Diving mask adapted for non-invasive ventilation and prone position in a patient with severe covid-19: case report
Máscara de mergulho adaptada para ventilação não-invasiva e posição prona em paciente com COVID-19 grave: relato de caso
Máscara de buceo adaptada para ventilación no invasiva y posición de prono en un paciente con covid-19 grave: reporte de caso
Diving mask adapted for non-invasive ventilation and prone position in a patient with severe covid-19: case report
Revista de Epidemiologia e Controle de Infecção, vol. 10, núm. 3, pp. 352-356, 2020
Universidade de Santa Cruz do Sul

Esta obra está bajo una Licencia Creative Commons Atribución 4.0 Internacional.
Recepción: 03 Julio 2020
Aprobación: 07 Octubre 2020
Abstract: Justification and objectives: In the search of strategies to treat acute respiratory failure caused by COVID-19, non-invasive ventilation (NIV) and the use of prone position in spontaneous breathing appear. The objective is to present the case of a patient with severe COVID-19 admitted to an intensive care unit (ICU) who used an adapted diving mask, which is configured as an innovative interface for NIV, and the prone position. Methods: Case report of a hospitalized patient diagnosed with COVID-19 who underwent early NIV by means of an adapted diving mask and the prone position during spontaneous breathing for 8 hours at night and 6 hours in the day. Results: Female patient, 56 years old, systemic arterial hypertension and obesity, with dry cough, odynophagia, fatigue and severe dyspnea on admission. Chest tomography with bilateral ground-glass opacities. Non-invasive ventilation was instituted 1-2.75 times/day, for 40-60 minutes, with positive pressure at the end of expiration of 8 (7.25-8.00) cmH.O and support pressure of 5.5 (4.00 -6.00) cmH.O. Air leaks of 6 to 30%, with good tolerance. The prone position during spontaneous breathing resulted in increased peripheral oxygen saturation and reduced respiratory discomfort 30 minutes later. Conclusion: The association of the use of NIV with an adapted diving mask and prone position during spontaneous breathing proved to be effective in preventing the orotracheal intubation of a patient with severe COVID-19, emphasizing the importance of the proposed intervention.
Keywords: Coronavirus, Respiratory failure, Non-invasive ventilation, Pronation.
Resumo: Justificativa e objetivos: Na busca de estratégias para o tratamento da insuficiência respiratória aguda causada pela COVID-19, surge a ventilação não invasiva (VNI) e o uso da posição prona em respiração espontânea. Objetiva-se apresentar o caso de uma paciente com COVID-19 grave admitida em unidade de terapia intensiva (UTI) e submetida à máscara de mergulho adaptada, que se configura em uma interface inovadora para VNI, bem como a posição prona. Métodos: Relato de caso de paciente hospitalizado diagnosticado com COVID-19 submetido à VNI precoce por meio da máscara de mergulho adaptada e uso da posição prona em respiração espontânea por 8 horas noturnas e 6 horas diurnas. Resultados: Paciente do sexo feminino, 56 anos, hipertensão arterial sistêmica e obesidade, apresentando tosse seca, odinofagia, fadiga e dispneia intensa na admissão. A tomografia de tórax demonstrou opacidades em vidro fosco bilaterais. A VNI foi instituída 1-2,75 vezes/dia, por 40-60 minutos, com pressão positiva ao final da expiração de 8 (7,25-8,00) cmH.O e pressão de suporte de 5,5 (4,00-6,00) cmH.O. Fuga aérea de 6 a 30%, com boa tolerância. A posição prona em respiração espontânea resultou em aumento da saturação periférica de oxigênio e redução do desconforto respiratório 30 minutos após. Conclusão: A associação do uso da VNI com máscara de mergulho adaptada e posição prona em respiração espontânea demonstrou ser eficaz em evitar a intubação orotraqueal de paciente com COVID-19 grave, ressaltando a importância da intervenção proposta.
Palavras-chave: Coronavírus, Insuficiência respiratória, Ventilação não invasiva, Pronação.
Resumen: Justificación y objetivos: En la búsqueda de estrategias para el tratamiento de la insuficiencia respiratoria aguda causada por COVID-19, aparecen la ventilación no invasiva (VNI) y el uso de la posición de prono con la respiración espontánea. El objetivo es presentar el caso de un paciente con COVID-19 grave ingresado en una unidad de cuidados intensivos (UCI) que utilizó una máscara de buceo adaptada, que se configura como una interfaz innovadora para VNI, así como la posición de prono. Métodos: Reporte de caso de una paciente hospitalizada con diagnóstico de COVID-19 que fue sometida a VNI precoz mediante máscara de buceo adaptada y la posición de prono con respiración espontánea durante 8 horas en la noche y 6 horas en el día. Resultados: Paciente de sexo femenino, 56 años, hipertensión arterial sistémica y obesidad, con tos seca, odinofagia, fatiga y disnea severa al ingreso. Tomografía de tórax con opacidades bilaterales en vidrio esmerilado. La VNI se instituyó de 1 a 2,75 veces/día, durante 40-60 minutos, con presión positiva al final de la espiración de 8 (7,25-8,00) cmH2O y presión de soporte de 5,5 (4, 00 -6,00) cmH2O. Fugas de aire del 6 al 30%, con buena tolerancia. La posición de prono con respiración espontánea resultó en un aumento de la saturación de oxígeno periférico y una reducción de las molestias respiratorias 30 minutos después. Conclusión: La asociación del uso de VNI con máscara de buceo adaptada y la posición de prono con respiración espontánea demostró ser efectiva para prevenir la intubación orotraqueal de una paciente con COVID-19 severo, enfatizando la importancia de la intervención propuesta.
Palabras clave: Coronavirus, Insuficiencia respiratoria, Ventilación no invasiva, Pronación.
INTRODUCTION
At the end of 2019, a viral infection by the infectious agent SARS-CoV-2 started and the disease was called COVID-191. Noninvasive ventilation (NIV) improves pulmonary ventilation in patients with COVID-192,3, provided that precautions are taken to minimize the risk of aerosolization4. Although the prone position has a strong foundation in the Severe Acute Respiratory Syndrome (SARS) for providing greater gas exchange5, a rigorous clinical monitoring is necessary to avoid delay in orotracheal intubation (OTI)6.
There are still no reports of studies on the effects of NIV with the adapted diving mask, because this is a new interface with research on its use under development. Such an interface is innovative, as it allows adequate sealing to the face, thereby minimizing the risk of aerosol generation in the environment. Aiming to contribute with evidence on such a therapeutic proposal, the objective is to present the case of a patient with severe COVID-19 admitted to an intensive care unit (ICU) who used NIV with an adapted diving mask and the prone position during spontaneous breathing. The study was approved by the Research Ethics Committee and the National Research Ethics Commission (CONEP) (CAAE 30783720.7.0000.5343) of the Universidade de Santa Cruz do Sul, Santa Cruz do Sul-RS, and informed consent was obtained.
CASE DESCRIPTION
Female patient, 56 years old, married, retired, incomplete primary school, living in a city in the countryside of Rio Grande do Sul – RS, with systemic arterial hypertension and obesity. She denied use of tobacco, alcohol and/or other drugs. Ten days after the onset of symptoms (dry cough, odynophagia and fatigue) with further worsening in the last four days and severe dyspnea, she was admitted to the Intensive Care Unit (ICU) on 23.04.20. The diagnosis of SARS-CoV-2 infection through the reverse transcription test followed by polymerase chain reaction (RT-PCR) had been confirmed in the city of origin on 20.04.20. Upon admission, she presented lymphopenia (953 cells/ul - 12.7%), reduced hematocrit (32%), increased C-reactive protein (CRP) (5.32 mg/dL), DHL (1185 u/L) and D-dimer (3326.29 ng/dL), with RPaO./FiO. of 100.2 mmHg (Table 1). Chest computed tomography (CT) revealed bilateral ground-glass opacities, peripheral and central, with consolidation and reticulation affecting more than 75% of the lung area (Figure 1).
| Hospital admission | Day 5 hospitalization | Day 14 hospitalization | Hospital discharge | |
| pH | 7.49 | 7.41 | 7.36 | 7.42 |
| PaO2, mmHg | 100.2 | 99.6 | 85.3 | 89.2 |
| PaCO2, mmHg | 36.8 | 46.3 | 52.7 | 40.6 |
| HCO3-, mEq/L | 27.8 | 29.1 | 29.5 | 25.9 |
| BE | +4.3 | +4.0 | +3.2 | +1.4 |
| SaO2, % | 98.0 | 97.7 | 94.7 | 96.8 |
| FiO2, % | 100 | 100 | 32 | 21 |
| PaO2/FiO2, mmHg | 100.2 | 99.6 | 266.5 | 424.7 |
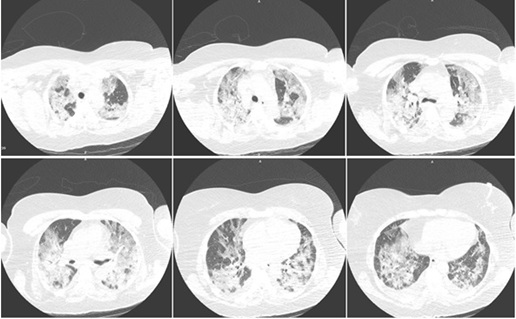
Figure 1
Computed tomography (CT) of a patient with COVID-19 at hospital admission.
Oseltamivir 75 mg, azithromycin 500 mg and ceftriaxone 1000 mg were started. Before hospitalization, the patient was using hydroxychloroquine, which was suspended on arrival at the institution. The use of full anticoagulation with unfractionated heparin-UFH (25000 UI FR/AMP 5 ml) intravenously started on 25.04.20, guided by the increase of D-Dimer levels by more than 100% in 36 hours and was maintained until reaching the target activated partial thromboplastin time (aPTT) (2-2.5 x the normal value), since hemostatic disorders have been related to SARS-CoV-2 infection7,8. On April 28, 2020 (day 6 of hospitalization), UFH was changed to enoxaparin (1mg/kg 2x/day).
Non-invasive ventilation was used by means of the adapted diving mask (Figure 2) in a mechanical ventilator, with a High-Efficiency Particulate Arrestance (HEPA) filter in the expiratory branch and a Heat and Moisture Exchanger (HME) filter in tracheal Y. It was instituted upon admission to the ICU and maintained until day 12 of hospitalization with the patient in the supine position, performed 2 (1-2.75) times/day for 60 (40-60) minutes, with PEEP levels of 8 (7.25-8.00) cmH.O and PSV of 5.5 (4.00-6.00) cmH.O. Adequate coupling was observed (air leaks of 6-30%), the patient presented good tolerance, reported dryness of the mouth/throat and slight pressure when fixing the mask to the face.
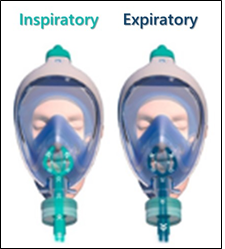
Figure 2
Air flow in the mechanical ventilation.
Image source: Onwtec Soluções em Engenharia e TecnoUnisc Company - Universidade de Santa Cruz do Sul.
The prone position during spontaneous breathing has been used in patients with hypoxemia due to COVID-19, as it improves oxygenation, reduces respiratory effort and can prevent OTI5,9,10. It was initiated on admission, with an increase in SpO2, a reduction in RR and respiratory discomfort 30 minutes later. Such therapy must be followed by strict monitoring of vital signs and the level of consciousness for adequate decision making on the need for OTI3. In view of the good response and hemodynamic stability, it was decided to use the prone position for 8 hours at night and 6 hours during the day with supplementation of oxygen therapy. After two days, as the patient reported cervical pain and difficulty sleeping, 500 mg dipyrone (if necessary), Precedex (100 mcg/ml vial/ampoule 2 ml) and massage therapy in the cervical and trapezoid areas were added.
From day 5 of hospitalization, the patient showed a favorable response to NIV and the prone position and improvement in dyspnea at rest with desaturation and tachypnea only during decubitus change. The time in prone position was gradually reduced (maintaining only 10 hours at night), as well as NIV time and oxygen supply (Figure 3), with progression in kinesiotherapy procedures and reestablishment of functionality. On 10.05.2020 (day 18 of hospitalization), the patient was discharged, breathing in ambient air with resolution of hypoxemia (Table 2).
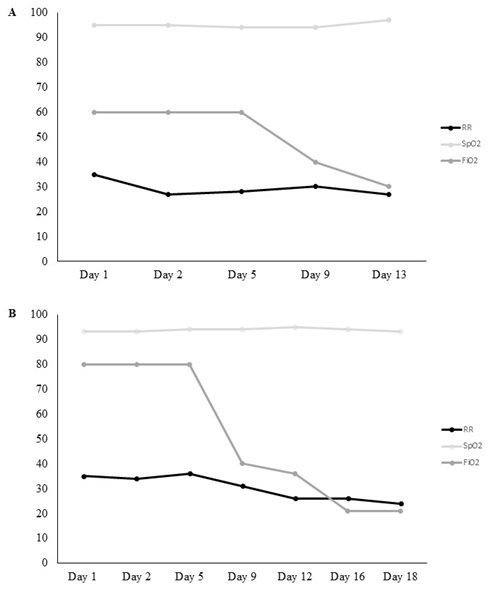
Figure 3
Behavior of respiratory rate (RR), peripheral oxygen saturation (SpO2) and fraction of inspired oxygen (FiO2) during the use of NIV in hospitalization (A) and during the prone position in hospitalization (B).
The present work is relevant because it is the first study involving a diving mask adapted as an interface for NIV. As a limitation, we emphasize that such findings cannot be generalized, given the need for a bigger sample size for a better foundation of the evidence found.
CONCLUSION
The association between the use of NIV and the prone position during spontaneous breathing proved to be effective in preventing the OTI of a patient with severe COVID-19, demonstrating the importance of the proposed intervention. Since this is a recent disease and its pathophysiological mechanisms have not yet been clarified, it is important to disclose treatments with positive outcomes that have been employed with accurate and constant monitoring.
References
1. Guan W-J. Ni ZY, Hu Y, Liang WH, Ou CQ, HE JX, et al. Clinical characteristics of coronavirus disease 2019 in China. N Eng J Med 2020;382:1708-1720. https://dx.doi.org/10.1056/NEJMoa2002032
2. Gattinoni CL, Chiumello D, Caironi P, Busana M, Romitti F, Brazzi L, et al. COVID-19 pneumonia: different respiratory treatment for different phenotypes? Intensive Care Med 2020. https://dx.doi.org/10.1007/s00134-020-06033-2
3. Peng M, Ren D, Liu XY, Li JX, Chen RL,, Yu BJ, et al. COVID-19 managed with early non-invasive ventilation and a bundle pharmacotherapy: A case report. World J Clin Cases 2020;8(9):1705–1712. https://dx.doi.org/10.12998 / wjcc.v8.i9.1705
4. American Society of Anesthesiologists. (ASA). COVID-19: Information for health care professionals, recommendations. 2020.
5. Lu SJ, Wang SP. Prone position and nursing care. Hu Li Za Zhi 2018;65(3):96-102. https://dx.doi.org/10.6224/JN.201806_65(3).13
6. Associação de Medicina Intensiva Brasileira. (AMIB). Orientações sobre o manuseio do paciente com pneumonia e insuficiência respiratória devido a infecção pelo coronavírus (SARS-CoV-2) - Versão n.05/2020*.
7. Connors JM, Levy JH. COVID-19 and its implications for thrombosis and anticoagulation. Blood 2020;135(23):2033–2040. https://dx.doi.org/10.1182/blood.2020006000
8. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 2020;395(10229):1054-1062. https://dx.doi.org/10.1016/S0140-6736(20)30566-3
9. Elharrar X, Trigui Y, Dols AM, et al. Use of prone positioning in nonintubated patients with COVID-19 and hypoxemic acute respiratory failure. JAMA 2020;323(22):2336-2338. https://dx.doi.org/10.1001/jama.2020.8255
10. Sun Q, Haibo QH, Huang M, Yang Y. Lower mortality of COVID-19 by early recognition and intervention: experience from Jiangsu Province. Ann Intensive Care 2020;33.