Abstract:
Population aging is associated with physiological changes and chronic diseases, such as COPD, which significantly impact quality of life (QoL). This study examines the relationship between respiratory symptoms and quality of life in rural patients, utilizing the St. George's Respiratory Questionnaire (SGRQ) and the modified British Medical Research Council (mMRC) dyspnoea scale. An observational and prospective study was conducted in 40 patients aged 40 to 90 years who were treated at the Claudio Benati Hospital in Zumbahua, Pujilí Town, Cotopaxi Province. Demographic variables, respiratory symptoms, and quality of life were assessed using SGRQ and mMRC. The sample was obtained by convenience sampling, excluding those who did not meet the established criteria. The sample included 65 % women and 35 % men, with a mean age of 63.6 years. The most prevalent respiratory symptoms were cough (100 %) and dyspnea (100 %). The SGRQ showed an average impairment of 72.5 %, with physical activity being the most compromised dimension (87.3 %). The mMRC indicated moderate to severe dyspnea, with 60 % of participants in grade 3. A significant relationship was found between exacerbations and quality of life (rho = 0.67, p < 0.001), but not between symptom frequency and individual dimensions. The results demonstrate a significant decline in the quality of life of patients with respiratory symptoms, underscoring the utility of tools such as the SGRQ and mMRC in assessing impact and guiding clinical interventions in vulnerable populations.
Keywords: Chronic Obstructive Pulmonary Disease, Quality Of Life, Dyspnea, Rural Population.
Resumen:
El envejecimiento poblacional está asociado a cambios fisiológicos y enfermedades crónicas, como la EPOC, que impactan significativamente en la calidad de vida (CV). Este estudio evalúa la relación entre síntomas respiratorios y calidad de vida en pacientes rurales, empleando el Cuestionario Respiratorio de St. George (CRSG) y la escala de disnea modificada del British Medical Research Council (mMRC). Se realizó un estudio observacional y prospectivo en 40 pacientes de 40 a 90 años atendidos en el Hospital Claudio Benati, de Zumbahua, cantón Pujilí, provincia de Cotopaxi. Se evaluaron variables demográficas, síntomas respiratorios y calidad de vida mediante CRSG y mMRC. La muestra se obtuvo por conveniencia, excluyendo a quienes no cumplían los criterios establecidos. La muestra incluyó 65 % mujeres y 35 % hombres, con media de edad de 63,6 años. Los síntomas respiratorios más prevalentes fueron tos (100 %) y disnea (100 %). El CRSG mostró una afectación promedio del 72,5 %, siendo la actividad física la dimensión más comprometida (87,3 %). La mMRC indicó disnea moderada a severa, con 60 % de participantes en grado 3. Se encontró una relación significativa entre exacerbaciones y calidad de vida (rho=0,67, p<0,001), pero no entre frecuencia de síntomas y dimensiones individuales. Los resultados evidencian una reducción considerable en la calidad de vida de pacientes con síntomas respiratorios, destacando la utilidad de herramientas como CRSG y mMRC para evaluar impacto y guiar intervenciones clínicas en poblaciones vulnerables.
Palabras clave: enfermedad pulmonar obstructiva crónica, calidad de vida, disnea, población rural.
Carátula del artículo
The quality of life of patients with respiratory symptoms
La calidad de vida de pacientes con síntomas respiratorios
 Jessica Paola Chancusig Palacios chancusigjessica4@gmail.com
Jessica Paola Chancusig Palacios chancusigjessica4@gmail.com
Claudio Benati Hospital, Ecuador
Lizbeth Alexandra García Tapia
Technical University of Ambato, Ecuador
Javier Caiza Lema
Technical University of Ambato, Ecuador
Revista Eugenio Espejo, vol. 19, núm. 3, pp. 17-35, 2025
Universidad Nacional de Chimborazo
Recepción: 30 Abril 2025
Aprobación: 01 Agosto 2025
INTRODUCTION
The older adult age group is a population experiencing exponential growth, undergoing multiple morphological, physiological, biochemical, and psychological changes that expose individuals to significant physical and mental limitations. (1,2)
According to the World Health Organization (WHO), 12.5 % of the total population is over 60 years old. This figure is expected to increase to 29.7 % by 2060. (3) The condition of being an older adult reveals a functional and structural deterioration due to physiological changes such as decreased protein synthesis, decreased bone density, alterations in the motor plate, and loss of brain mass, giving rise to scenarios of chronic pathologies. Within this concept are cardiopulmonary diseases that have socioeconomic significance due to the discriminated increase in cases and the care they require. (4,5)
The WHO(6) estimates indicate that approximately 30 % to 40 % of cases of chronic respiratory diseases are related to indoor air pollution, in addition to exposure to dust and working in polluted environments, (7,8) while acute cases are mainly associated with seasonal changes. (9) These figures increase in low- and middle-income countries, where primary health care systems often have difficulties in diagnosis, delaying care, especially for populations in areas with limited access, such as rural areas. (10)
All the changes that occur during the aging process have a significant impact on psychomotor skills, which in turn determine the quality of life. This concept relates to several value judgments that become self-attributable to the underlying pathology or condition itself and the limitations it produces. (11) The fact that it is associated with subjective components makes it difficult to find a metric to quantify it, tacitly evidencing the need to standardize tests, especially on older adults with a fragile condition.(12,13) Respiratory pathologies such as chronic obstructive pulmonary disease (COPD) are one of the conditions that most compromise quality of life. Recent epidemiological data, such as those collected in the 2023 Global Burden of Disease (GBD) study, show that COPD has a prevalence of 6 % in the global population and is also associated with a considerable deterioration in quality of life. (14,15)
Respiratory symptoms serve as an indicator or predictor of respiratory pathology, providing insight into its progression or worsening, and can also help identify limitations in daily living activities, exercise, and work performance. (16) In this way, information on respiratory symptoms should be considered of vital importance for epidemiological studies, especially in rural areas, to generate baselines that favor the development of a timely intervention. It should also be considered an important aspect in comprehensive care, (17) being essential the application of effective evaluation instruments or batteries that provide reliable and valid data on respiratory symptoms in different populations, such as those offered by the Saint George Questionnaire (CRSG), applied to the Latin American population, which has allowed to glimpse the real situation of chronic and acute respiratory pathologies. (18,19)
In Ecuador, although the St George test carried out by Rivadeneira has been validated since 2025 (20), scientific evidence on respiratory symptoms and their effect on the quality of life in people in rural areas is limited; studies such as that of Caini et al (2019) found that in Ecuador the highest influenza activity due to viral respiratory infections occurs in December and January. (21)
In Zumbahua, a rural parish of Pujilí, a highland area of Cotopaxi province, the majority of the inhabitants are registered as indigenous; most of them are engaged in agriculture. (22) These areas do not have all the basic services, so access to hospitals or health care centers is a real challenge. (23, 24)
Previous studies, such as those by Ibrahim et al.,( 25) have confirmed the pre-existing idea of the relationship between chronic respiratory symptoms and alterations in quality of life across the physical, psychological, and social spheres. Therefore, their early detection would improve the independence, autonomy, and well-being of patients who suffer from them. (26)
Under this premise, this study aimed to identify the quality of life of patients with respiratory symptoms living in rural areas who attend the Claudio Benati Hospital.
MATERIALS AND METHODS
This research was developed through an observational and prospective qualitative-quantitative approach carried out on 40 patients between 40 and 90 years old selected by non-probabilistic convenience sampling, all from the rural area of Zumbahua, who were part of the program for patients with respiratory pathology behaviors and were under biweekly follow-up at the Claudio Benati Hospital in Zumbahua, Pujilí canton, Cotopaxi province, in the period between 31 Oct 2023 to 6 Jan 2024. Patients with neurological disorders or mental health conditions that make communication impossible, with difficulty understanding and answering questions, patients outside the Zumbahua parish during the study, and those who did not agree to sign the informed consent were excluded.
The instrument used was the Saint George Questionnaire (SGRQ), specifically designed to evaluate the quality of life in patients with COPD, consisting of 50 questions organized on a 0 -5 point Likert scale. (27) According to the questionnaire, it has a cohort point where the higher the result, the worse the patient's quality of life is considered. This instrument demonstrates a Cronbach's α value of greater than 0.70 for all components. In addition, high sensitivity and specificity have been demonstrated under an ROC analysis, with a value of 0.92 (95 % IC 0.85 to 0.99) for COPD. Similarly, it exhibits high reliability, with a Cronbach's α of 0.92, which can be extrapolated to populations outside of COPD. (28, 29)
On the other hand, the modified dyspnea scale of the British Medical Research Council (mMRC) was also applied, which measures the severity of dyspnea in patients with COPD based on their perception of the disease, it consists of 5 items scored between 0 and 4. (30) Being an easy-to-apply scale makes it accessible and feasible to implement in COPD; a sensitivity ranging from 66 % to 81 %, specificity from 56 % to 70 % with a ROC curve between 0.62 to 0.76 has been shown. (31)
As regards this study, data on demographic variables such as age, sex (M/F), marital status (married/single/divorced/free union/widowed), weight (kg), height (cm), language (Spanish/Quichua), the location of the communities and addresses of each patient will be used;. In contrast, the analysis variables are respiratory symptoms, which are physical manifestations such as cough, phlegm, shortness of breath, chest noises. (27)
The intervention protocol was evaluated and authorized by the Research Ethics Committee of the University of the Americas (CEISH-UDLA), as well as authorization from the General Director of the Claudio Benatti Hospital in Zumbahua and the president of the Zumbahua Rural Parish GAD (Group of Rural Parishes), representing the rural population.
RESULTS
Of the total participants, 14 (35 %) were men and 26 (65 %) were women, with ages ranging from 42 to 90 years, with a mean of 63.63 (SD 14.208). According to the weight, the mean was 56.12 kg (SD 10.14), and the mean height was 1.5 m (SD 0.07). Regarding the marital status of the participants, 1 (2.5 %) was single, 34 (85 %) were married, and 5 (12.5 %) were widowed. Regarding the community to which the participants belong, 3 (7.5 %) were from Yanaturo, 6 (15 %) from Yanashpa, 7 (17.5 %) from Saraugsha, 11 (27.5 %) from Chami, 6 (15 %) from Michacala, and 7 (17.5 %) from Pucaugsha, as expressed in Table 1.
Table 1
Sociodemographic data
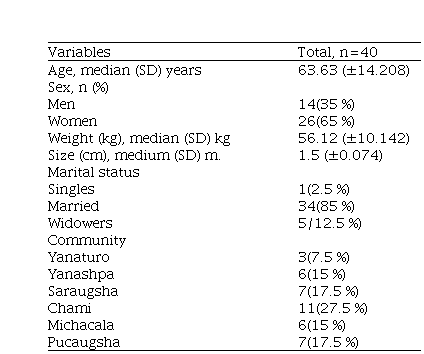
Note: (SD: standard deviation)
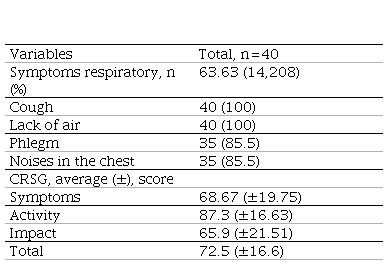
The weighting of the Saint George Respiratory Questionnaire (SGRQ) related to quality of life was scored according to the recommendations that propose a value of 0 to 100 for the total score of the questionnaire. (32) In addition, a reductionist numerical analysis that gives each sphere a total score (symptoms 566.2; activity 982.9; impact 1652.8) and the weighting obtained separately by dividing the sum of the weights by the maximum possible weighting for each component and expressing the result as a percentage. (33) Concerning the respiratory symptoms detected, they presented cough and shortness of breath, phlegm and noises in the respiratory cycle, obtaining an average level of 72.5 % (±16.6), these values demonstrate that in general there is a considerable affectation where the most affected sphere was physical activity with 87.3 % (±16.63) followed by symptoms with 68.67 % (±19.75) and 65.9 % (±21.51) in the impact expressed in table 2.
Table 2
Results of respiratory symptoms and SGRQ
Exacerbation of respiratory symptoms
Figure 1 shows the percentage of symptom exacerbation, measured using the modified Medical Research Council dyspnea scale (mMRC). 60 % of the sample presented a level 3, corresponding to a state where dyspnea requires stopping to rest after walking about 100 meters or after a few minutes of walking on flat ground; followed by 22.5 % with level 2, reflecting a sensation where dyspnea causes them to be unable to keep up with other people of the same age walking on flat ground or having to stop to rest when walking on flat ground at their own pace; and 17.5 % with level 4, corresponding to a sensation where dyspnea prevents the patient from leaving home or occurs with activities such as dressing or undressing. These data reveal a considerable impact on the well-being and normal functioning of the participants, which could have a significant effect on their quality of life.
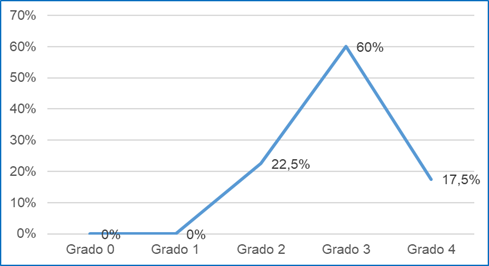 Figure 1
shows the percentage of symptom exacerbation, measured using the modified Medical Research Council dyspnea scale (mMRC). 60 % of the sample presented a level 3, corresponding to a state where dyspnea requires stopping to rest after walking about 100 meters or after a few minutes of walking on flat ground; followed by 22.5 % with level 2, reflecting a sensation where dyspnea causes them to be unable to keep up with other people of the same age walking on flat ground or having to stop to rest when walking on flat ground at their own pace; and 17.5 % with level 4, corresponding to a sensation where dyspnea prevents the patient from leaving home or occurs with activities such as dressing or undressing. These data reveal a considerable impact on the well-being and normal functioning of the participants, which could have a significant effect on their quality of life.
Figure 1
shows the percentage of symptom exacerbation, measured using the modified Medical Research Council dyspnea scale (mMRC). 60 % of the sample presented a level 3, corresponding to a state where dyspnea requires stopping to rest after walking about 100 meters or after a few minutes of walking on flat ground; followed by 22.5 % with level 2, reflecting a sensation where dyspnea causes them to be unable to keep up with other people of the same age walking on flat ground or having to stop to rest when walking on flat ground at their own pace; and 17.5 % with level 4, corresponding to a sensation where dyspnea prevents the patient from leaving home or occurs with activities such as dressing or undressing. These data reveal a considerable impact on the well-being and normal functioning of the participants, which could have a significant effect on their quality of life.
Figure 1. Level of exacerbation of respiratory symptoms, measured through the mMRC
Distribution of the sample of agreement to the frequency of the respiratory symptoms and the community
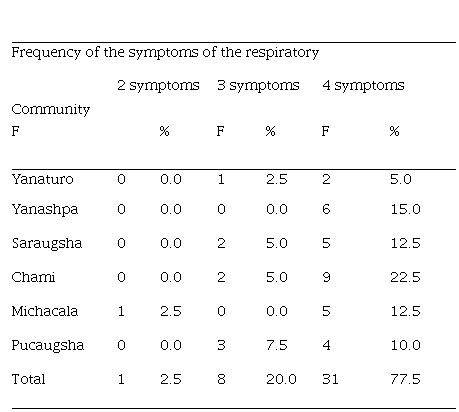
In Table 3, observe that most of the participants presented four respiratory symptoms, of which 9 (22.5 %) live in Chami, 6 (15.0 %) in Yanashpa, 5 (12.5 %) in Saraugsha and Michala, while 4 (10.0 %) live in Pucaugsha and 2 (5.0 %) in Yanaturo.
Table 3
Sample distribution, frequency of respiratory symptoms, and community
Correlation between variables
To assess the normal distribution of the data for each variable, the Shapiro-Wilk normality test was applied, given that the sample size was smaller than 50 participants. The impact variable (0.063) exhibited a normal distribution, whereas the remaining variables did not, as shown in Table 4. Therefore, a nonparametric test was required to measure the correlation between the variables.
Table 4
Data normality test
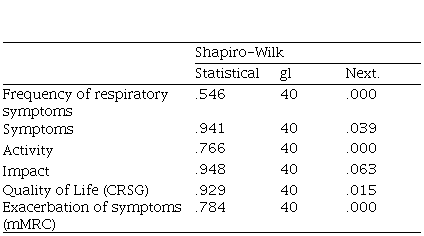
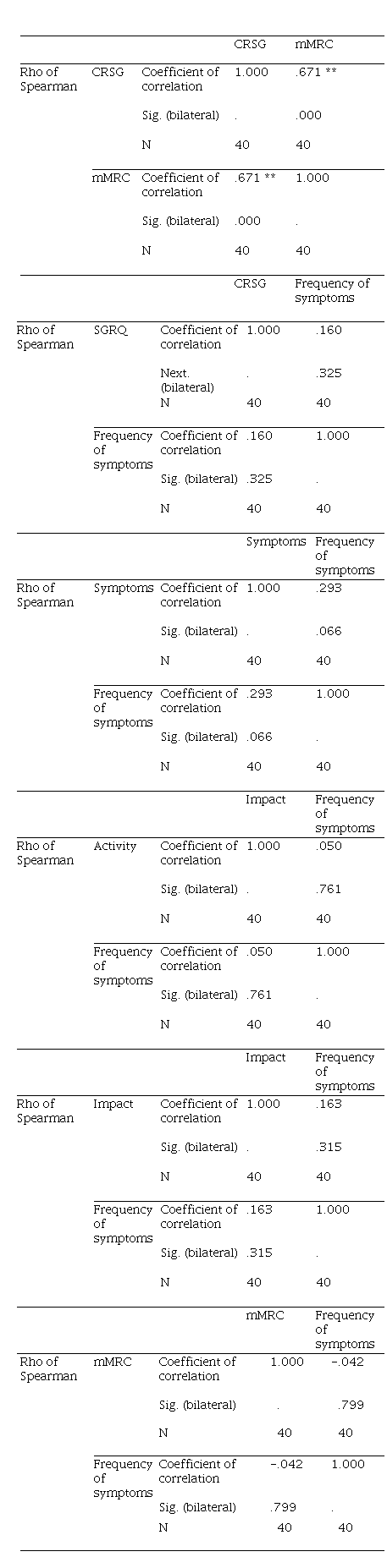
Table 5 presents the correlation between variables, indicating a p-value of 0.000 between quality of life (QoL) and symptom exacerbation (mMRC). This reflects a direct, moderate-to-high positive correlation, with a Spearman correlation coefficient of 0.67. The relationship between symptom frequency and overall QoL, as well as by dimension, showed a p-value of 0.325 for the total, 0.66 for symptoms, 0.761 for activity, and 0.315 for impact. The correlation between symptom frequency and mMRC also showed a p-value of 0.799. These data indicate a correlation only between quality of life and symptom exacerbation.
Table 5
Evidence of correlation between variables
DISCUSSION
This study, conducted among patients with respiratory symptoms from rural areas treated at the Claudio Benatti Hospital, collected information on the level of quality of life, measured using the SGRQ scale. The majority of participants were women (65 %) with an average age of 63.63; these data are similar to those reported by De la Torre et al., (34) who found that 18.2 % of 450 patients over 40 years of age presented chronic respiratory symptoms, affecting more people between 60 and 70 years of age, with a predominance in the female sex (59.8 %).
Regarding respiratory symptoms, a large proportion of older adults in this study experienced cough and shortness of breath, followed by phlegm production and chest noises, which may be associated with the combustion of materials such as firewood or charcoal for cooking in rural areas. (35,36) The high prevalence of cough in households where biomass fuel is used is consistent with the findings of Wafula et al. (37) When examining the frequency of respiratory symptoms among the participants by community. It was observed that the majority (77.5 %) presented with four symptoms, predominantly from the Chami and Yanashpa communities.
The analysis of quality of life utilized the SGRQ instrument, which has been reported to be more applicable for patients with COPD, offering the same clinical value as tools such as the COPD Assessment Test (CAT) (38) and the Chronic Respiratory Questionnaire (CRQ). (39) A point to highlight is the high reliability of the questionnaire to be related to functional limitations, obtaining scores between 0.7 and 0.8, which ranges from moderate to adequate. (40)
An average of 72.5 % of the affected area was obtained, which, according to the internationally proposed estimate, indicates a considerable decrease if 100 % is set as the base value for the maximum conditioning criterion of quality of life. (41) The most affected areas were activity (87.3 %), symptoms (68.67 %), and impact (65.9 %). These results show a population with high functional deterioration due to respiratory symptoms, coinciding with previous studies such as those of Lee et al., where 71.4 % of patients with COPD had mild airflow limitation measured by spirometry, of which 59.6 % had a high punctual, being presumptive for alteration of the quality of life. (42) It has been seen that the psychometric properties of the SGRQ mean that it is not for exclusive use in COPD, as mentioned in the systematic review by McLeese et al. where when applied to patients with bronchiectasis it presents a high reliability index, (43) an idea countered by Daudey et al. who mention the SGRQ as lacking a partial view of the impact of the disease, which restricts its capacity to guide therapeutic decisions comprehensively. (44)
The results obtained show a considerable reduction in the quality of life associated with the presence of respiratory symptoms, both acute and chronic, similar to the studies by Bolívar et al., (45) who reported an overall impact of 26.9 % in patients exposed to tobacco. In comparison, Rodríguez et al. (46) found an overall average of 52.1 % in symptoms, 79.3 % in activity, and 55.7 % in impact in patients with COPD.
Finally, regarding the exacerbation of respiratory symptoms, measured using the mMRC scale, dyspnea was found at levels between 2 and 4, with a higher proportion (60 %) at level 3, characterized by a feeling of shortness of breath that forces one to stop before walking 100 meters or after a few minutes on flat terrain. When considering symptom exacerbation by sex. It was observed that both women and men predominantly presented grade 3 dyspnea, with 40 % and 20 % respectively. Similarly, the correlation analysis between quality of life, as quantified by SGRQ, and symptom exacerbation, as measured by mMRC, showed a significant relationship (p = 0.000), with a Spearman's rho of 0.6, indicating a moderate to high correlation. However, no significant correlation was found between symptom frequency and the SGRQ, nor between symptom frequency and the mMRC, which could be due to the short recording period for symptom frequency. These data coincide with those shown by Phua et al., (47) where in patients with idiopathic pulmonary fibrosis, the mMRC had a consistent relationship with the quality of life (r=0.52), identifying the inexorable presence of worse psychological state, such as presenting depression and functional deterioration.
The limitations of this study relate to the type of design used, which only allows for describing the quality of life in patients with respiratory symptoms, without establishing a precise correlation between quality of life and the exacerbation of symptoms by individual sphere reported.
CONCLUSIONS
A significant relationship was found between quality of life and respiratory symptoms. This suggests that assessing quality of life in patients with respiratory symptoms could be a helpful tool for monitoring patients and anticipating potential complications in acute respiratory illnesses or exacerbations of chronic diseases. This assessment can contribute to a better understanding of patient needs, enabling comprehensive treatment and improved clinical outcomes. Despite existing limitations, the data obtained can serve as a basis for future randomized studies and the development of preventive strategies for managing chronic respiratory diseases. Detailed recording of respiratory symptom exacerbations is also suggested in patients requiring long-term monitoring.
Conflict of interest: The authors declare that they have no conflict of interest.
Contribution statement: All authors contributed to the conception, preparation, and development of the manuscript.
Información adicional
redalyc-journal-id: 5728

