Influenza A/H1N1 and COVID-19 in Brazil: impacts and epidemiological differences
Influenza A/H1N1 e COVID-19 no Brasil: impactos e diferenças epidemiológicas
Influenza A/H1N1 y COVID-19 en Brasil: impactos epidemiológicos y diferencias
Influenza A/H1N1 and COVID-19 in Brazil: impacts and epidemiological differences
Revista de Epidemiologia e Controle de Infecção, vol. 10, núm. 3, pp. 326-331, 2020
Universidade de Santa Cruz do Sul

Esta obra está bajo una Licencia Creative Commons Atribución 4.0 Internacional.
Recepción: 31 Julio 2020
Aprobación: 07 Octubre 2020
Abstract: Justificative and Objectives: In 2009, Brazil faced the influenza A/H1N1pdm09 pandemic that infected at least 50 thousand people. In 2020, it faces another pandemic caused by the SARS-Cov-2 virus (COVID-19). Because it is a new disease, there is much speculation about it and comparison with other scenarios, often based on fake news. This study compares the impacts and epidemiological differences of Influenza A/H1N1 and COVID-19 in Brazil. Methods: Quantitative, descriptive, epidemiological study, based on documents, whose data were collected on the information platforms of the Brazilian Ministry of Health and the World Health Organization, in addition to scientific articles. The data on Influenza A/H1N1 refer to 2009 and the data on COVID-19 to the period from March to April 30, 2020. Results: It appears that in Brazil, in just two months, the number of cases of COVID-19 (85380) has already exceeded the total cases of influenza A/H1N1pdm09 (50482) that occurred in the whole year of 2009 and caused a triple of deaths. Therefore, COVID-19 is more severe, given the proportions reached in lethality, due to the lack of vaccine and specific treatment of cases. Conclusion: The COVID-19 pandemic is more impactful for Brazil than the influenza A/H1N1pdm09 pandemic.
Keywords: Brazil, Coronavirus Infections, Epidemiology, Influenza A Virus, Public Health.
Resumo: Justificativa e Objetivos: Em 2009, o Brasil enfrentou a pandemia de influenza A/H1N1pdm09 que infectou, pelo menos, 50 mil pessoas. Em 2020, enfrenta outra pandemia causada pelo vírus SARS-Cov-2 (COVID-19). Por se tratar de uma doença nova, há muita especulação sobre a mesma, assim como comparação com outros cenários, muitas vezes com base em informações falsas. Este estudo compara os impactos e diferenças epidemiológicas da Influenza A/H1N1 e COVID-19 no Brasil. Métodos: Estudo quantitativo, descritivo, epidemiológico, de base documental, cujos dados foram coletados nas plataformas de informação do Ministério da Saúde do Brasil e da Organização Mundial da Saúde, além de artigos científicos. Os dados sobre Influenza A/H1N1 referem-se ao ano de 2009 e os de COVID-19 ao período de março a 30 de abril de 2020. Resultados: Constata-se que no Brasil, em apenas dois meses, o número de casos da COVID-19 (85.380) já ultrapassou o total de casos de influenza A/H1N1pdm09 (50.482) ocorridos em todo o ano de 2009 e provocou o triplo de óbitos. Portanto, a COVID-19 apresenta-se de forma mais severa, dada as proporções alcançadas em letalidade, pela falta de vacina e tratamento específico dos casos. Conclusão: The COVID-19 pandemic is more impactful for Brazil than the influenza A/H1N1pdm09 pandemic.
Palavras-chave: Brasil, Infecções por Coronavírus, Epidemiologia, Vírus da Influenza A, Saúde Pública.
Resumen: Justificación y Objetivos: En 2009, Brasil se enfrentó a la pandemia de influenza A / H1N1pdm09 que infectó al menos a 50,000 personas. En 2020, se enfrenta a otra pandemia causada por el virus SARS-Cov-2 (COVID-19). Como se trata de una enfermedad nueva, se especula mucho y se compara con otros escenarios, a menudo basados en información falsa. Este estudio compara los impactos y las diferencias epidemiológicas de la Influenza A / H1N1 y COVID-19 en Brasil. Métodos: Estudio epidemiológico cuantitativo, descriptivo, basado en documentos, cuyos datos fueron recolectados en las plataformas de información del Ministerio de Salud de Brasil y de la Organización Mundial de la Salud, además de artículos científicos. Los datos sobre Influenza A / H1N1 se refieren al año 2009 y los datos sobre COVID-19 al período de marzo al 30 de abril de 2020. Resultados: Parece que en Brasil, en solo dos meses, el número de casos de COVID-19 (85,380) ya excedió el número total de casos de influenza A / H1N1pdm09 (50,482) que ocurrieron en todo el año de 2009 y causaron un triple de muertes. Por lo tanto, COVID-19 se presenta más severamente, dadas las proporciones alcanzadas en la letalidad, debido a la falta de vacuna y al tratamiento específico de los casos. Conclusión: La pandemia de COVID-19 es más impactante para Brasil que la pandemia de influenza A / H1N1pdm09.
Palabras clave: Brasil, Infecciones por Coronavirus, Epidemiología, Virus de la Influenza A, Salud Pública.
INTRODUCTION
Pandemics caused by the influenza A/H1N1pdm09 virus and the new viral strain of the Coronaviridae family (SARS-CoV-2) have brought several repercussions to the world population, due to their speed of transmission and the expressive numbers of attacks and deaths.
The swine influenza A/H1N1pdm09 virus appeared in Mexico in early 2009 and spread rapidly around the world, giving rise to a phase 6 pandemic, declared by the World Health Organization (WHO) on June 11 of the same year1. A year later, the virus was distributed in a total of 214 countries2, there were 50 million confirmed cases in the laboratory and 18 631 deaths3. In Brazil, more than 50000 cases of the disease were confirmed, of which 4% died4.
On February 26, 2020, the first case of COVID-19 was identified in Brazil, according to data from the Ministry of Health5. It is a disease initially identified in China, which spread rapidly among the world population and generated negative impacts on people’s health and the countries’ economy6. The spread of the virus that causes COVID-19 and the ability to control it is still a challenge for health agencies and researchers 7.
In order to minimize the cases and guide the population in the two pandemics, the Brazilian Ministry of Health carried out some coping measures, such as: monitored and disseminated the cases through epidemiological bulletins; trained health professionals to follow protocols to guide them in suspected and confirmed cases; guided the population on preventive measures; in the case of the coronavirus pandemic, it established social distance8.
As COVID-19 is still being investigated for adequate treatment and cure, studies are being carried out for this purpose and with the objective of understanding the behavior of the virus in relation to other known endemic viral diseases.
This situation experienced with the current pandemic motivated the elaboration of this research, which aims to compare the impacts and epidemiological differences of Influenza A/H1N1 and COVID-19 in Brazil.
METHODS
This is a quantitative, descriptive, epidemiological study, based on documents, whose data were collected on the information platform of the Brazilian Ministry of Health (https://coronavirus.saude.gov.br/), in the Influenza Technical Report edition Jan 1, 2012 and the World Health Organization (https://www.who.int/emergencies/diseases/novel-coronavirus-2019).
The extracted data were submitted to descriptive analysis and presented in absolute numbers (cases and number of confirmed deaths). Then, the lethality of each disease was calculated, considering the division of the number of deaths by the number of cases, and were tabulated according to the origin region. The COVID-19 incidence and mortality coefficients were extracted from the aforementioned Ministry of Health portal, referring to the information released on May 1, 2020, and represented graphically by the Federated Unit. Influenza A/H1N1 data refer to 2009 and COVID-19 (cases and number of confirmed deaths) from March to April 30, 2020. This period was selected due to the beginning of diagnosed cases in the country and the coping measures by managers, health professionals and the population.
The study followed the recommendations of Resolution 466/2012 of the Brazilian National Health Council. As the study presents data in the public domain, it was not necessary to submit it for consideration by the ethics committee on research with human beings.
RESULTS
| Area | Confirmed Cases | Deaths and(Lethality rate %) | ||
| H1N1 (2009)* | COVID-19** | H1N1 (2009)* | COVID-19** | |
| Brazil | 50.482 | 85.380 | 2.060 (4.0) | 5.901 (6.9) |
| Region | ||||
| North | 868 | 10772 | 50 (5.76) | 712 (6.6) |
| Northeast | 846 | 24518 | 62 (7.32) | 1536 (6.2) |
| Southeast | 12104 | 42443 | 992 (8.19) | 3394 (7.9) |
| South | 35397 | 4958 | 789 (2.22) | 180 (3.6) |
| Middle-West | 1267 | 2689 | 167 (13.1) | 79 (2.9) |
**COVID-19 data from February to April 30, 2020.
Table 1 allows viewing the morbidity statistics for the two pandemics and shows the distribution of cases and deaths by region. It is observed that in just two months of registration of COVID-19 the number of cases has already exceeded the total cases of influenza A/H1N1pdm09 that occurred in 2009 (50482 of H1N1 with a lethality rate (LR) of 4%, against 85380 of COVID-19 and LR equal to 6.9%). The number of registered deaths is almost triple.
Considering the number of cases and the lethality of the two diseases, two regions stand out. In the South region, in 2009, a total of 35397 cases of influenza A/H1N1pdm09 were confirmed (seven times the number of COVID-19 cases registered until April 30, 2020). However, the lethality for COVID-19 was higher than influenza. In the Central-West region, the number of cases of influenza A/H1N1pdm09 was lower than that of COVID-19, but the lethality rate was the highest in the country (13.1%), and in the aforementioned date of the study it presented the lowest rate of COVID-19 (Table 1).
It is observed that the distribution of deaths by COVID-19 is not homogeneous in the country. It is noticed that deaths are more concentrated in the Southeast and Northeast regions. However, the lethality rate in the North is higher than in the Northeast, and the rate in the Southeast exceeds that of Brazil (Table 1).
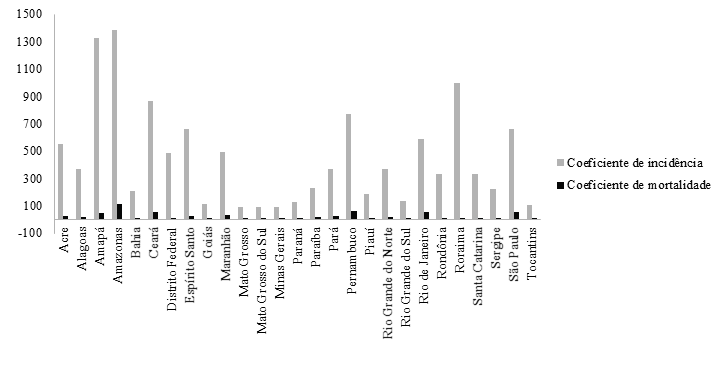
Figure 1
Incidence and mortality coefficients by COVID-19/1 million inhabitants according to Brazilian Federated Units.
Figure 1 shows the distribution of the coefficients of incidence and mortality in cases of COVID-19. There was a disparity in all states in the five Brazilian regions with regard to the incidence coefficients, when compared with the mortality coefficients. This context was also found in Sao Paulo, located in the Southeast region, considered as the state with the largest number of the country's population and cases of COVID-19.
Looking at the coefficients in more detail, it was noticed that the incidence of cases was concentrated in most states located in the North region, which is composed of a total of seven states, but Amazonas (1381/1 million inhabitants), Amapa (1325/1 million inhabitants) and Roraima (994/1 million inhabitants) stand out (Figure 1).
In Figure 1, it was also noticed that the Northeast had a significant number of cases in Ceara, with an incidence of 863/1 million inhabitants and Pernambuco (767/1 million inhabitants). And the Brazilian region that had the lowest incidence was the Central-West, which probably was due to the lowest population density in the three states: Mato Grosso, Mato Grosso do Sul and Goias.
DISCUSSION
The pandemic caused by the A/H1N1 influenza virus killed around 12 800 people in 2009, worldwide. Of these, 2 051 deaths were reported in Brazil and more than 50 thousand confirmed cases of the disease. The main Brazilian regions that had the highest incidence were the South and Southeast.6
In December 2019, a series of cases of pneumonia caused by a β-coronavirus identified in Hubei province, Wuhan, China, were reported.9 On January 12, 2020, the disease was named COVID-19 and on March 11 this year a pandemic state was declared.10
Assessments of the potential for spreading the disease to other countries, based on the number of infected people in January 2020 in China, estimated that the basic reproductive number (R0) was 2.2. This indicated that an infected person could transmit the virus, on average, to two more susceptible people. However, the detection and increase in the number of domestic cases in other regions outside China suggested that the disease would continue to increase in number, and that this risk was probably higher.11
Thus, accelerated by human migration, exported cases were reported in several regions of the world, including Europe, Asia, North America and Oceania12, and by May 25, 2020, a total of 5307298 cases of COVID-19 were confirmed in 216 countries, with 342070 deaths.10
The COVID-19 pandemic is more severe due to the high rates of transmissibility and pathogenicity of the virus. This is partly due to the ease of aerial transmission and fomites; the long incubation period, which can vary from 0-24 days13; the possibility of asymptomatic manifestations14; the time of viability of the virus in the environment, which remains for three hours in aerosols and for up to 72 hours in plastic and stainless steel.15
In Brazil, from the first cases of COVID-19, proliferation was alarming. Without specific treatment or vaccine, the main measure to contain the transmission of the disease was social isolation, with the aim of preventing a collapse in health, generated by the accumulation of cases in hospitals.16 This measure was not adopted during the influenza A pandemic. H1N1pdn09 and, even so, the number of cases and deaths from the disease was considerably lower.
Regarding the cases diagnosed by age group, it was found in the literature that the H1N1 pandemic affected proportionately more children and young adults than other age groups in the population.17 A study conducted in the city of Rio de Janeiro, with a total of 1191 cases of severe acute respiratory syndrome (SARS) due to H1N1, demonstrated that: 60.3% occurred in women, 185 pregnant women; 48.1% in children under 20 years old; regarding deaths, 75.1% occurred with the adult population between 20 and 59 years old. As for comorbidities, chronic heart disease, metabolic disease, smoking and immunosuppression stood out.18 Interestingly, in Brazil, the distribution of confirmed H1N1 cases of SARS was 42.4% in people aged 10 to 29 years old and 5.1 % of people aged 60 or over, with the most common comorbidities being pneumopathies, followed by chronic heart diseases.19
Like H1N1, COVID-19 can affect people of any age, as well as cause death. However, according to the CEO's Epidemiological Bulletin No. 14 (April 2020), 70% of the patients who died were aged over 60 years old and 67% had at least one of the comorbidities configured as a risk factor. The main one was cardiomyopathy (present in 1566 deaths), followed by diabetes (in 1223 deaths), kidney disease (296), pneumopathy (279) and neurological disease (265). Obesity is also considered a risk factor, regardless of age.20
In addition to the aforementioned factors that contribute to deaths, the conditions of hospital infrastructure are indispensable for reducing mortality from COVID-19. Infected by the virus with severe evolution, they have severe pneumonia with respiratory failure, leading to the need for hospitalization and mechanical ventilation.
A study carried out in China showed that in patients affected by COVID-19, at least 81% had respiratory symptoms. Of these, 14% had moderate symptoms - desaturation, dyspnea, oxygenation index below 300 and/or pulmonary infiltrates compromising above 50% of the parenchyma; and 5% progressed to acute respiratory failure, septic shock and multiple organ failure.21
A study showed that the age group of people affected by the Influenza A/H1N1pdm09 virus in Brazil, in 2009, was predominant in children under 2 years old and adults aged between 20 and 29 years old.6 On the other hand, data on the age group of people affected by COVID-19, in the literature investigated in this study, are in accordance with the main international statistics, which indicate the age above 60 years old.22
On the incidence and mortality rates: the result of the disparity in the Brazilian regions may be related to the non-compliance with the isolation measures and the use of masks with the increase of cases in people of different ages. In addition to the possible delay in diagnosis to confirm death and the peculiarities of each region of the country.8
In the north region of the country, it is common to find some diseases considered endemic, such as malaria, dengue, leprosy and others, which affect and increase the vulnerability of the resident and circulating population. They may be associated with the fact that the region is located in a geographic area favorable for these diseases and because it has a large industrial park in the electro-electronic sector, which promotes import and export trade and the increase in the migratory and visitor flow. This spatial configuration has repercussions on the dynamics of health problems, on social aspects and on economic inequalities of the people who live in the cities registered.23
In addition, the region concentrates the worst rates of use of health services in the country, facing low availability of physicians (1/1000 inhabitants), which is seven times lower than that found in the capitals in the South of the country (7.1/1000). In addition to the difficult applicability of policies instituted by the federal government, which suffer from low institutionality, discontinuity and limited sensitivity to regional specificities that are aggravated in times of pandemic.24
In the Northeast region, which concentrates the largest number of states in the country, in a total of nine, there is still another aggravating factor, which is the large population in unfavorable conditions, which enables the development of diseases and conditions.25
The other regions, mainly the South and Southeast, concentrate the highest population density, also reflecting on the social, economic, cultural and health conditions of their residents.
We conclude that the COVID-19 pandemic is more impactful for Brazil than the influenza A/H1N1pdm09 pandemic. Despite the intervention measures adopted, the main one being social isolation, the disease has reached catastrophic proportions, especially in some states. Perhaps becoming the main challenge for national public health in the 21st century.
REFERENCES
1. World Health Organization. World now at the start of 2009 influenza pandemic. 2009. [citado 2020 mar. 26]. Disponível em: http://www.who.int/mediacentre/news/statements/2009/h1n1_pandemic_phase6_20090611/em/
2. Boëlle PY, Ansart S, Cori A, et al. Transmission parameters of the A/H1N1 (2009) influenza virus pandemic: a review. Influenza and other respiratory viruses. 2011; 5 (5): 306-316. https://dx.doi.org/10.1111/j.1750-2659.2011.00234.x
3. Greninger AL, Chen EC, Sittler T, et al. A metagenomic analysis of pandemic influenza A (2009 H1N1) infection in patients from North America. PLoS One. 2010;5(10):e13381. https://doi.org/10.1371/journal.pone.0013381
4. Ministério da Saúde. (BR). Secretaria de Vigilância em Saúde. Informe Técnico de Influenza. Vigilância de Síndrome Respiratória Aguda Grave (SRAG), de Síndrome Gripal (SG) e de Internações por CID J09 a J18 1. ed.
5. Ministério da Saúde. (BR). Coronavírus Brasil; 2020.
6. Silveira MR, Felipe Junior NF, Cocco RG, et al. Novo coronavírus (Sars-CoV-2): difusão espacial e outro patamar para a socialização dos investimentos no Brasil. Revista Brasileira de Estudos Urbanos e Regionais. 2020; 22(1)::e202024. https://dx.doi.org/10.22296/2317-1529.rbeur.202024pt
7. Barroso BIL, Souza MBCA, Bregalda MM, et al. A saúde do trabalhador em tempos de COVID-19: reflexões sobre saúde, segurança e terapia ocupacional. Cad. Bras. Ter. Ocup. 2020; 28(3):1093-1102. https://doi.org/10.4322/2526-8910.ctoarf2091
8. Oliveira WK, Duarte E, França GVA, et al. Como o Brasil pode deter a COVID-19. Epidemiol. Serv. Saúde. 2020;29(2): e2020044. https://doi.org/10.5123/s167949742020000200023
9. Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. 2020; 382(1):1199-1207. https://dx.doi.org/10.1056/NEJMoa2001316
10. World Health Organization. Coronavirus disease (COVID-19) outbreak situation. 2020.
11. Liu Y, Gayle AA, Wilder-Smith A, et al. The reproductive number of COVID-19 is higher compared to SARS coronavirus. Journal of Travel Medicine. 2020;27(2):1-4. https://dx.doi.org/10.1093/jtm/taaa021
12. Anzai A, Kobayashi T, Linton NM, et al. Assessing the Impact of Reduced Travel on Exportation Dynamics of Novel Coronavirus Infection (COVID-19). J Clin Med. 2020; 9(601):1-9. https://dx.doi.org/10.3390/jcm9020601
13. Guan WJ, Ni ZY, Hu Y, et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020;382(18):1708‐1720. https://dx.doi.org/10.1056/NEJMoa2002032
14. Bai Y, Yao L, Wei T, et al. Presumed asymptomatic carrier transmission of COVID-19. Jama. 2020; 323(14):1406-1407. https://dx.doi.org/10.1001/jama.2020.2565
15. Doremalen NV, Morris DH, Holbrook MG, et al. Aerosol and surface stability of HCoV-19 (SARS-CoV-2) compared to SARS-CoV-1. The New England Journal of Medicine. N Engl J Med. 2020; 382:1564-1567. https://dx.doi.org/10.1056/NEJMc2004973
16. Silva AAA. Sobre a possibilidade de interrupção da epidemia pelo coronavírus (COVID-19) com base nas melhores evidências científicas disponíveis. Rev Bras Epidemiol. 2020: 23(1):200021. https://doi.org/10.1590/1980-549720200021
17. Punpanich W, Chotpitayasunondh T. A review on the clinical spectrum and natural history of human influenza. Int J Infect Dis. 2012;16(10):e714-23. https://dx.doi.org/10.1016/j.ijid.2012.05.1025
18. Felinto GM, Escosteguy CC, Medronho RDA. Factors associated with death of severe cases of influenza A (H1N1) pdm09. Cadernos Saúde Coletiva, 2019; 27(1), 11-19. https://dx.doi.org/10.1590/1414-462x201900010433
19. Ministério da Saúde. (BR). Secretaria de Vigilância em Saúde. Influenza pandêmica (H1N1) 2009 - análise da situação epidemiológica e da resposta no ano de 2009. Boletim Eletrônico Epidemiológico. 2010;10(2):1-21.
20. Ministério da Saúde. (BR). Secretaria de Vigilância em Saúde. Boletim epidemiológico especial COE-COVID19. 2020; 14: SE18-26 de abril.
21. Zhang H, Penninger JM, Li Y, et al. Angiotensin-converting enzyme 2 (ACE2) as a SARS-CoV-2 receptor: molecular mechanisms and potential therapeutic target. Intensive Care Med. 2020; 46(1): 586–590. https://dx.doi.org/10.1007/s00134-020-05985-9
22. Meng J, Xiao G, Zhang J, et al. Renin-angiotensin system inhibitors improve the clinical outcomes of COVID-19 patients with hypertension. Emerg Microbes Infect. 2020; 9(1):757-760. https://dx.doi.org/10.1080 / 22221751.2020.1746200
23. Lobão MSP, Correa AS, Schneider MB. Região Norte do Brasil e sua inserção no comércio internacional brasileiro. Interações (Campo Grande). 2017;18(2):87-101. https://dx.doi.org/10.20435/inter.v18i2.1433
24. Garnelo L, Lima JG, Rocha ESC, et al. Acesso e cobertura da Atenção Primária à Saúde para populações rurais e urbanas na região norte do Brasil. Saúde debate. 2018;42(1):81-99. https://dx.doi.org/10.1590/0103-11042018S106
25. Lima DLF, Dias AA, Rabelo RS, et al. COVID-19 no Estado do Ceará: Comportamentos e crenças na chegada da pandemia. Cien. Saúde Colet. 2020;25(5):1575-86. https://dx.doi.org/10.1590/1413-81232020255.07192020