Artículos
Attitude impaction of information and perception to digital dental practices in respect to coronavirus outbreak
Impacto de la actitud de la información y la percepción de las prácticas dentales digitales con respecto al brote de coronavirus
Attitude impaction of information and perception to digital dental practices in respect to coronavirus outbreak
Archivos Venezolanos de Farmacología y Terapéutica, vol. 40, núm. 8, pp. 811-817, 2021
Sociedad Venezolana de Farmacología Clínica y Terapéutica

Esta obra está bajo una Licencia Creative Commons Atribución-SinDerivar 4.0 Internacional.
Recepción: 28 Junio 2021
Aprobación: 15 Agosto 2021
Publicación: 30 Noviembre 2021
Abstract: Objectives: Objectives: The study's main aim is to assess the deep understanding and perception of dental practices to manage the digital facilities against coronavirus. Methods: A structured survey was assigned to all dentists practicing an online link Google form and transferred via Facebook, Viber, Telegram, and what's app official dental/ medical faculty groups for 3-months from 13 February to 13 May 2020. The questionnaire examined members’ awareness regarding coronavirus results, patient identification from the orofacial exhibition as a presumption control measure then understanding of dental staff to proper digital valuability. The statistical analysis was conducted utilizing simple SPSS Statistics V22.0 (IBM Corp., Armonk, NY, USA). Results: A sum of 250 participants answered the questionnaire. Overall, the awareness was beneficial with some distinct responses in control measures against quickening of outbreak ultimately. Nevertheless, coronavirus appeared extremely important and pandemic. Still, the attention toward adopting digital facilities in dental practices was critical and proportionate with overall understanding of the route of transmission, patient protections, and quality development protocols to lessen the chance of an outbreak in the dental practice area. The awareness was acceptable because of an efficiency of 60% and a validity of 45% scores to save time and cost in dropping COVID-19 outbreak. Conclusion: Best dental health care instructions rely on control measures of understanding and knowledge of dental practices workforce. Educational operations need to concentrate on those two concepts given special attention by logical activation of the digital dental workflow instead of traditional, particularly in times of crisis like coronavirus.
Keywords: Perception, Coronavirus, Digital Dentistry, knowledge.
Resumen: Objetivos: El objetivo principal del estudio es evaluar el conocimiento profundo y la percepción de las prácticas dentales para gestionar las instalaciones digitales contra el coronavirus. Métodos: Se asignó una encuesta estructurada a todos los dentistas que practican un enlace en línea de Google y se transfirió a través de Facebook, Viber, Telegram y los grupos oficiales de facultades dentales / médicos de What's App durante 3 meses desde el 13 de febrero hasta el 13 de mayo de 2020. El cuestionario examinó la conciencia de los miembros con respecto a los resultados del coronavirus, la identificación del paciente de la exposición orofacial como una medida de control de presunción y luego la comprensión del personal dental para la valuación digital adecuada. El análisis estadístico se realizó utilizando SPSS Statistics V22.0 simple (IBM Corp., Armonk, NY, EE.UU.). Resultados: Un total de 250 participantes respondieron el cuestionario. En general, la conciencia fue beneficiosa con algunas respuestas distintas en las medidas de control contra la aceleración del brote en última instancia. Sin embargo, el coronavirus parecía extremadamente importante y pandémico. Aún así, la atención hacia la adopción de instalaciones digitales en las prácticas dentales fue crítica y proporcionada con la comprensión general de la ruta de transmisión, las protecciones del paciente y los protocolos de desarrollo de calidad para disminuir la posibilidad de un brote en el área de la práctica dental. La consciencia de que somos aceptables debido a la eficiencia del 60% y las puntuaciones de validez del 45% para ahorrar tiempo y costos en la eliminación del brote de COVID-19. Conclusión: Las mejores instrucciones para el cuidado de la salud dental se basan en medidas de control de comprensión y conocimiento de la fuerza laboral de las prácticas dentales. Las operaciones educativas deben concentrarse en esos dos conceptos a los que se les presta especial atención mediante la activación lógica del flujo de trabajo dental digital en lugar de los tradicionales, particularmente en tiempos de crisis como el coronavirus.
Palabras clave: Percepción, Coronavirus, Odontología digital, conocimiento.
Introduction
In early March 2019, The SARS-CoV-2 has started behaving a lot like the once-in-a-century pathogen worldwide population has been worried about. Therefore, The Director-General of the World Health Organization declared COVID-19 a novel global pandemic on 11 March 20201.
Novel (COVID-19) is genetically more like SARS-CoV than MERS-CoV. This fact highlights the epidemiology and pathogenesis of these viruses, including our current analysis of knowledge, attitude, and awareness base on their characteristics, transmission, and recommendations. Also, there is strong evidence that it can be transmitted by people who are just mildly ill or even pre-symptomatic somewhat like beta-coronavirus Middle East respiratory syndrome MERS and severe acute respiratory syndrome SARS. However, COVID-19 is still attacking much harder and is spread much more efficiently and pandemically. In fact, COVID-19 has already caused 10 times as many cases as SARS in a quarter of the time2 (Figure 1).
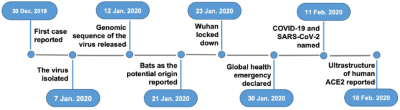
Figure 1.
Major events that occurred thus far during the outbreak of COVID-19
Upon activation of national pandemic preparedness and response strategies, a dedicated multi-disciplinary national crisis team should be established with clear lines of crisis management scheme based on public health risk assessments that motivate and evaluate the readiness of the public health system to implement the response measures in a collaboration plan.
As always happens, healthcare professionals have been immediately involved in the national emergency, and daily work clinic in routine health care demands. Unfortunately, dentists are often the first line of attack in an asymptomatic patient or even to an early infected patient, as they work in close contact with patients. To emphasize that facts, on 15 March 2020, the New York Times published an article entitled “The Workers Who Face the Greatest Coronavirus Risk”, where an impressive schematic figure described that dentist are the workers most exposed to the risk of being affected by COVID-19, much more than nurses and general physicians3 (Figure 2).

Figure 2.
The high-risk dentist that faces the COVID-19 attack.
As stated before, it is essential to give a clear idea about dental practice attitude and easy guidelines to manage dental patients with more awareness against COVID-19 attack. Dental professionals should be familiar with better knowledge based on evidence of how COVID-19 is spread, how to identify patients with COVID-19 infection, and what extra-protective measures should be adopted during the practice, to prevent the transmission of COVID-19. There are recommended basics in the infection control measures that should be followed by dental professionals, particularly because aerosols and droplets were considered as the main spread routes of COVID-19. This recommendation is a special release by the National Health Commission of the People’s Republic of China, and the practice experience in West China Hospital of Stomatology related to the outbreak of 2019-nCoV transmission.4(Figure 3).

Figure 3.
Major routes of the COVID-19 and control in dental practice.
Dental care practices are deeply concerned by the alarming levels of spread and monitoring the severity of the outbreak. They also expressed concern about the alarming levels of impaction of Medical/dental practice in a manner. Therefore, this assessment survey that COVID-19 can be characterized as a pandemic, to overwhelm these targets. Recently, to take significant actions against this harmful disease, an interesting paper written by researchers from Wuhan University School and Hospital of Stomatology was published with several recommendations for dentists and dental students to manage COVID-19 patients5.
A demographic study in late December of 2019 showed that the percentages of the clinical manifestations and symptoms were 98% for fever, 76% for dry cough, 55% for dyspnea, and 3% for diarrhea; 8% of the patients required ventilation support.23 Similar findings were reported in two recent studies of a family cluster and a cluster caused by transmission from an asymptomatic individual6.
So, dentists have been recommended to take several personal protection measures and avoid or minimize operations that can produce droplets or aerosols. Since the viral load contained in the human saliva is very high, rinses with antiseptic mouthwashes can only reduce the infectious amount but are not able to eliminate the virus in the saliva7.
The coronavirus pandemic will strain many healthcare sectors, including radiology. Radiographical films such as CBCT/ Extraoral/ Intraoral radiographs are an acceptable source of infection especially with analog film rather than digital film. Radiologists have been conscripted to the front line because COVID-19 has a chest computed tomography (CT) imaging signature befitting of viruses that damage lungs. But CT can be normal in early illness, and after each potentially infected patient is scanned, the machine must be completely disinfected. Therefore, CT isn't recommended to screen for COVID-198.
Nowadays, A computer-aided digital dental design/ manufacturing indicated technology is widely used since it is more comfortable for patients with more accuracy of workflow and high-value quality than conventional workflow. Significantly digital dental technology reduces the costs (about 30%) with more active working time in 90%. Exclusively, the term of aesthetic and more biocompatible materials and the flexibility to manufacture from simple to complex dentofacial and/or orthodontic appliances.
Obviously, a significant innovation of virtual technology promotes excessive business targets and improves eco-friendly dentistry. Despite the high interest in dentistry on digital dentistry nowadays, gold standard guidelines for infection prevention did not pay attention to it9.
Concurrently, insufficient notes a re-available from Laws on health safety and guidelines for using digital dental practices, the usually reported advantages for infection prevention are the nonrequirements of disinfection and better occupational safety10,11.
Education-related challenges for medical and dental schools, as well as their affiliated hospitals, are significant. It was reported that open communication among students, clinical teachers, and administrative staff would enhance mutual trust and facilitate adequate cooperation. Based on our experience with SARS and relevant highly pathogenic infectious disease, we provide a few basic recommendations for dental education during an outbreak: First, during the outbreak period, online lectures, case studies, and problem-based learning tutorials should be adopted to avoid unnecessary aggregation of people and associated risk of infection12.
Some previous studies assessed the knowledge and awareness measure against MERS-COV, SARS-COV among health professions students, dental students, and dentists for disease control strategies in some countries13-16.
This is a critical time for information but also for the support and reassurance that science and evidence can offer. However, what actions do we know are effective in pandemics, and does social distancing truly make a difference in an outbreak, and what have we learned about COVID-19 that can inform how we prepare and respond in our daily lives. All these real questions were reported by experts from the Johns Hopkins Bloomberg School of Public Health19.
Updating the information on current COVID-19 knowledge and Increasing awareness toward beneficial use of advanced digital dental workflow among dentists on a wider scale in the country is needed to identify existing gaps and set ideal measures to address training deficiencies. Moreover, it is important to develop awareness toward more creative facilities that enforce quality of workplace output within the scheduled time and acceptable cost especially in a crucial time of crisis or disaster like the COVID-19 outbreak.
To our knowledge, this is the first paper that focuses on the COVID-19 attack in detail using digital workflow rather than traditional dentistry. Here, we report three specific concepts of study orientation toward problem-solving related to sufficient guidelines for recognition of dental practices knowledge, attitude, and awareness regarding the COVID-19 outbreak.
Materials and Methods
A cross-sectional survey was conducted for 3 weeks from 13-March 2020 to 31-April 2020 at Al-Farahidi University, Baghdad, Iraq.
Questionnaire Design
A 21-item structured questionnaire was developed using the style and format of some of the questions used in previous studies.13-16 The questionnaire was designed to evaluate all dental concepts implementations and perceptions of COVID-19 attack in dental health care. However, the questionnaire was developed in the English language as this is the official scientific language at all healthcare faculties and institute in Iraq and almost all the world. The questionnaire was designed for this study among small, selected participants (n=10) of various dental and health care workers. The presentation and validity of the questionnaire were undertaken by experienced academic and senior pharmacy students.
The study questionnaire comprised four sections containing 21 items. First Section: had four items that explored the general information of respondents including age, gender, residency area, and degree of health practices.
Second Section: comprised ten items and was categorized to evaluate participants' in-depth knowledge about COVID-19 including topics of causes, ways of transmission, mortality, morbidity, prevention measures, and high-risk groups for COVID-19. The knowledge was focused on four means (prevalence, mortality, treatment therapy, toplist risk group). A high-risk group was restricted for dental and non-dental practice manpower in both academic and clinical attachment regions such as WHO and CR employees. An incomplete assessment already was not submitted and omitted from the survey. A maximum knowledge of ten items was obtainable in this section.
Third Section: comprised 9 items but divided into 2 subdivisions; First subdivision aimed to gather participants' sources of knowledge about COVID-19 by 5 items. Generally, this subdivision emphasized the preventive measures and their maintenance roles among diverse dental practices against COVID-19. The second subdivision comprised 4 questions and aimed to evaluate participants' attitudes and perspectives of awareness toward digital dentistry to interpret all control strategies about COVID-19. All questions were designed based on topics of "Importance of Digital Imaging, Validity of Digital Dentistry in the workplace, Valuable use of Digital Dental workflow in the workplace, Accuracy of Digital Dental workflow in the workplace" regarding crisis time. The questionnaire was prepared and shared using Google Forms.
Questionnaire distribution and data collection
Undergraduate dentistry students, dental juniors, dental seniors, and health care practice volunteers were approached and recruited through social channel groups (Facebook, Viber, and Whats'up). Students were eligible to participate if they were in years 3, 4, 5 of their undergraduate programs. The password-protected survey links were shared on various official college social media pages and groups. A preliminary paragraph highlighting the aims and scopes of the study as well as instructions to fill the questionnaire was posted along with the survey.
Statistical analysis
The data were coded, entered, and analyzed using SPSS. Descriptive statistics, frequencies, and percentages were used to summarize the data. An ANOVA test was used to determine the association of study disciplines with both Knowledge and Awareness of dental staff on COVID-19. P<0.05* was considered statistically significant.
Results
Demographics and characteristics of participating students
A total of 250 participants were assessed during the study. The majority (73.3%) of the participants were under the 25-year age group. More than two-thirds (68.9%) were dental students followed by dental juniors (2.2%). Most (73.3%) were 3rd, 4th, and 5th academic year students in dental faculties a world. Just a 17.8% of the participants had a non-dental (healthcare) in the dental workplace and meanwhile at least 11.1% were dental senior. Additionally, most of the study participants were academic workers (80%) rather than (20%) in the clinical attachment of WHO and CR. Over half of the participants were female (57.8) whereas 42.2% participants were male (Table 1).
| Table 1. General information of participants in the study (N=423). |
| Factors n (%) |
| -Age |
| <25 years 132 (73.3) |
| 25+ years 48 (27.7) |
| -Gender |
| Male 104 (57.8) |
| Female 76 (42.2) |
| -Residency |
| Iraq 156 (84.5) |
| Aboard 24 (15.5) |
| -Specialty* |
| Dental Students 124 (68.9) |
| Dental Practice 4 (3.2) |
| Dental Senior 20 (11.1) |
| Non-Dental Senior 32 (17.8) |
| -Nature of practice* |
| Academic 144 (80) |
| Clinical (MOH & CR) 36 (20) |
| *Number does not add up to total due to item non-response. MOH - Ministry of Health, and related CR - clinical relatives. |
Preventive measure and epidemiology knowledge about COVID-19
Overall, prevalence measures such as facemask, gloves, and protective eyeglass achieved significantly better scores 88.9% than protective diet 37.8% or therapeutic means 46.7% of study disciplines, respectively. However, weather factor seemed with least significant value than illiteracy and health baseline facilities to increase pandemiology (p<0.0001). Near to half (42.2%) of the participants were aware that COVID-19 is increased by the illiteracy of the community followed by unexpected virus attacks (33.6%).
More than two-thirds 73.3% of the participants believed that COVID-19 can be transmitted through direct or indirect contact with no significant mention to stress score in transmission increase (Table 2). Regarding preventive strategies for COVID-19, the majority near to (90%) of the participants most significantly believed that the Dental student's first-line attack (p<0.0001*) through monitoring of high-risk group. Furthermore, 57.8% stated that maintaining drugs can also be curable in decreasing the mortality rate (Table 2).
| Table 2. Factors associated with control measures and Epidemiology. |
| Factors CoR* CI* 90% 95% 99% P* value |
| Pandemiology 0.3 (0.15 , 0.6) (0.13 , 0.69) (0.1 , 0.9) 0.001* |
| Prevalence 1.1 (0.42 , 2.91) (0.35 , 3.5) (0.24 , 5.04) |
| Mortality rate 0.36 (0.1 , 1.31) (0.08 , 1.68) (0.05 , 2.72) |
| First line attack 0.81 (0.48 , 1.35) (0.44 , 1.49) (0.36,1.8) 0.001* |
| Vaccine 1.06 (0.59 , 1.87) (0.53 , 2.09) (0.43 , 2.59) |
| CoR= Confidential relation, CI= Correlation Interval, P value < 0.001 * |
Awareness toward dental practice workflow
Most of the participants 66.7% strongly agreed that preparatory investigation either lab test RT-PCR (33.3%) or other all diagnostic measures (33.3%) about COVID-19 is important to prevent the spread the disease. Furthermore, just over half (53%) of the participants expressed their level of concern about COVID-19 by strongly relating to dentists or nurses. Whereas physician (15.6%) seems on last of the top list after laboratory staff (22.2%). Although, dentists appeared statistically high-risk related groups but in different ratios. Indeed, dental surgeons cited on the top list (42.2%) of dental practice specialty that they are more susceptible to attack with COVID-19 than periodontists (28.8%) subsequently. Progressively near to half of the scores, dental students (48.4%) were cited as most susceptible maneuvers in the dental workplace than all others to COVID-19 attack. Furthermore, A statistically most significant oral manifestation was reported, is sore throat than temporomandibular joint (TMJ) arthralgia is least significant among study discipline score (p<0.0001) (Table 3)
| Table 3. Dental staff Knowledge regarding prevention and high-risk groups |
| Questions manner Yes, n (%) |
| -What do you suspect Oral Manifestation of COVID 19 |
| Myofascial pain 16 (8.9) |
| Sore throat 64 (35.6) |
| Dry mouth 52 (20) |
| TMJ arthralgia 12 (28.9) |
| All symptoms 36 (6.7) |
| -how a preparatory dental practice detection of COVID-19 |
| Lab test RT-PCR (mRNA) 60 (33.3) |
| Radiological test 8 (4.4) |
| Both lab. & Radio. test 36 (20) |
| Clinical test 16 (8.9) |
| All 60 (33.3) |
| -Who of medical staff is on the top list of contact with COVID-9 |
| Physician 28 (15.6) |
| Dentist 60 (33.3) |
| Nurse 52 (28.9) |
| Laboratory Staff 40 (22.2) |
| -Who is most susceptible in dental specialty |
| Surgeon 76 (42.4) |
| Prosthodontist 36 (20) |
| Periodontist 52 (28.9) |
| Radiologist 16 (8.9) |
| -Who is a High-risk group of dental practice |
| Dental student 84 (46.7) |
| Dental assistant 16 (8.9) |
| Dental junior 40 (22.2) |
| Dental senior 40 (22.2) |
| -What is the limit of maintenance in dentistry to do |
| Infection control 52 (28.9) |
| Diagnosis 28 (15.6) |
| Innovation (3D digital) 4 (2.2) |
| All 96 (53.3) |
Attitude to advanced digital dentistry impaction
Attitude certainty was very clear toward the Digital Dentistry concept through four disciplines of scope which are importance, validity, valuability, and accuracy terms. Remarkably, more than half (51.1%) of questioner Score line schemed a Dentofacial imaging Cone Beam Computed Tomography (CBCT) significantly is a better protocol than all other (48.9%) in detection strategy, respectively. However, the participants selected different scopes of digital dentistry implementation, the infection control seemed mostly interested in both direct and indirect view of application by 13.3% (p <0.0001*). Meanwhile, very few (2.2%) of the participants refused a digital dentistry interpretation intentionally whereas, more than a third (40%) of participants scored to fully digital dentistry implementation in dental health care progressively.
Moreover, near to half (44.3%) of the participants believed that use of digital advanced technology in dental workflow impact positively in both insurance of patient’s modality and workflow accuracy then subsequently reduce time and manpower demand in all dental disciplines, especially at crisis times like COVID-19 outbreak (Table 4)
| Table 4.Awareness Certainty toward Digital Dentistry Concept, n (%) |
| N (%) Certain, Neutral, Probable Disagree |
| Dentofacial Radiograph Imaging importance in the workplace |
| 92 (51.1) 60 (33.3) 16 (8.9) 12 (6.7) |
| Validity of Digital Dentistry Validity in the workplace |
| 124(68.9) 24 (13.3) 24(13.3) 8 (4.4) |
| Valuable use of Digital Dental workflow in the workplace |
| 72 (40) 68 (37.8) 36 (20) 4 (2.2) |
| Accuracy of Digital Dental workflow in the workplace |
| 80 (44.4) 56 (31.1) 32 (17.8) 12 (6.7) |
Discussion
The participants in this study had a different higher education level according to their level in dental school or health care and were mainly female (58.7%), which indicates that females are more concerned with medical outbreaks of the disease than males. Moreover, most participants 84.8% were from Baghdad province and more than two-third 69.6% were dental students of all participants. Briefly, a high score of knowledge was given to the control mean of COVID-19 prevalence, protection, and control measures that COVID-19 is an airborne pathogen, 54% recognized the symptoms, and 48% realized that the probable source of COVID-19 virus is camels, while 64% were aware of the way of spreading by close contact and 79% knew instructions and measures for protection. However, most of the participants in this study cited social media as their source of information for COVID-19. Study participants’ increased use of and access to the internet to seek information have also been reported in previous studies conducted in Saudi Arabia13-16.
The World Health Organization (WHO) and the Ministry of Health in all worldwide countries provided continuously all educational posts or media programs on infection control18. Such educational programs can be a very useful source for providing information to both the public and various healthcare professionals. Similarly, online webinars, sessions, and research papers can also be effective in raising awareness about COVID-19 and other emerging infectious diseases13-16.
Attitudes toward knowledge of control measures
A clustering in crowded places, ignoring health measures and direct contact is considered the major route of COVID-19 transmission. Participants identified that close contact with a patient of COVID-19 is one of the main routes of spreading the virus (71.7%). Also, a high proportion (89.9%) of participants was aware of the instructions of protection, and obviously near half of them (43.5%) toward the spreading of the virus by ignorance of the population. So, this indicates that the information related to the way of contamination and spreading of COVID-19 and the measure for protection is well known13,18,19.
Perception’s availability of awareness towards digital dental workflow
A third proportion of the participants (32.3%) expressed their apprehension about toplist risk opportunity from health care by stating that dentists are highly susceptible due to their clinical close relation (47.8%) with saliva droplet in touch (15.3%) without a clear infection COVID-19 on control isolation policy. This concern seemed by participants in this study also reflects their awareness about pathogen transmission18. Transmission of COVID-19 infection from infected patients to healthcare professionals has been confirmed in previous studies28,30. The European center for disease prevention and control (ECDC) scientific advisory council has developed COVID-19 guidelines for the safer management of COVID-19 infected patients. These guidelines have also clearly outlined the isolation procedures and precautions for the control of COVID-19 infection. All healthcare facilities worldwide including the dental care region should therefore strictly adhere to these policies to ensure the protection of not only the public but also healthcare workers19.
Even though, near to third of participants (32.3%) mentioned a dentist as a top list of high-risk health care personnel but stated in different proportions. Surgeons are located more closer to attack (43.5%) than another dental staff specialty due to their situation in emerging cases and hospitalization. In addition, the radiologist was reported as the least dental practitioner susceptible to direct contact. That indicates the initial response of participants' awareness towards digital dental facilities like CBCT more than others20.
The dental students achieved a better COVID-19 knowledge score (69.9%) than their counterparts. This difference may be explained by the selection of dental students as the most susceptible (47.8%) than other dental care staff. Indeed, that fact is real because dental students have more clinical attachments than others and therefore have direct contact with the patients more than other participants. Furthermore, dental students have often engaged themselves in more public health campaigns that provide them as volunteers with opportunities to improve their knowledge and maybe decrease the gap of health care disaster time about potentially epidemic infectious diseases such as COVID-1917.
Accordingly, there is a need to provide motivation courses to students from other health disciplines to improve their awareness and enforce them of various urgent infection trends and their available infection control policies and procedures13-16.
However, the majority of participants (71.7%) were aware of the measures adopted for protection and 50% knew that COVID-19 (89.9%) is contagious, and therefore, it is very important to apply all maintenance levels of dentistry discipline preliminary from infection control, diagnosis to the innovative workflow by digital facilities than conventional work, which is more hazardous in work and time21,22.
Near 70% of participants accepted different scopes of digital dentistry baseline to enclose all dental workflow advantages and should be subjected to encounter all dental disciplines with accurate, clear, and valuable work. Certainly, all the advantages of the digital dental workflow are more on-demand subsequently especially in our defense against COVID-19 outbreak23.
From the results of this survey, it is very encouraging to conclude that our dental practices especially dental students had good knowledge of COVID-19 (etiology, symptoms, protection) and thus reflect the successful motivation of participants toward the awareness about digital dentistry in the academic and clinical workplace. More awareness of COVID-19 hazards is related to conventional workflow with dental material and saliva contamination by dental staff who are the first people in contact with patients infected by the COVID-19 24.
Conclusion
Our data indicate the necessity for further continuing education among dental staff, as well as improving more public education about digital dentistry awareness for all dental care staff especially old fashion-dental practices.
Despite this study having some limitations, it reveals a direct association between the study discipline of knowledge criteria and Awareness response toward digital facilities in dental practices mentioned by the questioner for all participants concerning COVID-19, this association could be explained by the risk of confounding. However, it could be argued that this study was a descriptive study with no hypothesis testing. In this study, participants were recruited based on their willingness and ability to participate to show the signal of acceptability toward the digital era in dentistry a how can these facilities improve dental practices quality and reduce the risk value with patient safety especially in disaster or epidemic times such like COVID-19 breakdown. Therefore, the sample size used in this study was based on available resources. Also, the time of lockdown due to corona all facilities have done online with a short time and sample of the study.
Recommendations Dental students expressed their perspectives to work in dental healthcare with adequate COVID-19 infection control policies. So, The Governmental manpower of Health should ensure the strict interpretations of clear isolation procedures by the digital dental workflow in all healthcare facilities across the countries, including in dental clinics in all academic and clinical practice places during ready in all situations especially unexpected times like COVID-19 crisis.
Acknowledgments
I would like to thank Mrs. Baidaa Mohammed Merzah for her assistance to prepare questioner online form.
References
1. Gates B. Responding to Covid-19—A Once-in-a-Century Pandemic?. New England Journal of Medicine. 2020 Feb 28.
2. Dong N, Yang X, Ye L, Chen K, Chan EW-C, Yang M. et al. Genomic and protein structure modeling analysis depicts the origin and infectivity of. 2019 -nCoV, a new coronavirus which caused a pneumonia outbreak in Wuhan, China. 2020. DOI: https://doi.org/10.1101/2020.01.20.913368
3. Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet. 2020; 395:470-473.
4. Guidelines for Infection Control in Dental Health-Care Settings — 2003 www.cdc.gov/mmwr/PDF/rr/rr5217.pdf
5. Gamio, L. The Workers Who Face the Greatest Coronavirus Risk. Available online: https://www.nytimes.com/interactive/2020/03/15/business/economy/coronavirus-worker-risk. (accessed on 15 March 2020).))
6. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020; 6736:1-10.
7.Meng L, Hua F, Bian Z. Coronavirus Disease 2019 (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine. J. Dent. Res. 2020. [CrossRef]
8. Perspective Medscape Radiology Commentary Radiology Must Adapt to New Pandemic Saurabh Jha, MBBS, MRCS; Scott Simpson, DO DISCLOSURES )) March 20, 2020
9. Gallardo YR, Bohner L, et al. Patient outcomes and procedure working time for digital versus conventional impressions: A systematic review. The Journal of Prosthetic Dentistry. 2018;119(2):214–219.
10. Arora S, Mittal S, Dogra V. Eco-friendly dentistry: Need of future. An overview. Journal of Dental and Allied Sciences. 2017;6(1):22,
11. Rutalaand WA, Weber DJ. The Health care Infection Control Practices Advisory Committee (HICPAC).Guidelines for infection control in dental health-care settings 2003,” MMVR.2003;52:1-61. http://www.cdc.gov/mnwr/preview/mmwrhtlm/rr5217al.htm. [Accessed: Feb 15, 2019].
12. Park SW, Jang HW, Choe YH, et al. Avoiding student infection during a Middle East respiratory syndrome (MERS) outbreak: a single medical school experience. Korean J Med Educ. 2016;28(2):209–217.
13. Kharma MY, Alalwani MS, Amer MF, Tarakji B, Aws G. Assessment of the awareness level of dental students toward Middle East Respiratory Syndrome-coronavirus. Journal of International Society of Preventive & Community Dentistry. 2015 May;5(3):163.
14. Khan MU, Shah S, Ahmad A, Fatokun O. 2014 Knowledge and attitude of healthcare workers about Middle East respiratory syndrome in multispecialty hospitals of Qassim, Saudi Arabia. BMC Public Health .2014. 14:1281. https://doi.org/10.1186/1471-2458-14-1281
15. Baseer MA, Ansari SH, AlShamrani SS, et al. Awareness of droplet and airborne isolation precautions among dental health professionals during the outbreak of coronavirus infection in Riyadh city, Saudi Arabia. Journal of clinical and experimental dentistry. 2016 Oct;8(4):e379.
16. Hoda J. Identification of information types and sources by the public for promoting awareness of Middle East respiratory syndrome coronavirus in Saudi Arabia. Health Educ. 2016 Res 31:12–23. https://doi.org/10.1093/her/cyv061
17. Summary of Infection Prevention Practices in Dental Settings. USA: Centers for Disease Control and Prevention. 2016. http://www.cdc.gov/oralhealth/infectioncontrol/pdf/safe-care2.pdf. [Accessed: Feb 18, 2019].
18. -sixth-update-Outbreak-of-novel-coronavirus-disease-2019-COVID-19.pdf https://www.ecdc.europa.eu/sites/default/files/documents/RRA
19. https://www.facs.org/covid-19
20. Kanne JP, Little BP, Chung JH, Elicker BM, Ketai LH. Essentials for Radiologists on COVID-19: An Update-Radiology Scientific Expert Panel. Radiology. 2020:200527. DOI: http// doi.org./10.1148/radiol.2020200527. PubMed PMID: 32105562.
21. Mangano F, Shibli JA, Fortin T. Digital dentistry: new materials and techniques. International Journal of Dentistry, 2016, ArticleID5261247,2pages,2016. BioMed Research International13
22. Tordiglione L, De Franco M, Bosetti G. The Prosthetic Workflow in the Digital Era, International Journal of Dentistry, 2016;9823025,7.
23. Rakhshan V, Sforza C, Vucinic P, Vitalariu AM, and DeMenezes M. Advanced digital dentistry. International Journal of Dentistry. 2018:1-2.
24. Zitzmann N, Kovaltschuk I, Lenherr P, Dedem P, and Joda T. Dental Students’ Perceptions of Digital and Conventional Impression Techniques: A Randomized Controlled Trial. Journal of Dental Education. 2017;81(10):1227–1232.
Notas de autor
ammar_19_80@yahoo.com