinical management and infection control of SARS: Lessons learned. Antiviral Res. 2013;100:407–19.
16. Sun X, Wang T, Cai D, Hu Z, Chen J, Liao H, et al. Cytokine storm intervention in the early stages of COVID-19 pneumonia. Cytokine Growth Factor Rev. 2020;53:38–42.
17. Jin, J. M. et al. Gender Differences in Patients With COVID-19: Focus on Severity and Mortality. Frontiers in Public Health8, (2020).
18. Lan F-Y, Filler R, Mathew S, Buley J, Iliaki E, Bruno-Murtha LA, et al. COVID-19 symptoms predictive of healthcare workers’ SARS-CoV-2 PCR results. PLoS ONE. 2020;15(6): e0235460.
19. Haitao T, Vermunt JV, Abeykoon J, Ghamrawi R, Gunaratne M, Jayachandran M, et al. COVID-19 and Sex Differences: Mechanisms and Biomarkers. Mayo Clin Proc. 2020;95(10):2189-2203.
20. Medina KL, Strasser A, Kincade PW. Estrogen influences the differentiation, proliferation, and survival of early B-lineage precursors. Blood. 2000;95(6):2059-2067.
21. Mohamed MO, Gale CP, Kontopantelis E, Kontopantelis E, Doran T, de Belder M, et al. Sex Differences in Mortality Rates and Underlying Conditions for COVID-19 Deaths in England and Wales. Mayo Clin Proc. 2020;95(10):2110-2124.
22. Sultan S, Altayar O, Siddique SM, Davitkov P, Feuerstein JD, Lim JK, et al. AGA Institute Rapid Review of the Gastrointestinal and Liver Manifestations of COVID-19, Meta-Analysis of International Data, and Recommendations for the Consultative Management of Patients with COVID-19. Gastroenterology. 2020;159(1):320-334.
23. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497-506.
24. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA. 2020;323(11):1061-1069.
25. Conti P, Ronconi G, Caraffa A, Gallenga CE, Ross R, Frydas I, et al. Induction of pro-inflammatory cytokines (IL-1 and IL-6) and lung inflammation by Coronavirus-19 (COVI-19 or SARS-CoV-2): anti-inflammatory strategies. J Biol Regul Homeost Agents. 2020;34:1.
26. Johnson KD, Harris C, Cain JK, Hummer C, Goyal H, Perisetti A. Pulmonary and Extra-Pulmonary Clinical Manifestations of COVID-19. Front Med (Lausanne). 2020;7:526.