
Esta obra está bajo una Licencia Creative Commons Atribución 4.0 Internacional.
Recepción: 07 Enero 2020
Aprobación: 15 Julio 2020
DOI: https://doi.org/10.17058/jeic.v10i3.14674
Abstract: Background and Objectives: To analyze the golden time developed by the Mobile Emergency Care Service (Samu) in Floriano, Piauí, Brazil. There are few productions that primarily emphasize the service’s response time (golden hour), crucial for students and professionals in the field, whose knowledge on the issue can lead to saving lives. Methods: This is a descriptive, documentary, and quantitative study that analyzed emergency care records for the year 2018. It is based on the survey of the variables of the golden time stages, their nature, and the duration of events, analyzed by descriptive and inferential statistics. This study met all ethical principles based on the approval opinion of the ethics committee (No. 96443518.4.0000.5660). Results: The most frequent golden time performed by Samu was 15 to 30 minutes, in 58.5% of the cases. Adult clinical urgencies and emergencies were the most common types of events (35.50%). Conclusion: The most frequent service provided by Floriano’s Samu was clinical urgencies and emergencies in adults, with a response time of 15 to 30 minutes.
Keywords: Emergencies, Reaction time, Health, Emergency medical services.
Resumo: Justificativa e Objetivos: Analisar o golden time desenvolvido pelo Serviço de Atendimento Móvel de Urgência (Samu) da cidade de Floriano, Piauí, Brasil. Justifica-se por haver poucas produções que enfatizam primordialmente o tempo (goldenhour), imprescindível aos estudantes e profissionais da área médica, do qual o domínio e o conhecimento, podem salvar vidas. Métodos: Trata-se de estudo descritivo, documental e de abordagem quantitativa realizado a partir de registros em fichas de atendimento referentes ao ano de 2018, com base no levantamento das variáveis das etapas do golden time, da natureza e do tempo do evento, analisados por meio de estatística descritiva e inferencial. Resultados: O golden time mais frequentemente desenvolvido pelo Samu, em 58,5% dos casos, foi de 15 a 30 minutos. As urgências e emergências clínicas em adultos foram os tipos de evento mais comumente atendidos (35,50%). Conclusão: Os atendimentos de maior frequência do Samu de Floriano foram de casos de urgências e emergências clínicas em adultos, com tempo de resposta de 15 a 30 minutos.
Palavras-chave: Emergências, Tempo de reação, Saúde, Serviços médicos de emergência.
Resumen: Justificación y Objetivos: Analizar el tiempo de oro desarrollado por el Servicio de Emergencia Móvil (Samu) en la ciudad de Floriano, Piauí, Brasil. Son pocas las producciones que enfatizan primordialmente el tiempo (hora dorada), esencial a los estudiantes y profesionales del campo médico, del cual tener dominio y conocimiento pueden salvar vidas. Métodos: Se trata de un estudio descriptivo, documental y de abordaje cuantitativo, realizado desde los registros en las fichas de atención del año 2018, con base en la búsqueda de las variables de las etapas del tiempo de oro, naturaleza y tiempo del evento, analizados mediante la estadística descriptiva e inferencial. Resultados: El tiempo de oro con mayor frecuencia, en el 58,5% de los casos, desarrollado por Samu fue de 15 a 30 minutos. Las urgencias y emergencias clínicas de adultos fueron los tipos de eventos más frecuentes (35,50%). Conclusión: La atención más frecuente en Samu de Floriano fueron los casos urgentes y de emergencias clínicas en adultos, con el tiempo de respuesta de 15 a 30 minutos
Palabras clave: Urgencias Médicas, Tiempo de reacción, Servicios médicos de urgencia.
INTRODUCTION
“Golden hour” is a theory from the late 1960s whose purpose is to offer trauma victims the best possible emergency care in the shortest time between the event and the action of the rescuers, which is a crucial period for rescue of the victim1. Currently, it is recommended to use the term “golden time” instead of “golden hour”, as it is not possible to set an exact time for the victim care in different situations. Thus, the term "golden time" is ideal because the rescue may take more than one hour to arrive.
According to the Ministry of Health, pre-hospital care (PHC) is defined as the assistance provided in a first level of care to patients with acute conditions, whether they are of a clinical, traumatic or psychiatric nature, whose purpose is to provide early assistance to victims of health problems of different natures at the place of their occurrence2.
In Brazil, the PHC system is divided into mobile and fixed services, so that mobile care has the mission of providing immediate assistance to victims who are referred to the fixed PHC or to hospital care. This work can be performed by professionals whose specific training for the rescuer activity is a criterion used to enable them to work in pre-hospital services. This occurs in many countries like the United Kingdom, the USA, and France, but not in Brazil3.
No occurrence, scene, or patient is the same, requiring the team to have the flexibility to act according to each situation. The objective of pre-hospital emergency care is always the same: (1) reach the victim; (2) identify and treat injuries as early as possible; and (3) immobilize it and transport it to the reference institution4.
The PHC has predefined time intervals in order to provide greater agility in the passage between the trauma site and the hospital, including: the travel time from the base to the scene (activation of the service and arrival at the site); the on-scene interval (arrival at the site and on-site care); the travel time from the scene to the reference service (departure from the scene); and the golden time (activation of the service and arrival at the hospital).
This process provides for emergency care within realistic timescales to achieve positive results in saving lives. The concept assumes that, in the first hour of effective care, the person who suffered trauma is more likely to survive than after this period5,6.
Considering all the obstacles in this process, we raise the following question: is the response time of the Mobile Emergency Care Service (Samu) in the city of Floriano (Piauí, Brazil) adequate? To answer it, we analyzed the golden time of Samu in this municipality.
METHODS
This is a descriptive, documentary study with a quantitative approach carried out in the city of Floriano, in the period between February and March 2019 on the decentralized basis of Samu.
The municipality of Floriano is located in a reference point, right at the entrance to the south and southeast of Piauí. According to data from the Brazilian Institute of Geography and Statistics (IBGE), for the year 2020 it is estimated that its population is 60,025 people. It is the fifth richest city in the state, with a gross domestic product per capita of R$ 17,285.077, with the service sector being the most important for the municipality’s economy. During the morning, its shopping malls serves a large number of people from various cities in southern Piauí and Maranhão, causing traffic-related disorders in that location. Floriano also stands out as an educational pole, as it has a vast education network, especially at higher and technical levels. In terms of health services, the municipality offers extensive care in both the public and private sectors. It has a medium-sized regional hospital and basic health units throughout the territory, and it is a reference in neurosurgery assistance, with emergency care, outpatient emergency, and surgical procedures. The city also has a network of private clinics with a small private hospital. These services meet the demand of the macro-region in several specialties. Samu, implemented in 2006, works in support, hospital transport, clinical cases, and trauma in the region.
We used the records of emergency care carried out in 2018 by nursing students to constitute the study population. Then, we collect the variables related to the stages of the golden time, the nature of the emergency care, and the time of the event. Thus, of the 4,038 complications due to external and clinical causes, we established the weighted average of monthly occurrences (336.5) for verification.
We included services classified as cases of urgency or emergency that occurred on urban public roads in the municipality, regardless of sex and age, as well as those that required displacement from the Advanced Support Unit, Basic Support Unit or other. Calls for clinical, obstetric, traumatic. or psychiatric health care were also included. Cases of predominance in rural areas, such as snakebites, were excluded.
Data analysis was carried out using descriptive and inferential statistics, in which categorical variables are presented using distributions of absolute and relative frequencies. For quantitative variables, measures of centrality (mean) and variability (standard deviation) were used. The Student t test was used to compare the golden time measured with the standard recommendation found in the international literature, using the significance level p> 0.05 in the Statistical Package for the Social Sciences (SPSS, version 22) software. For the description and analysis of Samu’s response times, the 95% confidence interval (CI) was used, with an error of 5% and a significance level of 5%.
The project of this study was submitted to and approved by the Research Ethics Committee of the Federal University of Piauí, according to opinion No. 96443518.4.0000.5660 and CAAE 96443518.4.0000.5660, respecting Resolution No. 466/2012 of the National Health Council.
RESULTS
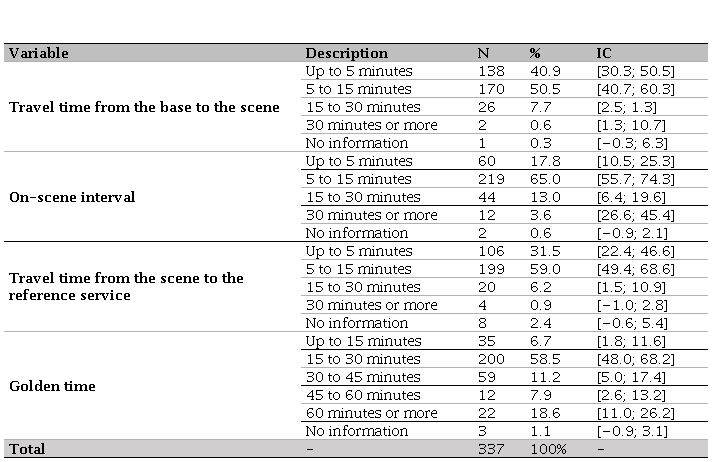
The average time spent by Samu in each stage was 5 to 15 minutes – occurring in 50.5% of the trips from the base to the scene, in 65% of the services on site and in 59% of the trips from the scene to the reference service –, with the exception of golden time, which ranged from 15 to 30 minutes in most cases (58.5%) (Table 1).
Description of the time spent according to the steps of the golden time in the emergency cares made in Floriano Piauí in 2018
Most class were for or adult clinical urgencies or emergencies (35.5%), followed by traffic accidents (28.8%) and falls (6.8%). The least frequent cases (0.3%) were sudden illness, stab wounds, thermal shock, situations in which the victim had already been removed when the service arrived at the scene, and those in which the victim died before help arrived (Figure 1).
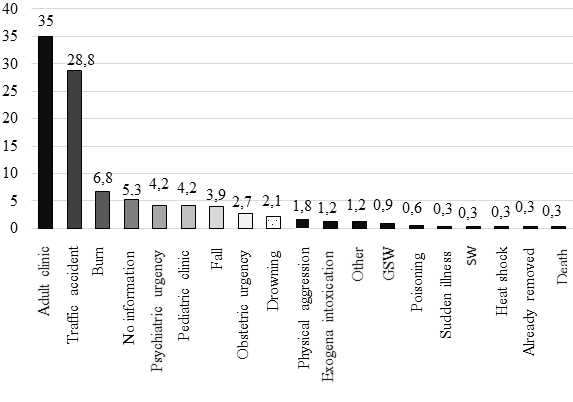
Figure 1
Distribution of care services provided by Samu, according to the nature of the event, in Floriano, Piauí, in 2018.
GSW: gunshot wounds; SW: stab wounds.
In the trauma-orthopedic emergency group, the most frequent cases were traffic accidents (28.8%), for which the minimum service time was 8 minutes, and the maximum was 1,014, with an average of 38 and a mode of 22 minutes. In other words, despite the average time taken to deal with traffic accidents is 38 minutes, the most frequent golden time was 22 minutes. Falls were the least frequent event, with 13 occurrences. In this case, the minimum service time was 15 minutes, and the maximum 43, with a mean and mode of 22 minutes, the latter being the time that was most frequent in the emergency care (Table 2).
Classification of services according to their nature and time golden time held in Floriano Piauí in 2018
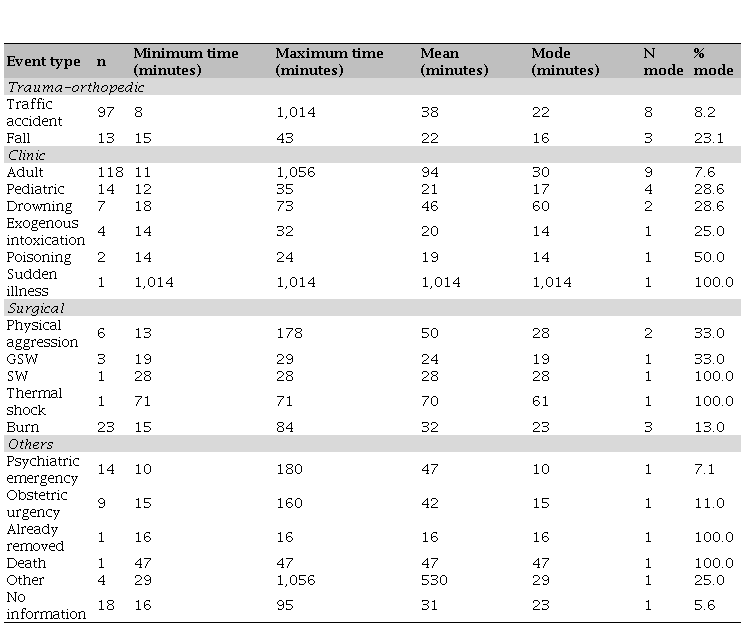
GSW: gunshot wounds; SW: stab wounds.
DISCUSSION
The transportation time to the specialized health service is an essential factor to be considered in the prognosis of the traumatized person, as it is extremely important that the PHC systems are strengthened and organized8.
In a highly urbanized area, where traffic conditions fluctuate constantly, transport infrastructure is a major contributor to ease of maintenance and reliable vehicle circulation. Thus, the stage of travel time from the base of Samu to the scene of the occurrence is the most affected by interference from external actions9.
The average time required to provide an ideal care to the victim is around 30 and 40 minutes. Thus, it can be said that the time used by Floriano’s service fits the recommendations, since about 80% of the emergency cares were performed within 30 minutes, making patients more likely to have a positive prognosis1.
One of the premises of the PHC is to arrive at the scene of the injury early, to intervene in the shortest possible time, reducing sequelae or deaths, and to improve the survival conditions of the victims, ensuring proper care and transportation. These premises have a strong impact on health problems in which time is a determining factor for the outcome of care10.
These scenarios, in turn, lead to an important issue in this analysis: the concept of potentially preventable death, that is, one that could be prevented if the right treatment was administered, at the ideal time11.
In this sense, the present study shows a transition from the most frequent cases answered by Samu, since clinical care for adults is the most requested service, countering the idea that traffic accidents are the major cause of traumatic conditions, as found for the country and states12.
Traffic accidents are among the main causes of mortality worldwide, especially in developing countries, such as Brazil. In addition, they are responsible for the main cause of disease burden in developed countries, in which an individual dies in traffic accidents every 20 minutes. This occurs due to the carelessness of citizens, who abuse speed limits, neglect safety measures, and constantly abuse alcohol intake13. The United Nations has recognized urban traffic accidents for several years as a serious public health problem worldwide, as they are accompanied by a high rate of morbidity and mortality14.
The cases of sudden illness appear as one of the less frequent. Its cause may be linked not only to loss of consciousness, but also to a range of situations and problems, such as heart attack, stroke, among others, as indicated by the current guidelines of the American Heart Association, focused mainly on the prevention of sudden illness15 . It is also worth mentioning the “XABCDE” approaches to assisting multiple trauma patients, which allow a preliminary assessment in order to avoid aggravating the victim’s condition or even a sudden illness15.
In turn, trauma has occupied a prominent place in the statistics of diagnoses and hospital admissions. Therefore, it is characterized as a pandemic of modern life and a serious public health problem, since it reached the first place as the etiology of morbidity and mortality of the general population11.
The less frequent cases in the group of trauma-orthopedic events are falls, with an average time of 22 minutes, in accordance with the predicted. Thus, all times observed in this group are within the parameters recommended by the golden time metric.
Among clinical events, cases of emergency medical care in adults predominated. In these events, especially those that require specialized referral services or even vacancies in the intensive care unit, there is a tendency to occur a significant increase in the time spent by Samu in the rescue, which can be explained by common situations in Brazilian health services, such as overcrowding, excess demands and lack of a specific unit to receive the case.
We note that cases of snakebites did not count in the occurrence count. This can be justified by the fact that the sample is exclusively urban and by the sample fluctuations, although Samu serves the urban and rural areas.
The maximum time observed was different from what is expected, being inconsistent with reality. This can be attributed to transfers made to other hospitals – in this case, to the capital Teresina –, or even to a mistake in the annotation. This may imply a misinterpretation of the data, leading the reader to imagine that the service needs a much longer time than recommended for its performance, when, in fact, what happened was an incorrect record.
At this point, users affected by clinical conditions in situations that destabilize their vital condition require early and qualified intervention. These are one of the reasons for seeking health services, which include mobile care 16.
Still in the category of clinical cases, those of drowning are noteworthy, and it can be inferred that they have demanded greater dedication from rescuers because they are slightly more complex events. Burns, on the other hand, differ from what is expected in their maximum emergency care time, despite their minimum time following the parameters recommended by the golden time – which is necessary, since it is a traumatic event.
As for events of a surgical nature, aggressions also reach a high average time, although the minimum is within the recommended time. In these situations, the provision of assistance presents complicating factors, such as popular crowding, making it difficult for professionals to withdraw the victim.
CONCLUSION
In this study of the PHCs of Samu de Floriano (Piauí, Brazil), we found that the most frequent cases were adult clinical urgencies or emergencies, usually taking 15 to 30 minutes to provide assistance. It is worth mentioning some limitations of the study, such as the lack of a reference that explains the topic addressed, in addition to the specific difficulties that may occur in the service. Therefore, this study should not be exhausted by the results presented, but new perspectives must be stimulated and implemented with the aim of improving the PHC service.
Acknowledgments
We are grateful for the contribution of those who participated in the study, as well as those who indirectly assisted in its construction.
REFERENCES
1. Ministério da Saúde. Secretaria de Atenção à Saúde. Protocolos de Intervenção para o SAMU 192 – Serviço de Atendimento Móvel de Urgência. Brasília: Ministério da Saúde, 2016.
2. Ministério da Saúde. Secretaria de Estado da Saúde. Governo do Estado de Alagoas.
3. Crespilho DF, et al. Segurança Do Paciente Na Assistência Pré-Hospitalar de Emergência: Uma Revisão Integrativa. Revista Uningá Review, 2015; 24 (1), p. 45-49.
4. Garçon TL, Pupulim JSL. Qualidade do atendimento pré-hospitalar móvel de urgência na perspectiva dos profissionais/ Quality of emergency in mobile prehospital care in the perspective of professionals. Cienc. Cuid. Saúde [Internet]. 19º de dezembro de 2017 [citado 23º de fevereiro de 2021];16(4). Disponível em: http://periodicos.uem.br/ojs/index.php/CiencCuidSaude/article/view/37306
5. Mock CN, Jurkovich GJ, Nii-Amon-Kotei D, Arreola-Risa C, Maier RV. Trauma mortality patterns in three nations at different economic levels: implications for global trauma system development. J Trauma. 1998 May;44(5):804-12; discussion 812-4. http://dx.doi.org/10.1097/00005373199805000-0001
6. Fukushima AR, Corrêa LT, Muniz GA, Carafinii PHL, Verganii AB, Ferreira KA, Batista LE. Análise multifatorial de métodos volumétricos para a quantificação de ácido ascórbico em comprimidos efervescentes. [Internet]. 2018Oct.31 [cited 2021Feb.23];11(3). Available from: http://autores.revistarevinter.com.br/index.php?journal=toxicologia&page=article&op=view&path[]=376
7. IBGE. Censo Demográfico, 2020. [Internet]. Available from: https://cidades.ibge.gov.br/
8. Ibiapino MK. et al. Serviço de atendimento móvel de urgência: epidemiologia do trauma no atendimento pré-hospitalar. Rev. Fac. Ciênc. Méd. Sorocaba. 2017; 19(2): 725. http://dx.doi.org/10.23925/1984-4840.2017v19i2a5a
9. Cho J, You M, Yoon Y. Characterizing the influence of transportation infrastructure on Emergency Medical Services (EMS) in urban area—a case study of Seoul, South Korea. PloS one, 12(8) (2017). http://dx.doi.org/10.1371/journal.pone.0183241
10. Mendonça MFS, Silva APSC, Castro CCL. Análise espacial dos acidentes de trânsito urbano atendidos pelo Serviço de Atendimento Móvel de Urgência: um recorte no espaço e no tempo. Rev. bras. epidemiol. [Internet]. 2017 Dez [citado 2021 Fev 23] ; 20( 4 ): 727-741. Disponível em: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1415-790X2017000400727&lng=pt. https://doi.org/10.1590/1980-5497201700040014
11. Santos IDC, et al. Miocardiopatia hipertensiva no contexto da atenção primária: um relato de caso. Rev Med Saude Brasilia 2017; 6(Supl.2).
12. Lefundes AAG, et al. Caracterização Das Ocorrências Do Serviço De Atendimento Móvel De Urgência. Revista Baiana de Enfermagem,30(3).(2016). http://dx.doi.org/10.18471/rbe.v30i3.16387
13. Seyyednozadi M, et al. Pre-Hospital Emergency Medical Services: An Epidemiological Survey in Mashhad, Iran. Patient Saf Qual Improv.. 2017; 5(3), p.572-76.
14. Zhang ZHQ, Gou J, Li X. Medida de desempenho para tempo de viagem confiável de veículos de emergência. Pesquisa de Transporte Parte C: Tecnologias Emergentes. 2016; 65: 97–110. http://dx.doi.org/10.1016/j.trc.2016.01.015
15. Ministério da Saúde. Destaques das Atualizações Focadas em Recomendações de 2018 da American Heart Association para RCP e ACE: Suporte Avançado de Vida Cardiovascular e Suporte Avançado de Vida em Pediatria, American Heart Association. 2018.
16. Santos JC, Melo W. Estudo de saúde comparada: os modelos de atenção primária em saúde no Brasil, Canadá e Cuba. Gerais: Revista Interinstitucional de Psicologia. 2018; 11(1), p. 79-98. http://dx.doi.org/10.36298/gerais2019110107
