Ventilator-associated pneumonia: scientific evidence
Pneumonia associada à ventilação mecânica: evidências científicas
Neumonía asociada al ventilador: evidencia científica
Ventilator-associated pneumonia: scientific evidence
Revista de Epidemiologia e Controle de Infecção, vol. 10, núm. 3, pp. 345-351, 2020
Universidade de Santa Cruz do Sul

Esta obra está bajo una Licencia Creative Commons Atribución 4.0 Internacional.
Recepción: 21 Diciembre 2019
Aprobación: 24 Julio 2020
Abstract: Background and objectives: to identify factors related to the prevention of ventilator-associated pneumonia in patients of intensive care units. Method: this is an integrative review with searches for studies that presented factors related to the disease in question, in the LILACS, MEDLINE, SCOPUS and BDENF databases, between 2007 and 2016. The final sample consisted of nine studies that addressed as protective factors: maintenance of headboard elevation between 30° and 45°, oral hygiene with chlorhexidine, aspiration prior to decubitus change and adoption of Subglottic Aspiration System. Conclusion:the knowledge about risk factors and the application of preventive measures can contribute to reduce the incidence of this disease in the intensive care environment.
Keywords: Cross Infection, Bacterial pneumonia, Infection control, Protective factors, Intensive Care Units.
Resumo: Justificativa e Objetivos: identificar os fatores relacionados à prevenção de Pneumonia Associada à Ventilação Mecânica em pacientes de unidades de terapia intensiva. Método: revisão integrativa com buscas, nas bases de dados LILACS, MEDLINE, SCOPUS e BDENF, entre 2007 e 2016, por estudos que apresentassem fatores relacionados ao desenvolvimento da pneumonia em questão. A amostra final foi composta por nove estudos que abordaram como fatores de proteção a manutenção da cabeceira elevada entre 30° e 45°, a higiene oral com clorexidina, a necessidade de aspiração prévia à mudança de decúbito e a adoção de sistema de aspiração subglótica. Conclusão: o conhecimento sobre os fatores de risco e a aplicação de medidas preventivas podem contribuir para reduzir a incidência deste agravo no âmbito intensivo.
Palavras-chave: Infecção hospitalar, Pneumonia bacteriana, Controle de infecções, Fatores de Proteção, Unidades de Terapia Intensiva.
Resumen: Justificación y Objetivos: identificar los factores relacionados con la prevención de la neumonía asociada al ventilador en pacientes en unidades de cuidados intensivos. Método: revisión integradora con búsquedas en las bases de datos LILACS, MEDLINE, SCOPUS y BDENF, entre 2007 y 2016, de estudios que tratan de los factores asociados al desarrollo de la referida neumonía. La muestra se compuso de nueve artículos, que abarcan como factores protectores el mantenimiento elevado de la cabecera entre 30° y 45°, la higiene oral con clorhexidina, la necesidad de aspiración antes del cambio de decúbito y la adopción del sistema de aspiración subglótica. Conclusiones: el conocimiento sobre los factores de riesgo y la aplicabilidad de medidas preventivas pueden contribuir a la reducción de la incidencia de este problema en el área intensiva.
Palabras clave: Infección Hospitalaria, Neumonía bacteriana, Control de infecciones, Factores Protectores, Unidades de Cuidados Intensivos.
INTRODUCTION
Healthcare-associated infections (HAI) are any infections associated with care, therapeutic and/or diagnostic procedures that affects individuals in hospital and nonhospital settings. To organize the Brazilian scenario, the National Health Surveillance Agency (Anvisa) revised in 2017 the measures to prevent HAI such as ventilator-associated pneumonia (VAP), healthcare associated urinary tract infection (HAUTI), catheter-related bloodstream infection (CRBSI) and surgical site infection (SSI)1.
In Intensive Care Units (ICU), VAP ranks second in HAI records, a fact that strengthens the importance of adopting emerging preventive measures for this condition. Recent studies show that VAP incidence is concerning in developed and developing countries alike. In USA, PAV density is estimated to be 5 to 10 cases for every thousand days of mechanical ventilation. Regarding the Brazilian ICU scenario, the data available are inaccurate and do not reliably contextualize the national incidence.1,2
The establishment of preventive measure bundles emerged from discussions related to quality of care and patient safety to prevent HAI. Bundles aimed at VAP prevention were thus proposed to guide the teams that assist individuals in mechanical ventilation and disseminated through educational activities1.
International studies have revealed the importance of implementing educational activities through preventive bundles of measures to reduce VAP in several countries, such as South Korea, Spain, USA, Argentina and Egypt. However, despite the continental application of bundles, high VAP rates are still observed worldwide, either in developing or developed countries. This can increase the patient’s hospitalization time, generating costly monetary implications for the services, in addition to favoring the proliferation of multidrug-resistant microorganisms that raise the mortality rates caused by this infectious process.1,3-6
Brazilian studies record similar VAP rates in different regions and highlight the implementation of preventive bundles as effective strategies to prevent this disease. In a study conducted in Southern Brazil, the VAP rate prior to the implementation of bundles was 49.6% and, after the educational intervention, 17.5%3.
The main VAP risk factors indicated by literature are: mechanical ventilation time longer than five days, leading to use of tracheostomy;16.19 unplanned extubation, which may culminate in reintubation; diet by nasoenteral tube with gastric positioning, combined with non-use of the headboard elevation from 30º to 45º; and use of previous antibiotic therapy, with the combination of three or more antimicrobials.7,8,10-12
Regarding protective factors, international literature indicates: maintenance of headboard elevation between 30° and 45°; use of a tube with Subglottic Aspiration System; oral aspiration prior to decubitus change; oral hygiene with chlorhexidine, at least three times a day; early withdrawal of sedation, combined with planned extubation; cuff pressure of up to 30 cmH.O; and hand sanitization. 4,6,14-17
Although the protective factors are implemented in other countries, such measures are still poorly conducted in Brazil, for example, the Subglottic Aspiration System. Given this context, the need to adopt effective protective measures to reduce VAP in ICU, in accordance with the most recent international guidelines. Thus, this study sought to identify the factors indicated by the literature related to VAP prevention in ICU patients.
METHODS
This is an integrative literature review, a research method used in the context of Evidence-Based Practice (EBP), where the objective is to synthesize results obtained through studies on a given topic, providing broad information about the subject/problem and seeking to promote integration between scientific research and care practice.18,19
The integrative method steps are didactically distributed as: Phase I: identification of subject and selection of the research hypothesis or question; Phase II: criteria establishment for inclusion and exclusion of studies or search in the literature; Phase III: definition of information that can be extracted from the selected studies, in line with the guiding question of the review; Phase IV: assessment of the studies included in the integrative review; Phase V: results interpretation; Phase VI: presentation of the review/synthesis of knowledge.18,19
Studies were selected through electronic search of primary study articles that answered the following research question: what protective and risk factors are reported by national and international literature and are related to ventilator-associated pneumonia in intensive care units?
Articles included had to be published in full, resulting from experimental, quasi-experimental, cohort and case-control research projects, in Portuguese, English and Spanish language, published between 2007 and 2016. Articles with inconsistent statistical data analysis were excluded.18,19
The search was made on the following databases: Latin American and Caribbean Literature in Health Sciences (LILACS), Medical Literature Analysis and Retrieval System Online (MEDLINE/PubMed), SciVerse (SCOPUS) and the Brazilian Nursing Database (BDENF). The descriptors adopted in the search were extracted from the Health Sciences Descriptors (DeCS) and Medical Subject Headings (MeSH).
In the LILACS database, searches were made using the descriptors “pneumonia associada à ventilação mecânica” (“ventilator-associated pneumonia”) and “pneumonia bacteriana” (“bacterial pneumonia”) in isolation, whereas the descriptors “prevenção & controle” (“prevention & control”) and “infecção hospitalar” (“hospital infection”) were searched in combination. In the MEDLINE/PubMed and SCOPUS databases, the searches were made with the following combinations: “pneumonia,associated-ventilator” and “health profissional”; “pneumonia,associated-ventilator” and “epidemiological monitoring”; “pneumonia,associated-ventilator” and “cross infection” and “health profissional”; “pneumonia,associated-ventilator” and “cross infection” and “prevention & control”. Regarding the search in the BDENF, the descriptors used were “Pneumonia Associada à Ventilação Mecânica” (“Ventilator-associated pneumonia”), in isolation, and the following combinations: “Pneumonia Associada à Ventilação Mecânica” and “Prevenção & Controle” (“Prevention & Control”); “Pneumonia Associada à Ventilação Mecânica” and “Monitoramento Epidemiológico” (“Epidemiological Monitoring”); “Pneumonia Associada à Ventilação Mecânica” and “Saúde Profissional” (“Professional Health”). The Boolean operator AND was used in all combinations.
The flowchart Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) was used to present the systematic search and selection of the studies. Data combinations and analysis occurred between June and December 2017 and were performed independently by three researchers, one of which was selected to verify the conflicts. Articles that did not meet the inclusion criteria were excluded after title and abstract reading. Figure 1 shows the crossing results.19
After the searches, selected articles were read in full considering the pre-established research question. From this perspective, the findings allowed us to list the evident analytical categories in the studies that composed this review.
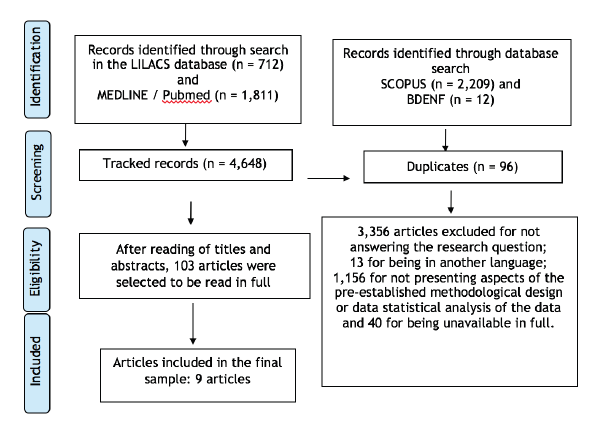
Figure 1
Diagram representing the selection of articles for review.
RESULTS
After searching the databases, the findings were systematized in two tables. The first describes the studies characterization and the second describes the VAP-related protection and risk factors.
| Authors | Titles | Bases | Institutions |
| Quenot et al. (2007).16 | Effect of a nurse-implemented sedation protocol on the incidence of ventilator-associated pneumonia. | MEDLINE | Hospital in Dijon, France. |
| Chao et al. (2008).15 | Removal of oral secretion prior to position change can reduce the incidence of ventilator-associated pneumonia for adult ICU patients: a clinical controlled trial study. | MEDLINE | Hospital in Taiwan. |
| Kollef et al. (2008).20 | Silver-coated endotracheal tubes and incidence of ventilator-associated pneumonia. | MEDLINE | US hospitals. |
| Rello et al. (2013).3 | A care bundle approach for prevention of ventilator-associated pneumonia. | MEDLINE | Hospitals of Catalonia. |
| Gopal. et al. (2014).14 | Significant reduction in ventilator-associated pneumonia with the Venner-PneuX System in high-risk patients undergoing cardiac surgery: the low ventilator-associated-pneumonia study. | MEDLINE | UK hospitals. |
| Azab et al. (2015).6 | Reducing ventilator-associated pneumonia in neonatal intensive care unit using "VAP Prevention Bundle": a cohort study. | SCOPUS | University Hospitals of Egypt. |
| Talbot et al. (2015).4 | Sustained Reduction of Ventilator-Associated Pneumonia Rates Using Real-Time Course Correction With a Ventilator Bundle Compliance Dashboard. | SCOPUS | University Hospitals in the US. |
| Tsai et al. (2008).21 | Intermittent Suction of Oral Secretions Before Each Positional Change may Reduce Ventilator-Associated Pneumonia: a pilot study. | SCOPUS | Hospitals in Taiwan. |
| Nseir et al. (2007).13 | Relationship between tracheotomy and ventilator-associated pneumonia: a case-control study. | SCOPUS | University Hospital in France. |
| Authors | Objective | Type of Study, Level of Evidence and Sample | Protective factors |
| Quenot et al. (2007).16 | To implement an effective sedative management protocol for patients using MV. | Case-control. LE: 4. A total of 423 patients using MV for more than 48 hours, 226 in the control group and 197 in the case. The VAP rate was 6% in the case and 15% in the control. | Reduction of sedation at every 3 hours (95%CI 2.1-9.5; p-value=0.001); ICU time < 5 days (95%CI 2.5-13; p-value=0.004). |
| Chao et al. (2008).15 | To evaluate the effect of oral secretion removal in reducing VAP incidence, before changing the patients position. | Randomized clinical trial. LE: 2. 102 patients comprised the case group and 159 the control group. Rate of 4.9% in the case group and 15.1% in the control group. | Aspiration of secretion from the oral cavity before decubitus change (RR: 0.32; 95%CI 0.11-0.92; p-value<0.05). |
| Kollef et al. (2008).20 | To determine whether the silver-coated endotracheal tube reduces VAP incidence. | Randomized clinical trial. LE: 2. A total of 9,417 adult patients using MV, from 54 US intensive care centers, between 2002 and 2006. Among the patients using the silver-coated orotracheal tube, 4.8% had VAP, which also occurred with 7.5% of patients using conventional tubes. | Use of silver-coated orotracheal tube (95%CI 14.6-81.9; p-value = 0.0005). |
| Rello et al. (2013).3 | To evaluate VAP preventive measures. | Cohort. LE: 3. A total of 1,034 patients, of which 149 represented baseline and 885 did so after the intervention. The previous VAP rate was 16% and after the intervention was increased to 11%. | Hands satinization before airway manipulation (OR: 0.35;95%CI 0.11-0.68); Cuff pressure (or: 0.21; 95%CI 0.25-0.92); Oral hygiene with chlorhexidine, (OR: 0.23; 95%CI 0.17-0.75). |
| Gopal. et al. (2014).14 | To evaluate whether the subglottic suction endotracheal tube system was associated with reduced VAP when compared to the standard endotracheal tube. | Randomized clinical trial. LE: 2. A total of 240 patients, 120 with conventional tube and 120 with subglottic suction tube. The incidence in the group with subglottic suction tube was 10.8%, and 21% in the group with conventional tube. | Use of endotracheal tube with subglottic suction (OR: 0.45; p-value=0.03). |
| Azab et al. (2015).6 | To evaluate the effectiveness of the Ventilator-associated pneumonia protective bundle | Case-control LE: 4 143 neonates using MV for more than 48 hours participated in the study, 62 in the control group 81 in the case. The study was conducted in two phases: Phase 1 – verification of incidence prior to intervention; and Phase 2 –after the bundle implementation. In Phase 1, the VAP rate was 67.8%, corresponding to 36.4 episodes/1,000 patients using MV. In Phase II there was a reduction to 38.2%, that is, 23 episodes / 1,000 patients using MV. | Reduction of VAP incidence (RR: 0.565; 95%CI: 0.40-0.78; p-value=0.0006). From the preventive measures: headboard elevation to 30°-45°; education related to hand sanitization; aseptic handling of ventilatory assistance equipment during aspiration; oral hygiene with saline solution and sedation reduction. |
| Talbot et al. (2015).4 | To implement a measures bundle, in real time, to reduce ventilator associated complications. | Quasi-experimental. LE: 3. The participants were patients admitted to ICU between 2005 and 2008. The study was conducted in two phases: Phase 1 – verification of incidence prior to intervention; and Phase 2 – after the bundle implementation. The VAP rate before the intervention was 19.5% and 9.2% after. | Before the bundle implementation, there was a 19.5% incidence (95%CI: 2.64-3.92) and after 9.2% (95%CI: 0.14-0.30; p-value=0.04). Prevention measures: prophylaxis of peptic ulcer, prophylaxis of venous thrombosis, planned extubation, headboard elevation to 30° and oral hygiene. |
| Tsai et al. (2008).21 | To evaluate the use of oral secretions intermittent suction before each position change in VAP reduction. | Case-control. LE: 4. The participants were patients who used MV for more than 72 hours, between 2004 and 2005, 237 in the control group and 227 in the case group. There was a reduction of 26 VAP episodes in the control group and 6 in the case group. | Use of the oral secretion suction system before decubitus change (OR: 0.25; 95%CI: 0.101-0.624, p-value=0.003). |
| Nseir et al. (2007).13 | To determine the relation between tracheostomy and VAP. | Case-control. LE: 4. A total of 177 patients in the case group and 177 in the control group, analyzed between the years 1996 and 2001. The VAP incidence in the control group was 9.2/1,000 and in the case group 4.8/1,000. | Tracheostomy (OR: 0.18; 95%CI: 0.1-0.3; p-value=0.001). |
All studies were conducted in hospitals, more precisely in adult ICU. Among them, two were held in the American continent, specifically in the US, four in Europe (two in France, one in the UK and one in Spain) and three in Asia (two in Taiwan and one in Egypt). All articles were published in international journals. We note that three are randomized controlled clinical studies, one is a non-randomized (quasi-experimental) clinical study, there is one cohort study and four case-control studies.
DISCUSSION
The following protective measures were listed in the included studies: headboard elevation with an angle range between 30° and 45°; maintenance of the ventilation circuit free of visible dirtness,5 sterilization assurance of reprocessing circuits; maintainance of cuff pressure between 20 and 30 cmH.O; oral hygiene with chlorhexidine 0.12 per cent at least three times a day; oral hygiene using only a saline solution and hand sanitization before and after contact and manipulation of the patient’s airway; gradual and early decrease os sedation at every three hours; planned extubation to prevent reintubation; silver coated orotracheal tube; use of pipe with intermittent subglottic suction system, so as to prevent secretions accumulation above the cuff; oral secretions removal prior to position change; early extubation, that is, withdrawal of orotracheal tube in less than 48 hours; prophylaxis and treatment of peptic ulcer disease, and prophylaxis and treatment for venous thrombosis.4,6,7,10,11,14-16,21
From our findings, the maintenance of headboard elevation between 30°-45°, ventilation circuit free of dirtness, cuff pressure up to 30 cmH.O, oral hygiene with antiseptic solution (chlorhexidine), gradual reduction of sedation and planned extubation are strongly recommended measures are notable measures, all in line with North American, European and Brazilian guidelines.1,2,22
The sterilization assurance of reprocessable circuits was mentioned only in the Brazilian guideline, possibly due to the use of reprocessable and thermosensitive circuits in several health institutions. Oral hygiene using antiseptics was widely recommended, in line with the Irish guideline, which suggests using chlorhexidine between 0.12% and 2% every six hours. The cuff pressure and the tube position must be measured before conducting oral hygiene, as well as at the end, conducting subglottic aspiration so that the aspiration is effective, avoiding the risk of trachea injury1.
Regarding the use of aspiration to remove oral secretion before decubitus change, although cited in two studies conducted with critical patients in Taiwan, the procedure is not recommended in the European guidelines. Such a protective measure is indicated by the American Thoracic Society, which understands it as part of the modifiable risk factors, subject to implementation and without burden to the health service, and should therefore be strongly encouraged.2,15,21
Early extubation, less than 48 hours after intubation, was also referred to as a protective measure. However, constant assessments of the patient’s clinical condition are necessary for the use of this measure in order to avoid reintubations, since these interventions are regarded as VAP risk increasers.1,16,22-24
It should be noted that orotracheal reintubation was considered a risk factor in several studies. However, different scenarios must be considered. The second intubation was considered a risk factor when related to the absence of extubation planning or to the inherent complications of severe patients clinical condition. Thus, the extubation planning, including early weaning, lasting 24 to 48 hours, and the evaluation of sedatives reduction, can be important preventive measures to avoid new intubations.1,7,10,12-14,22-24
Regarding the prophylaxis of peptic ulcer, although prevention with H. antagonists and proton pump inhibitors is considered a protective factor due to local pH reduction, this measure potentiates the action of Clostridium difficile, compromising the gastric mucosa, and should therefore be evaluated with caution. Similarly, it is known that prophylaxis of Deep Vein Thrombosis (DVT), with no direct relation to VAP prevention, positively impacts the reduction of hospitalization time and hospital mortality. However, in the context of VAP prevention, studies have shown that it can favor mucosal bleeding emergence and potentiate existing bleeding, so that both measures were withdrawn from international consensus as of 2010.15, 23, 24
Regarding tracheostomy, although a study conducted in France showed that the practice was related to the VAP prevention, more recent studies and with more representative samples found the practice was associated with greater VAP occurrence.1,9,13
In the context of conditions that tend to favor colonization, national and international studies often indicate that low adherence to oral hygiene practices with chlorhexidine is a risk factor for oropharynx and stomach colonization, and consequent VAP development.6,7,10,22-24
Hand sanitization was another measure cited as part of interventional actions to control and reduce VAP. However, national and international studies have shown that the frequency of such practice is considerably inferior to desirable, possibly due to preventing factors such as the lack of adequate physical structure.1,6,7,17,22-24
In this context, it is known and recommended by the World Health Organization (WHO) that hand sanitization occurs in five main moments: before contact with the patient; before aseptic procedures; after risk of exposure to body fluids; after contact with the patient; and after contact with areas close to the patient. Therefore, the WHO encourages health education based on multimodal strategies to ensure greater adherence of professionals to the practice of hand sanitization, since it is the simplest and most effective measure to control HAI.24
CONCLUSION
From the data recovered in this study, we could conclude that several opinions regarding VAP-associated risks and preventive measures against it exist. However, the following measures should be highlighted as common preventive interventions outlined by most studies: extubation planned to avoid reintubation; sedation evaluation and reduction as part of extubation planning; aseptic oral and endotracheal aspiration before decubitus change, especially when there is no routine measurement of cuff pressure; maintenance of headboard elevation between 30° and 45°; oral hygiene with 0.12% to 2% chlorhexidine; and sterilization of reprocessing ventilatory circuits or utilization of single-use circuits.
When considering public health policies to reduce VAP in Brazil, a major challenge is the need for extensive investment in scientific research that enables HAI-reducing strategies, since most of the international strategies in the literature recommend the use of technologies/devices that do not fit the current characteristics of the country’s health system given the high costs associated with acquisition and implementation.
However, the existence of measures to minimize risks and ensure patient safety was noteworthy, implementing, in addition to the previous preventive measures, interdisciplinary and interprofessional actions, considering the responsibility each health professional has in the promotion, prevention, recovery and rehabilitation of individual and community health.
As a limitation of this study, we identified gaps that still need to be explored through investment in research that addresses the subject, so a consensus on the best recommended practices for VAP prevention can be reached, in addition to the need of encouraging interprofessional protagonism, in the face of the responsibility each professional area in critical patient care bears. Thus, this study did accomplish its objective regarding the survey of Brazilian and international literature production on VAP-related protective and risk factors.
REFERENCES
1. Brasil. Agência Nacional de Vigilância Sanitária. Medidas de Prevenção de Infecção Relacionada à Assistência à Saúde. Brasília: ANVISA; 2017.
2. American Thoracic Society. Guidelines for the Management of Adults with Hospital Acquired, Ventilator-Associated, and Health-care Associated Pneumonia. Am J Respir Crit Care Me, 2005; 171(1):388-416. https://dx.doi.org/10.1164/rccm.200405-644ST
3. Rello J, Afonso E, Lisboa T, Ricard M, Balsera B, Rovira A, Valles J, et al. A care bundle approach for prevention of ventilator-associated pneumonia. Clinical Microbiology and Infection. 2013;19(4):363-9. https://dx.doi.org/10.1111/j.1469-0691.2012.03808.x
4. Talbot TR, Carr D, Parmeley CL, Martin BJ, Gray B, Ambrose A, Starmer J. Sustained Reduction of Ventilator-Associated Pneumonia Rates Using Real-Time Course Correction With a Ventilator Bundle Compliance Dashboard. Infect Control Hosp Epidemiol. 2015;36(11):1261-7. https://dx.doi.org/10.1017/ice.2015.180
5. Cristofano A, Peuchot V, Canepari A, Franco V, Perez A, Eulmesekian P. Implementation of a Ventilator-Associated Pneumonia Prevention Bundle in a Single PICU. Pediatric Critical Care Medicine. 2016;17(5):451-6. https://dx.doi.org/10.1097/PCC.0000000000000714
6. Azab SF, Sherbiny HS, Salet SH, Elsaeed WF, Elshafiey MM, Siam AG, et al. Reducing ventilator-associated pneumonia in neonatal intensive care unit using “VAP prevention Bundle”: a cohort study. BMC Infectious Diseases. 2015;15(314):1-7. https://dx.doi.org/10.1186/s12879-015-1062-1
7. Deng C, Li X, Zou Y, Wang J, Namba F, Hiroyuki K, et al. Risk factors and pathogen prolife of ventilator-associated pneumonia in a neonatal intensive care unit in China. Clinical Journal of the Japan Pediatric Society. 2011;53(1):332-7. https://dx.doi.org/10.1111/j.1442-200X.2011.03382.x
8. Gutiérrez JM, Millare PA, Al Schengiti YA, Enaya AA. Exposure to reprocessed single-use tracheal suction catheter and ventilator-associated pneumonia risk: a preliminary, single unit-based, matched case-control study. J. Crit Care. 2016;32(1):154-61. https://dx.doi.org/10.1016/j.jcrc.2015.11.018
9. Peña-López Y, Pujol M, Campins M, Gonzáles-Antero A, Rodrigo JA, Balcells A, et al. Implementing a care bundle approach reduces ventilator-associated pneumonia and delays ventilator-associated tracheobronchitis in children: differences according to endotracheal of tracheostomy devices. Journal Infections Diseases. 2016;52(1):43-8. https://dx.doi.org/10.1016/j.ijid.2016.09.021
10. Bayona CEA, Gómez JHD, Gutierrez CAC. Factores de riesgo para neumonia associada al ventilador en um hospital de tecer nível de la cuidad de Medellin: estúdio de casos y controles. Medicina UBP. 2008;27(1):25-32.
11. Al Dorzi HM, El Saed A, Rishu AH, Balkhy HH, Memish ZA, Arabi YM. The results of a 6-year epidemiologic surveillance for ventilator-associated pneumonia at a tertiary care intensive care unit in Saudi Arabia. American Journal of Infection Control. 2012;40(1):794-9. https://dx.doi.org/10.1016/j.ajic.2011.10.004
12. Kusahara DM, Enz Cda C, Avelar AF, Peterlini MA, Pedreira Mda L. Risk factors for ventilator-associated pneumonia in infants and children: a cohort study. Am J Crit Care. 2014;23(6):469-76. https://dx.doi.org/10.4037/ajcc2014127
13. Nseir S, Di Pompeo C, Josefowicz E, Cavestri B, Brisson H, Nyunga M, et al. Relationship between tracheotomy and ventilator-associated pneumonia: a case–control study. Eur Respir J. 2007;30(1):314–20. https://dx.doi.org/10.1183/09031936.06.00024906
14. Gopal S, Luckraz H, Giri G, Nevill A, Muhammed I, Reid M, et al. Significant reduction in ventilator-associated pneumonia with the Venner-PneuX System in high-risk patients undergoing cardiac surgery: the low ventilator-associated-pneumonia study. Journal Cardiothorac. 2014;47(3):92-6. https://dx.doi.org/10.1093/ejcts/ezu483
15. Chao YF, Chen YY, Wang KW, Lee RP, Tsai H. Removal of oral secretion prior to position change can reduce the incidence of ventilator-associated pneumonia for adult ICU patients: a clinical controlled trial study. Journal Clinical Nursing. 2008; 18(1):22-8. https://dx.doi.org/10.1111/j.1365-2702.2007.02193.x
16. Quenot JPMD, Ladoire S, Dovoucoux F, Doise JM, Cailliod R, Cunin N, et al. Effect of a nurse-implemented sedation protocolo on the incidence of ventilator-associated pneumonia. Critical Care Medicine. 2007;35(9):2031-36. https://dx.doi.org/10.1097/01.ccm.0000282733.83089.4d
17. Hamishekar H, Shadvar K, Taghizadeh M, Golzadi SE, Mojtahedzadeh M, Soleimanpour H, et al. Ventilator-Associated Pneumonia in Patients Admitted to Intensive Care Units, Using Open or Closed Endotracheal Suctioning. Anesth Paim Med. 2014;4(5):1-6. https://dx.doi.org/10.5812/aapm.21649
18. Soares CB, Hoga LAK, Peduzzi M, Sangaleti C, Yonekura T, Silva DRAD. Revisão integrativa: conceitos e métodos utilizados na enfermagem. Rev Esc Enferm USP. 2014;48(2):335-45. http://dx.doi.org/10.1590/S0080-6234201400002000020
19. Moher D, Shamseer L, Clarke M, Ghersi D, Liberrati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Bio Med Central. 2015;4(1):1-9. https://dx.doi.org/10.1186/2046-4053-4-1
20. Kollef MH, Afessa B, Anzueto A, Veremakis C, Kerr KM, Margolis BD, et al. Silver-Coated Endotracheal Tubes and Incidence of Ventilator-Associated Pneumonia. American Medical Association. 2011;300(7):805-13. https://dx.doi.org/10.1001/jama.300.7.805
21. Tsai HH, Lin FC, Chang SC. Intermittent suction of oral secretions before each positional change may reduce ventilator-associated pneumonia: a pilot study. Am J Med Sci. 2008;336(5):397-401. https://dx.doi.org/10.1097/MAJ.0b013e31816b8761
22. European Centre for Disease Prevention and Control. Healthcare-associated infections acquired in intensive care units. Annual Epidemiological Report for 2015; 2015.
23. European Centre for Disease Prevention and Control. Surveillance of healthcare-associated infections and prevention indicators in European intensive care units. Stockholm: ECDC; 2017.
24. Morton PG, Fontaine DK, Hudak CM, Gallo BM. Cuidados Críticos de Enfermagem: uma abordagem holística. 12 ed. Rio de Janeiro: Guanabara Koogan, 2016.