
Esta obra está bajo una Licencia Creative Commons Atribución 4.0 Internacional.
Recepción: 14 Abril 2019
Aprobación: 28 Octubre 2019
DOI: https://doi.org/10.17058/.v1i1.13449
Abstract: Background and Objectives: The maintenance of regular development and maturation of the Central Neural System of the neonate in the first year, associated to the environmental conditions in which he is inserted, justify the scientific relevance of this research. Our objective was to describe the influence of stressful factors on hospitalized neonates in the Neonatal Intensive Care Unit of a teaching hospital. Methods: Cross-sectional study with convenience sampling. The participants were observed in moments that were identified as being of more and less exposition to stress factors, in which the sound pressure, illuminance, quantity of procedures, presence of pain, besides the indicators of vital signs expressed by the patient’s monitor were registered. Results: Thirteen neonates, predominantly moderate premature babies of low weight, of c-section birth, average age of 8.0 ± 5.9 days, mostly female and breathing room air were evaluated. We noted that stress factors produced significant increase of the heart rate (sound pressure: p=0.001, illuminance: p<0.001, procedures: p=0.022), occurring the same with the respiratory rate (sound pressure: p<0.001, illuminance: p=0.022, procedures: p<0.001) and score obtained in the Neonatal Pain Evaluation Scale (sound pressure: p=0.001, illuminance: p=0.016, procedures: p<0.003), besides the reduction of peripheral oxygen saturation (sound pressure: p=0.011, illuminance: p=0.024, procedures: p<0.016), when compared to the periods of higher and lower exposition. Conclusion: Our findings demonstrated the negative impact of the environmental factors and its influence on the vital signs of hospitalized neonates.
Keywords: Hospitalization, Neonatal Intensive Care Units, Physiological Stress, Neonate.
Resumo: Justificativa e Objetivos: A manutenção do desenvolvimento normal e a maturação do Sistema Nervoso Central do recém-nascido, no primeiro ano de vida, associado às condições ambientais nas quais está inserido, justificam a relevância científica desta pesquisa. Nosso objetivo foi descrever a influência de fatores estressores sobre os sinais vitais de recém-nascidos hospitalizados na Unidade de Tratamento Intensivo Neonatal de um hospital de ensino. Método:Estudo transversal com amostragem de conveniência. Os participantes foram observados nos momentos identificados como sendo de maior e de menor exposição a fatores estressores, sendo registrados níveis de pressão sonora, iluminância, quantidade de procedimentos, presença de dor, além dos indicadores de sinais vitais expressos pelo monitor do paciente. Resultados:Treze neonatos predominantemente prematuros moderados, de baixo peso, nascidos de parto cesárea, com média de idade de 8,0 ± 5,9 dias, preponderância feminina e respirando sob ar ambiente foram avaliados. Notou-se que ambos os fatores estressores provocaram aumento significativo da frequência cardíaca (pressão sonora: p=0,001, Iluminância: p<0,001, procedimentos: p=0,002), ocorrendo o mesmo com a frequência respiratória (pressão sonora: p<0,001, Iluminância: p=0,022, procedimentos: p<0,001) e escore obtido na Escala de Avaliação da Dor Neonatal (pressão sonora: p=0,001, Iluminância: p=0,016, procedimentos: p<0,003), além de redução da saturação periférica de oxigênio (pressão sonora: p=0,011, Iluminância: p=0,024, procedimentos: p<0,016), quando comparados os períodos de maior e de menor exposição. Conclusão: Nossos achados demonstraram o impacto negativo de fatores ambientais e sua influência sobre os sinais vitais de recém-nascidos hospitalizados.
Palavras-chave: Hospitalização, Unidades de Terapia Intensiva Neonatal, Estresse Fisiológico, Recém-nascido.
Resumen: Justificación y objetivos: El mantenimiento del desarrollo normal y la maduración del Sistema Nervioso Central del recién nacido, en el primer año de vida, asociado a las condiciones ambientales en las que está inserto, justifican la relevancia científica de esta investigación. Nuestro objetivo fue describir la influencia de factores estresores sobre los signos vitales de recién nacidos hospitalizados en la Unidad de Tratamiento Intensivo de un hospital de enseñanza. Métodos: Estudio transversal con muestreos de conveniencia. Los participantes fueron observados en los momentos identificados como de mayor y de menor exposición a los factores estresores, siendo registrados niveles de presión sonora, iluminancia, cantidad de procedimientos, presencia de dolor, además de los indicadores de los signos vitales expresados en el monitor del paciente. Resultad: Trece neonatos predominantemente prematuros moderados, de bajo peso, nacidos de cesárea con media de edad de 8,0 ± 5,9 días, preponderancia femenina y respirando en aire ambiente fueron evaluados. Se notó que ambos factores estresores provocaron aumento significativo de la frecuencia cardíaca (presión sonora: p=0,001, Iluminancia: p<0,001, procedimientos: p=0,002), ocurriendo lo mismo con la frecuencia respiratoria (presión sonora: p<0,001, Iluminancia: p=0,022, procedimientos: p<0,001) y puntación obtenida en la Escala de Evaluación de Dolor Neonatal (presión sonora: p=0,001, Iluminancia: p=0,016, procedimientos: p<0,003), además de reducción de la saturación periférica de oxigeno (presión sonora: p=0,011, Iluminancia: p=0,024, procedimientos: p<0,016), cuando comparados los periodos de mayor y de menor exposición. Conclusiones: Nuestros hallazgos demostraron el impacto negativo de factores ambientales y su influencia sobre los signos vitales del recién nacidos hospitalizados.
Palabras clave: Hospitalización, Unidades de Cuidado Intensivo Neonatal, Estrés Fisiológico, Recién nacido.
INTRODUCTION
The recent advances in Medicine associated to social indicators contributed to the reduction of child mortality in Brazil, especially in the neonatal period1. In this context, the Neonatal Intensive Care Unit (NICU) has significant importance in the mortality reduction of hospitalized neonates2.
Neonatal care demands a higher number of equipment and specialized therapeutic procedures to guarantee the survival of the hospitalized neonate3. However, the technological apparatus that guarantees the reduction of neonatal mortality can expose the neonate to an environment excessively stimulant, inherent to the intensive care, which can contribute to the emergence of stress4.
Stressful factors such as: elevated levels of sound pressure, illuminance, and procedures, individually or associated to pain sensation can cause the disorganization of different systems, contributing, therefore, to changes in the physiological and behavioral parameters that interfere in a negative way in the neurobehavioral development of hospitalized neonates.3,5-8
Neonates hospitalized in the NICU are constantly exposed to stress factors causing important reactions to their vital signs. While in a stress situation, the neonate is submitted to alterations in blood pressure, heart rate (HR), respiratory rate (RR) and oxygen peripheral saturation (SpO2)8. Besides, the liberation of hormones indicators of stress, such as cortisol, adrenaline and noradrenaline also take place9.
The maintenance of regular development and maturation of the Central Neural System of the neonate in the first year, associated to the environmental conditions in which he is inserted, justify the scientific relevance of this research3. Our objective was to describe the influence of stressful factors (high levels of sound pressure, illuminance, quantity of procedures and presence of pain over the vital signs) on hospitalized neonates in the NICU of a teaching hospital.
METHODS
Search
Cross-sectional study, in which each participant was its own control. Convenience sampling constituted by hospitalized neonates in NICU of a teaching hospital in a municipality of south Brazil, from August to December 2015.
The NICU in question has 8 beds and had an average of 8 hospitalizations per month during the research period, mostly consisting of premature newborns with complications related to delivery, metabolic disorders, in the immediate postoperative period or congenital pathology requiring hospitalization in the Unit.
The staff is composed of 1 doctor on duty every 24h shift, 1 nurse and 1 nursing technician for every two patients, distributed in 6h shift. In addition, speech therapists, physiotherapists, psychologists, nutritionists and social workers are responsible for the Unit's demand.
The NICU environment is of significant professional movement, especially during the morning shift, when routine procedures are performed and exams are scheduled by the attending physician; beyond the moments of shift change. As a result, newborns undergo manipulations of varying lengths to receive: hygiene care, diaper and dressing changes, tube feeding every 2 or 3 hours, decubitus changes, pulmonary and cardiac auscultation, intravenous medication application, maintenance of orogastric tube and venous puncture, among other procedures.
The protocol followed the conditions established in Resolution 466/12 of Health National Council without offering any risks to the participants and was approved by the Committee of Ethics in Research of the University of Santa Cruz do Sul, under number 1.172.112.10 All legal representatives of the participants signed the Informed Consent Form (ICF) authorizing the participation in the study.
Participants
The criteria for inclusion in the sample were: neonates of both genders, independent of ethnicity, type of birth, gestational age, weight, height, hospitalization period, need of ventilation support or place of birth. Patients with the following clinical diagnosis were excluded: congenital malformation, neurological pathology, glycemic disturb, negative cochlear response and red reflex in neonatal examination, hemodynamically instable, in use of analgesic or sedatives during the last 12 hours, in phototherapy, using ocular or hearing protection, in immediate post operative care of abdominal surgery or in which the legal representative did not authorize the participation in the study.
Among a total of 33 admitted patients in the NICU, during the period of the research, 26 were eligible to the study, according to the established criteria. In 5 neonates, the data collection was not possible due to their discharge of the NICU before performing and in 8 of them because of the unfavorable climate conditions due to several days of cloudiness, remaining 13 patients to the analysis of the study.
Procedures
The research was made in two steps, demanding several days of monitoring to rigorously collect data, in a confidential way in all its execution with the objective of preserving the NICU routine, being informed to the professionals and legal representatives of the participants that the procedures were to investigate radiation levels inside the incubator. Besides, in order to avoid study bias, the data collection were automatically interrupted and the values were not considered during the occurrence of adverse events that could bias the obtained results, such as, for example, a cardiopulmonary arrest.
Collect one. The first stage to data collection was developed through a pilot study, in order to explore the target environment and to identify the period of higher and lower exposition to the stress factors characterized in this study. In order to do that, the higher and lower peaks of sound pressure were measured, during a period of 24 hours, through the use of a digital Dosimeter (Instruterm, model DOS500, Brazil), with capacity to store register data of sound pressure in decibels (dBA). The higher and lower peaks of illuminance were measured through the use of a digital Luxmeter (Lightmeter, model Center337, Taiwan), and the values were registered in lux (lx) in three moments, in intervals of 1 hour and 30 minutes in each shift, in a sunny day, in order to obtain the maximum fidelity as to the influence of natural light associated to artificial light over the inside environment of the NICU.
The peaks of higher and lower manipulation of patients were determined through the use a specific checklist structured by the researcher, in which the professionals involved in the direct care of the patient received the proper orientation in order to correctly fill it, being stimulated to signal the corresponding procedure, the quantity and the time interval in which it was done.
Collect two. After the collection of the results obtained through the pilot study, the second stage to data collection of the research was executed, in which patients were selected according to the criteria previously described and, based on these criteria, observed in the appointed moments of higher and lower exposition to stress factors. In each distinct moment the patient was analyzed for 10 (ten) minutes. During this period, the corresponding maximum values were registered, such as sound pressure, through the use of a digital Decibelmeter (Minipa, model MSL-1325, Brazil), illuminance, measured inside the incubator, the quantity of procedures that were realized, considering the 60 minutes before the evaluation, the presence of pain, as well as the vital signs shown in the patient’s monitor.
Measures
The excess of sound pressure was considered in any level superior to 45 dBA and the excess of illuminance in any value above 600 lx, its cumulative effect was not analyzed.11,12 To the evaluation of the presence of pain, the Neonatal Infant Pain Scale (NIPS) was used, composed of six parameters, among which five are behavioral (facial expression, cry, arm and leg position and consciousness state) and one is physiological (respiratory pattern). In each parameter there are two items that have to be scaled in 0 or 1, except the item cry, which has scales from 0 to 2. The total score of the scale can vary from 0 to 7 points. Pain is present when the score is superior to 3.13
As to the vital signs, expressed in the patient’s monitor, these were the parameters of normality considered: HR of 120-160 beats per minute, RR of 30-60 breaths per minute and SpO. equal or superior to 91%.12,14
Data Analysis
The collected data were analyzed using the Statistical Package for the Social Sciences (SPSS) program, version 20.15 The results were presented in a descriptive manner, expressed in averages, standard deviation and distribution of frequencies, being initially analyzed as to the normal distribution through the Shapiro-Wilk test. In order to correlate the obtained results during the moment of higher and lower exposition to stress factors, the paired t-Student and Kruskal-Wallis tests were used. To the effect of statistical significance, a p<0.05 was used.
RESULTS
The sample was constituted predominantly by female neonates, average of 8.0 ± 5.9 days, moderately premature, of low weight, born of c-section, and who were in room air in the evaluation moment (TABLE 1).
Description of the studied sample according to the clinical characteristics of participants.
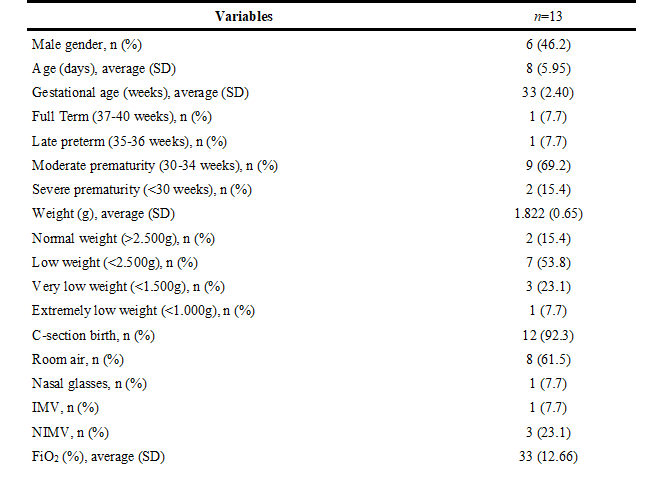
n: Absolute frequency; %: Relative frequency; SD: Standard Deviation; IMV: Invasive Mechanical Ventilation; NIMV: Non-Invasive Mechanical Ventilation; FiO2: Inspired Oxygen Fraction.
The periods of higher and lower exposition to stress factors, monitored through the pilot study, are expressed in Figure 1. We observe that the period of higher exposition of elevated sound pressure levels and the realization of procedures occurred right after the shift of personnel, in the morning (07:30 a.m. – 09:00 a.m.) and the lower exposition was in the night shift (10:00 p.m. – 11:00 p.m.). The maximum peak of illuminance occurred during the day (11:30 a.m.) and the lower was in the night shift (after 7:30 p.m.).
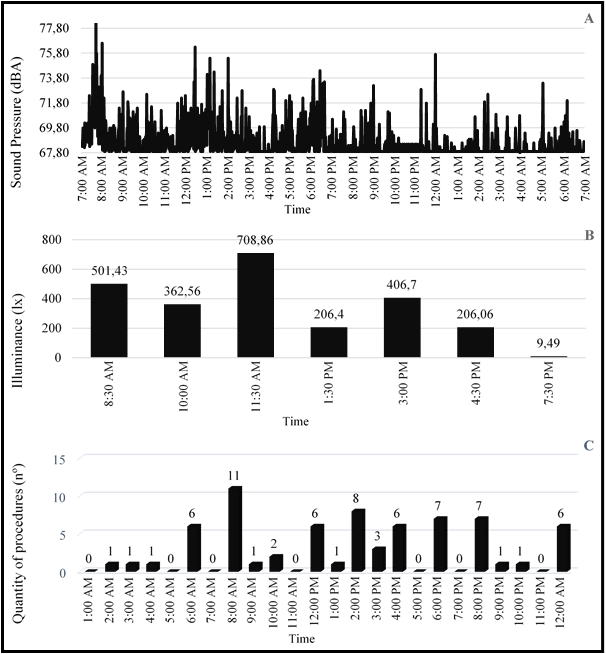
Figure 1.
Results that correspond to the higher and lower exposition to stress factors during the evaluation period. A: Levels of sound pressure expressed in decibels (dBA). B: Levels of natural illuminance associated to artificial illuminance expressed in lux (lx). C: Quantity of realized procedures expressed in numbers (nº).
The average values registered between the stress factors, during the periods identified as being of higher and lower exposition, are presented in Figure 2. We observed a reduction of the sound pressure levels (63.0±6.8 dBA versus 55.1±3.1 dBA), illuminance (150.5±63.9 lx versus 6.5±3.4 lx) and the quantity of realized procedures (3.2±1.8 versus 0.0±0.0), which all reached the levels of significance stipulated in the study (p<0.05).
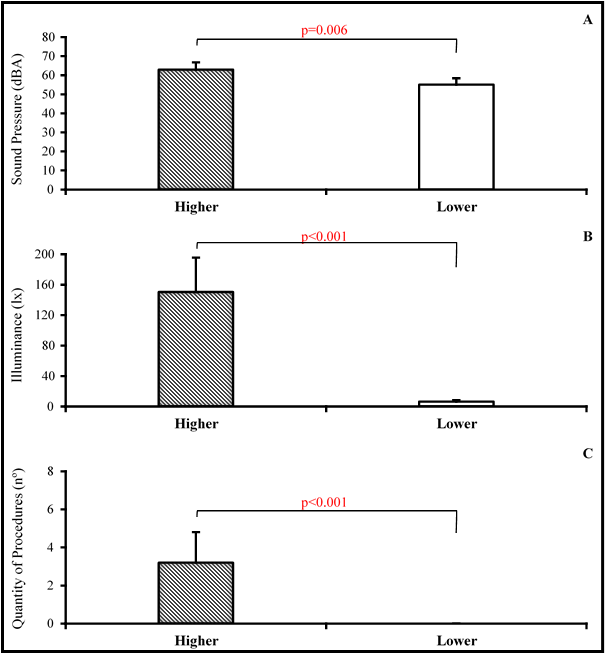
Figure 2
Results that correspond to the average levels between stress factors during the periods of higher and lower exposition. A: Levels of sound pressure (63.0±6.8 dBA vs. 55.1±3.1 dBA). B: Levels of natural illuminance associated to artificial illuminance (150.5±63.9 lx vs. 6.5±3.4 lx). C: Quantity of realized procedures (3.2±1.8 vs. 0.0±0.0). Values expressed in average and standard deviation (p<0.05).
Respective to the influence of stress factors over the vital signs of the participants, when compared to the higher and lower exposition, we noted a significant statistical increase in the levels of HR (sound pressure: p=0.001, illuminance: p<0.001, procedures: p=0.002), RR (sound pressure: p<0.001, illuminance: p=0.022, procedures: p<0.001), and NIPS score (sound pressure: p=0.001, illuminance: p=0.016, procedures: p<0.003), besides the reduction of SpO. (sound pressure: p=0.011, illuminance: p=0.024, procedures: p<0.016) (TABLE 2).
Influence of elevated levels of sound pressure, illuminance and quantity of procedures on the vital signs of neonates, during the period of higher and lower exposition.

HR: Heart Rate; RR: Respiratory Rate; SpO2: Peripheral oxygen saturation; NIPS: Neonatal Infant Pain Scale; M: Average; SD: Standard Deviation; Diff.: Difference between the period of higher and lower exposition. * Estimated value of p during the paired t-Student Test to the comparison of the difference between the period of higher and lower exposition. ** Estimated value of p through the Kruskal-Wallis Test to the comparison of the difference between stress factors. β Difference between Illuminance vs. Procedures (p=0.001) and Illuminance vs. Sound Pressure (p<0.001). Values expressed in average and standard deviation (p<0.05).
DISCUSSION
The objective of the study in question was to describe the influence of stress factors, such as: high levels of sound pressure, illuminance, quantity of procedures and presence of pain on the vital signs of hospitalized neonates. Our results showed that, during the periods of higher exposition, the stress factors caused significant alteration in the vital signs and in NIPS score, when compared to the moments of lower exposition.
Recent studies, with the objective to determine the epidemiologic profile of child mortality in the neonatal period, showed prematurity and low weight at birth as the most important factors related to death in hospitalized neonates.16-18 Besides, the lower the gestational age and the weight at birth, the higher are the risks of these neonates to show problems in their neurobehavioral development.19These risks are consistent not only because they are prone to malformation and congenital neuropathies, but also because they are exposed for a longer period to iatrogenic factors, such as: isolation from his/her mother, longer period in incubator, effect of medication, mechanical ventilation and stress due to an extremely stimulant environment.20
Although the causes associated with weight loss in the neonatal period are multiple, the stressors evidenced in this study may cause increased caloric demand and excessive weight loss4. This exposure is of great concern, considering that the sample consisted predominantly of moderate and low birth weight premature infants, which may contribute to a worse prognosis, increased morbidity and mortality.20
The multi-professional team involved in direct care of the neonate can be an important source of stress in the NICU, increasing substantially the exposition of neonates to elevated sound pressure and excessive manipulation5. The fact that the higher quantity of procedures and elevated levels of sound pressure were identified in the morning shift in our study, right after the change of personnel, can be justified by the fact that the day shifts have higher number of professionals, clinical evaluations and collection of de exams, besides the fact that the team changes are destined to information exchange about patients among teams, and this is in accordance with the literature7.
In this study, the most frequently performed procedures observed at the time of the evaluation were: capillary glycemia, diaper changes and dressing, decubitus change, pulmonary and cardiac auscultation, intravenous medication application, orogastric tube maintenance and venous puncture. Therefore venous puncture is possibly the procedure that caused the most stress in the studied neonates.21,22
Inadequate illuminance conditions are considered one of the environmental factors that generate stress in the NICU, predisposing the neonates to retinopathy, physiological instability and long term neurobehavioral prejudice6. The addition of natural light to artificial light explain the higher levels of illuminance identified in our study in the day shifts, specially at 11:30a.m.
The significant difference evidenced in all vital signs and NIPS score, when compared the higher and lower exposition to the studied stress factors, are in accordance with the literature that confirms the deleterious effects of high levels of sound pressure, illuminance, procedures, isolated or associated to pain sensation, over the physiological stability, of hospitalized neonates.5-8,13
The immediate physiological effects of elevated sound pressure on neonates include: increase of HR and RR, diminution of SpO., increase of blood pressure, apnea and alterations in the sleep-vigil state.23 Although the elevated levels of sound pressure in the NICU can be generated by the noise produced by the use of innumerous life support equipment, we believe that, in this study, the main source was the conversation between professionals and activities realized by the health team in the assistance of neonates. We may highlight that in both identified periods of higher and lower exposition, the average levels of sound pressure that were registered remained above the recommended.11 These results are concerning, once the measurement occurred inside the incubator.
In relation to illuminance, the levels that are tolerated at the NICU may vary between 10-600lx.12 This factor itself demonstrates the innovative character of this study, considering that, even when exposed to lower levels than those recommended, it was possible to observe the significant effects of the excess of illuminance on the vital signs and NIPS score. Besides, denotes the inefficiency of the adopted measures to cover the incubators in order to avoid excessive visual stimulation, considering that the illuminance measurements occurred inside the compartment.
The exposition of neonates to excessive or disorganized manipulations can be a source of stress and cause alterations in blood pressure, heart rate, respiratory rate and peripheral oxygen saturation, as evidenced in this study4. However, the tactile and kinesthetic stimulation, techniques that are admittedly used by physiotherapists in the NICU, have relevant contribution to the immunological system, weight gain, calorie burn, hospitalization period, bone formation and mineralization, sleep-vigil state, body temperature, brain maturation speed and gastric mobility, demonstrating the importance of the action of this professional in the behavioral and physiological stress responses of hospitalized neonates.24,25
Although this study did not evidence the presence of pain associated to the other stress factors, we noticed a significant difference in the NIPS score when the periods of higher and lower exposition were individually compared and between illuminance versus procedures and illuminance versus sound pressure.
In spite of the significant results, some limitations deserve proper attention, such as the methodological design, which did not permit more interference in the results. Another important limitation that contributed to the difficulty in data collection was the unfavorable regional climate conditions, which sometimes impeded the adequate illuminance incidence and, therefore, the collection sometimes had to be interrupted.
Our findings demonstrated the negative impact of environmental factors and their influence on the vital signs of hospitalized neonates. The methodology that was employed enabled the analysis of their immediate effects, not considering the time of exposition or their long term consequences, which recommend the realization of new studies that allow identify the observed changes due to the exposition of stress factors after hospital discharge.
REFERENCES
1. Rasella D, Aquino R, Santos CAT, et al. Effect of a conditional cash transfer programme on childhood mortality: a nationwide analysis of Brazilian municipalities. The Lancet. 2013; 382 (9886): 57-64. http://dx.doi.org/10.1016/S0140-6736(13)60715-1
2. Shahheidari M, Homer C. Impact of the design of neonatal intensive care units on neonates, staff, and families: a systematic literature review. J Perinat Neonatal Nurs. 2012; 26 (3): 260-266. http://dx.doi.org/10.1097/JPN.0b013e318261ca1d
3. Orsi KCSC, Llaguno NS, Avelar AFM, et al. Effect of reducing sensory and environmental stimuli during hospitalized premature infant sleep. J Sch Nurs - University of São Paulo. 2015; 49(4):550-555. http://dx.doi.org/10.1590/S0080-623420150000400003
4. Moore TA, Berger AM, Wilson ME. A new way of thinking about complications of prematurity. Biol Res Nurs. 2014; 16(1):72-82.
5. Correia CQOS, Mendonça AEO, Souza NL. Scientific production on noise in the neonatal intensive care unit: integrative review. J Nurs - University of Pernambuco. 2014; 8 (Supplement 1):2406-2412.
6. Aita M, Johnston C, Goulet C, et al. Intervention Minimizing Preterm Infants’ Exposure to NICU Light and Noise. Clin Nurs Res. 2012; 22(3):337-358. http://dx.doi.org/10.1177/1054773812469223
7. Pereira FL, Góes FSN, Fonseca LMM, et al. Handling of preterm infants in a Neonatal Intensive Care Unit. J Sch Nurs - University of São Paulo. 2013; 47(6):1272-1278. http://dx.doi.org/10.1590/S0080-623420130000600003
8. Cordeiro RA, Costa R. Non-pharmacological methods for relief of discomfort and pain in newborns: a collective nursing construction. Text Context Nurs. 2014; 23(1):185-92. http://dx.doi.org/10.1590/S0104-07072014000100022
9. Dias FSB, Marba STM. The evaluation of prolonged pain in the newborn: adaptation of the EDIN scale for the Brazilian culture. Text Context Nurs. 2014; 23(4):964-970. http://dx.doi.org/10.1590/0104-07072014002100013
10. Brazil, Health Ministry, Health National Council, National Committee on Ethics in Research. Resolution 466/2012: Guidelines and regulatory standards of researches involving humans. Brasília, DF: Health National Council; 2012.
11. White RD, Smith JA, Shepley MM. Recommended standards for newborn ICU design, eighth edition. J Perinatol. 2013; 33 (Supplement 1):S2–S16. http://dx.doi.org/10.1038/jp.2013.10
12. American Academy of Pediatrics, American College of Obstetricians and Gynecologists. Guidelines for Perinatal Care. 7th ed. Elk Grove Village, IL/Washington, DC; 2012.
13. Schardosim J, Motta G, Cunha M. Neonatal Infant Pain Scale: Cross-Cultural Adaptation and Validation in Brazil. J Pain Symptom Manage. 2015; 50(3):394-401. http://dx.doi.org/10.1016/j.jpainsymman.2015.03.019
14. McKinney ES, James SR, Murray SS, et al. Maternal-Child Nursing. 4th ed. St Louis, MO: Saunders Elsevier; 2013: 484-808.
15. IBM SPSS [Software]. Version 20. Armonk, NY: IBM Corporation; 2012.
16. Atkinson AL, Santolaya-Forgas J, Blitzer DN, et al. Risk factors for perinatal mortality in patients admitted to the hospital with the diagnosis of placental abruption. J Matern Fetal Neonatal Med. 2015; 28 (5):594-597. http://dx.doi.org/10.3109/14767058.2014.927427
17. Katz J, Lee AC, Kozuki N, et al. Mortality risk among term and preterm small for gestational age infants. In Low-Birthweight Baby: Born Too Soon or Too Small. Vol 81. Karger Publishers; 2015: 29-35.
18. Rakhsha M, Pourali L, Ayati S, et al. Effective maternal and neonatal factors associated with the prognosis of preterm infants. Patient Saf Qual Improv J. 2016; 4(1):327-333. http://dx.doi.org/10.22038/PSJ.2016.6304
19. Brocchi BS, Leme MIS. Relation between mother-child interaction upon the development of oral language of the preterm newborn. Audiol Commun Res. 2013; 18(4):321-331. http://dx.doi.org/10.1590/S2317-64312013000400014
20. Grunau RE. Neonatal pain in very preterm infants: long-term effects on brain, neurodevelopment and pain reactivity. Rambam Maimonides Med J. 2013; 4(4):e0025. http://dx.doi.org/10.5041/RMMJ.10132
21. Barros MMA, Luiz BVS, Mathias CV. A dor como quinto sinal vital: práticas e desafios do enfermeiro em uma unidade de terapia intensiva neonatal. BrJP. 2019; 2(3):232-6. http://dx.doi.org/10.5935/2595-0118.20190041
22. Rebelato CTC, Stumm EMF. Análise da dor e do cortisol livre em recém-nascidos em terapia intensiva com procedimentos terapêuticos. BrJP. 2019; 2(2):159-65. http://dx.doi.org/10.5935/2595-0118.20190029
23. Santos J, Pearce SE, Stroustrup A. Impact of hospital-based environmental exposures on neurodevelopmental outcomes of preterm infants. Curr Opin Pediatr. 2015; 27(2):254-260. http://dx.doi.org/10.1097/MOP.0000000000000190
24. Metgud D, Honap R. Comparison of kangaroo mother care and tactile kinesthetic stimulation in low birth weight babies – an experimental study. Int J Disabil Hum Dev. 2015; 14(2):147-150. http://dx.doi.org/10.1515/ijdhd-2014-0011
25. Aliabadi, F, Askary RK. Effects of Tactile–Kinesthetic Stimulation on Low Birth Weight Neonates. Iran J Pediatr. 2013; 23(3):289–29.
