Paget's bone disease, clinical case report
Enfermedad Ósea de Paget, reporte de caso clínico
 Connie Daniela Kroll Chica connie_daniela@hotmail.com
Donna Estefanía Rodríguez Lara
Asdruval Ramiro Granda Cueva
Eduardo Harry Herrera Méndez
Connie Daniela Kroll Chica connie_daniela@hotmail.com
Donna Estefanía Rodríguez Lara
Asdruval Ramiro Granda Cueva
Eduardo Harry Herrera Méndez
Paget's bone disease, clinical case report
Revista Eugenio Espejo, vol. 19, núm. 3, pp. 92-103, 2025
Universidad Nacional de Chimborazo

Esta obra está bajo una Licencia Creative Commons Atribución-NoComercial-SinDerivar 4.0 Internacional.
Recepción: 18 Noviembre 2024
Aprobación: 03 Julio 2025
Abstract:
Paget's disease is a disorder affecting bone metabolism due to accelerated bone remodeling. It mainly affects the pelvis, spine, lower extremity bones, and skull. It is believed to be the result of a combination of genetic and environmental factors; its incidence has decreased in recent years. Symptoms are usually absent; however, some report bone pain. Treatment aimed to prevent bone remodeling by using bisphosphonates. We present the case of a 34-year-old female with pain and bone deformity of the knee of 5 months of evolution, in radiographs and scintigraphy, with signs compatible with Paget's disease. Bisphosphonates were administered, and there was improvement after 3 months. This is a relevant case because the incidence of Paget's disease is higher in men over 40 years of age.
Keywords: Osteitis Deformans, Bone Remodeling, Bisphosphonates.
Resumen:
La enfermedad de Paget es un trastorno que afecta al metabolismo óseo dado por una remodelación ósea acelerada. Afecta principalmente a la pelvis, columna, huesos de extremidades inferiores y cráneo. Se cree que es el resultado de la combinación de factores genéticos y ambientales, su incidencia ha disminuido en los últimos años. Generalmente no se presentan síntomas; sin embargo, algunos refieren dolor óseo. El objetivo de tratamiento es evitar la remodelación ósea con el uso de bifosfonatos. Se presenta caso de femenina de 34 años con dolor y deformidad ósea de rodilla de 5 meses de evolución, en radiografías y gammagrafía con signos compatibles con enfermedad de Paget. Se administra bifosfonatos con mejoría de cuadro a los 3 meses. Este es un caso relevante debido a que la incidencia de la enfermedad de Paget es mayor en hombres sobre los 40 años.
Palabras clave: osteítis deformante, remodelación ósea, bifosfonatos.
INTRODUCTION
Paget's disease of bone (PDB), also known as osteitis deformans, was first described by Sir James Paget in 1876 (1) and is a disorder affecting bone metabolism. It is characterized by accelerated bone remodeling, resulting in excessive bone growth in specific areas, either in a single location (monostotic PDB) or in multiple locations (polyostotic PDB). It can lead to deterioration in the integrity of the affected bones. The most commonly affected body parts are the pelvis in up to 70 % of cases, the femur in 30–55%, the lumbar spine in 25–50 %, the skull in 20–4 %, and the tibia in 15–30 %. (2,3)
The incidence is low in South American countries, and those primarily affected are of European origin. Over the past 20 years, the prevalence has decreased considerably in many countries. (1) Despite advances in technology and research, there are no studies that report the incidence of PDB in Ecuador.
Most patients with PDB are asymptomatic. In these cases, the diagnosis is usually made incidentally, often after a routine blood test reveals elevated levels of bone-derived alkaline phosphatase, an isoenzyme found in the plasma membrane of osteoblasts, whose serum concentration provides an index of osteoblastic activity, (4) or through imaging studies performed for other reasons, which show characteristic changes in bone of the disease. (5)
Paget's disease manifests primarily through two main clinical symptoms: pain caused by direct damage to the bone, complications arising from excess bone growth such as osteoarthritis or nerve compression, and deafness (due to alterations in the bony structures that contain the inner ear). Fractures, bone tumors, neurological disorders, and imbalances in calcium and phosphate levels may also occur. Furthermore, due to the increased vascularization of the bone affected by Paget's disease, there may be an increased risk of bleeding during orthopedic surgical procedures. (2, 5)
The pathogenesis of the disease is thought to result from a combination of genetic and environmental factors. Although genetic mutations contribute to susceptibility, the declining prevalence in certain areas also suggests the influence of environmental factors. A consistent correlation between PDB and various environmental exposures, such as measles exposure, pet ownership, urban or rural environment, heavy metal exposure, milk intake, or family size, has not yet been established. (6) However, environmental triggers have been identified, including toxins, low calcium intake, vitamin D deficiency, biomechanical loading, and infections with slow viruses such as paramyxoviruses (e.g., measles virus). (7) (Studies in mice show that overexpression of slow viruses induces a state of elevated bone turnover.) (8)
In 1883, it was observed that PDB could occur in several members of a family, with 15 % of cases reporting this family history (1)
A significant amount of evidence has been collected supporting the influence of genetic factors in the development of the disease; familial inheritance appears to follow an autosomal dominant pattern with variable penetrance. Alonso et al. (8) have, through genome-wide association studies, proposed the identification of 15 genetic loci involved in the onset of PDB, most of which are related to proteins known to affect bone physiology. Some of these loci directly affect the activity of the RANK-RANKL pathway, such as the TNFRSF11A locus encoding RANK.
In a review by Ralston et al., it was shown that the most prominent and best-documented genetic association is with mutations of the ubiquitin-associated (UBA) domain of SQSTM1, which encodes the ubiquitin-binding protein sequestosome-1. A specific mutation, SQTSM1 P392L, has been identified in several families with familial PDB, and this mutation is the most common, present in up to 50 % of familial PDB cases; in addition, 28 other different mutations in SQSTM1 are associated with PDB, with a significant percentage of association with sporadic PDB cases, both in germline and somatic mutations. (9)
The presence of SQSTM1 mutations, especially truncating mutations, has been shown to correlate with a more severe clinical phenotype of the disease. However, it is essential to note that some adults with inherited SQSTM1 mutations from an affected parent exhibit disease symptoms in only a minority of cases, suggesting the potential influence of gene-environment interactions on disease expression. (10)
For the diagnosis of PDB, radiographs should be performed to demonstrate the degree of deformity, identify possible fractures, and also evaluate adjacent joints that could be affected. Among the radiographic characteristics of PDB, we can observe osteolytic areas, cortical thickening, loss of distinction between the cortex and medulla, trabecular thickening, osteosclerosis, and bone deformity (Figure 5A, 5B). (2) Computed tomography and magnetic resonance imaging are primarily functional when a preoperative requirement for arthropathy or corrective osteotomy is necessary; (7) a biopsy is rarely required to establish the diagnosis of PDB. (11)
Nuclear bone scintigraphy is the most sensitive test for identifying pagetic lesions. (7) Regarding laboratory tests, several markers of elevated bone turnover can be used; among these, serum alkaline phosphatase (AP) is the most commonly used. (12)
In patients with active PDB who present symptoms, treatment with bisphosphonates is indicated to reduce bone resorption by osteoclasts through pharmacological means. Bisphosphonates are classified into nitrogen-containing bisphosphonates such as clodronate, etidronate, and tiludronate, and those containing nitrogen such as pamidronate, alendronate, zolendronic acid, and risedronate. (13) The functionality of the bisphosphonate family is determined by the affinity for hydroxyapatite and the inhibition of farnesyl pyrophosphate. By influencing this mechanism, secondary apoptosis of osteoclasts is induced. (7)
Bisphosphonates are the primary treatment for PDB; however, complications of the disease may require surgical procedures such as joint replacement, osteotomy for deformity, or surgical therapy for associated pathological fractures. (7) The adverse effects of bisphosphonate use are related to excessive suppression of bone remodeling, including atypical fractures and osteonecrosis of the jaw, mainly at the maxillomandibular level and as a secondary location it is usually associated with the hip; (14) however, Silvestre et al. have shown that necrosis is time-dose dependent, so maxillary osteonecrosis usually appears between 4 months and 6 years after starting treatment with bisphosphonates. (15)
CASE PRESENTATION
Female patient, 39 years old, mestiza, married, resident of the city of Quito, occupation: seamstress, Catholic. Personal pathological history: apparently poliomyelitis in childhood, family pathological history: not reported, surgical history: not reported, Gynecological-Obstetric history: menarche: 7 years, date of last menstruation: 10 days before admission, family planning: barrier method, pregnancies: 2, births: 2, cesarean: 0
The patient presents with pain in his left knee, which began five months ago and lasted seven days, with no apparent cause, and was moderately intense. The visual analogue scale (VAS) was 6/10. A valgus-type bone deformity and limited walking accompanied her. She self-medicated with paracetamol and ibuprofen at unspecified doses on several occasions without improvement.
On physical examination: left lower limb: left hip: flexion 90 degrees, extension 0 degrees, external rotation 20 degrees, internal rotation 30 degrees, left knee: valgus deformity is evident, at 9 degrees, extension 0 degrees, pain on palpation on the anteromedial side of the left leg (Figure 1A, 1B, 1C)
Table 1. Diagnostic evaluation
Laboratory studies:
| Reference ranges | 12/13/2023 | 08/03/2024 | |
| Total serum calcium (milligrams per deciliter) | 8.5 - 10 | 8.84 | |
| Serum phosphorus (milligrams per deciliter) | 2.5 - 4.5 | 2.35 | |
| Parathormone (picograms milliliter) | 10 -55 | 43.90 | |
| Thyroid-stimulating hormone (microunits milliliters) | 0.4 - 4 | 0.487 | |
| Antithyroglobulin (international units milliliter) | LESS THAN 116 | 10,000 | |
| Free thyroxine (nanograms per deciliter) | 0.92 – 1.68 | 1.17 | |
| 24-hour urine calcium (milligrams) | LESS THAN 300 | 38.4 | |
| C-reactive protein | 0 - 5 | 8.35 | |
| Erythrocyte Sedimentation Rate (Millimeters per hour) | UNDER 20 | 45 | |
| Alkaline phosphatase (International Units) | 40 - 129 | 682 | 270 |
| Uric acid (milligrams deciliter) | 3.5 – 7.2 | 6.8 | 4 |
Imaging studies :

Figure 1A, 1B, 1C: Left leg with evidence of valgus deformity

Figure 2. Hip and AP radiograph of bilateral femur: an inveterate fracture is evident at the level of the left femoral neck in addition to bilateral coxa vara.

Figure 3. Lateral radiograph of the left femur: poor bone quality, very thin cortices, ground-glass images, areas of osteolysis and osteosclerosis in the greater and lesser trochanters and the neck of the femur, loss of distinction between the cortex and the bone marrow of the upper part of the femur.

Figure 4. Lateral radiograph of the left knee and leg: evidence of valgus deformity

Figure 5. 5a AP radiograph of bilateral legs, 5b Anteroposterior and lateral radiograph of left ankle: tibia and fibula with increased bone density, bone with irregular and thin cortices, valgus deformity of tibia and fibula are observed.
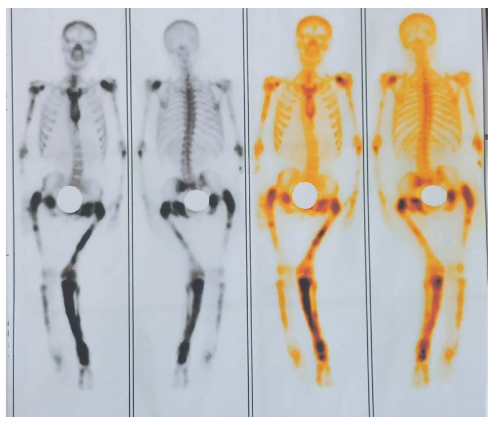
Figure 6. Bone scan: marked increase in osteoblastic activity with bone deformity in the humerus, femur, tibia, which appears to correspond to the scintigraphic pattern of Paget's disease as a first consideration.
Therapeutic intervention: Alendronate 40 milligrams orally daily, due to the unavailability of intravenous medication. Additionally, calcium carbonate 500 milligrams daily and vitamin D 5 drops daily are prescribed. The patient is discharged to continue treatment with bisphosphonates and undergo periodic check-ups. At her last consultation (3 months after starting treatment), the patient does not report pain and remains asymptomatic, in control tests with considerable evidence of a decrease in AP.
DISCUSSION:
Osteitis deformans, also known as Paget's disease of bone, as previously mentioned, is a condition whose incidence has been declining in recent years. It is essential to suspect it in patients with bone pain and deformity without a specific cause. It is the second most common bone remodeling disease after osteoporosis and can occur in any bone. (16) The patient in this case presented with polyostotic involvement (pelvis and lower limbs), asymmetrically.
This disease typically occurs in middle-aged and elderly patients, with an increased onset after 50 years of age and a rare diagnosis before 40 years of age. (17) Additionally, a higher incidence has been observed in men (1.4:1). (2) However, in our case, it is a 34-year-old female patient with an apparent history of poliomyelitis.
Regarding clinical presentation, approximately 70 % of PDB cases are usually asymptomatic and diagnosed incidentally based on radiological findings or elevated AP levels, (18) however, bone pain is the most common symptom evidenced in up to 73 % of symptomatic cases according to a 2014 study by Tan A. et al. (19) although the mechanisms of pain are not fully understood, an increase in metabolic activity is mentioned that could be related to the onset of pain. (7) Reid et al. (1996) showed that 41.8 % of people with elevated total AP did not experience bone pain. However, in the PRISM study, a randomized trial of intensive versus symptomatic treatment, it was found that 635 patients had increased AP at baseline, of which only 295 suffered from bone pain. Wang Qin-Yi et al., in their 2020 study of 256 cases of Paget's disease, 226 patients (88.3 %) were symptomatic, in 113 of 126 patients elevated AP levels were obtained; however, when applying the chi-square test (p = 0.288) they showed that there is no statistically significant correlation between the AP level and bone pain, (12) when comparing the presented case, bone pain was identified, in addition to elevated AP as in most cases. Regarding other symptoms, bone metaplasia may occur, which leads to hearing loss, obstructive hydrocephalus, deformities and paraplegia; in the same study by Tan A. et al., (19) the presence of bone deformity in 21.5 %, deafness in 8.9 % and pathological fractures in 8.5 % is mentioned, symptoms that were not present in the case in question.
For diagnosis, Wang Qin-Yi et al. (12) in their study, reported that 40.7 % were diagnosed with PDB by performing x-rays and determining AP levels; x-ray in 134 cases (77.9 %), AP levels in 108 cases (62.8 %), biopsy 70 cases (4.07 %), bone scan in 44 cases (25.6 %), tomography in 43 cases (25 %) and magnetic resonance imaging in 13 cases (7.6 %); in the presented case, PDB is determined based on the clinical finding, radiographic complements and serum AP levels; in addition to evidence of the suggestive conclusions in the bone scan.
Treatment is based on symptom control and the prevention of deformity. Drugs such as analgesics, nonsteroidal anti-inflammatory drugs, or antineuropathic agents are often used. Bisphosphonates remain the primary treatment for reducing bone turnover, demonstrating their effects on lowering total serum AP. Therefore, their determination is used as a measure of treatment efficacy.
In a study by Merlotti et al., (20) involving 90 patients, the administration of a single dose of 4 mg of zolendronic acid versus 30 mg of intravenous pamidronate for two consecutive days every 3 months was compared, determining that both generated pain improvement and a decrease of up to 75 % in AP levels, with zolendronic acid being more effective. Another study by Reid et al. determined that a single dose of 5 mg of intravenous zoledronic acid generated a greater probability of pain relief compared to a single two-month course of risedronate sodium 30 mg administered orally daily. (2) Alendronate is structurally similar to pamidronate. In a later study also conducted by Ralston et al., (13) the effects of oral alendronate at a dose of 40 mg were compared with those of placebo for 2 months, followed by a 6-month follow-up in patients with active PDB. The study observed a significant reduction in uric acid and AP after 3 months. Still, in the placebo group, no significant changes were observed in these markers, which, in comparison with the case presented, can help clarify the relationship between the use of daily oral alendronate and the decrease in AP and uric acid, which in turn led to an improvement in pain.
In patients with the development of bone deformity, pharmacological management does not reverse this complication. Therefore, surgical procedures such as hip replacement, total knee replacement, femoral and tibial osteotomy, correction of spiral stenosis or nerve compression, vertebropalsy, and ventriculoperitoneal shunt (in cases of hydrocephalus) may be considered. (1)
Regarding the adverse effects of bisphosphonates, especially intravenous ones, they can cause pathological fractures, including atypical femoral fractures, uveitis, osteonecrosis of the jaw, hypocalcemia, and impaired renal function. Most of the studies supporting these effects involve the use of oral bisphosphonates that do not contain nitrogen. Zoledronic acid, despite its evident efficacy, was found to have the highest risk of adverse effects. When receiving treatment with bisphosphonates, patients should ensure adequate dietary calcium intake and vitamin D supplementation, which is believed to reduce the rate of adverse effects.
CONCLUSIONS
The case presented here identifies clinical, imaging, and laboratory findings consistent with Paget's disease, and a comparison with previous studies confirms this conclusion. The diagnosis is based on radiographs and determination of AP levels. Treatment aims at symptom control and preventing progressive deformity, and is therefore based on the administration of bisphosphonates in combination with analgesics, nonsteroidal anti-inflammatory drugs, or antineuropathic agents.
Source of Funding: Funding for this article was provided through our means.
Acknowledgments: The authors would like to thank the patient for her willingness and support in carrying out this case.
Conflicts of interest: The authors declare that they have no conflicts of interest.
Contribution statement: Dona Estefanía Rodríguez Lara contributed to the information gathering. Connie Daniela Kroll Chica wrote the article. Asdruval Ramiro Granda Cueva participated in the discussion, while Eduardo Harry Herrera Méndez was responsible for the final draft of the article.
REFERENCES BIBLIOGRAFICS
1. Singer FR. The evaluation and treatment of Paget's disease of bone. Best Pract Res Clin Rheumatol. 2020; [cited Jun 15, 2024]; 101506. Available at: https://www.sciencedirect.com/science/article/abs/pii/S1521694220300231 DOI: https://doi.org/10.1016/j.berh.2020.101506.
2. Ralston SH, Corral-Gudino L, Cooper C, et al. Diagnosis and management of Paget's disease of bone in adults: a clinical guideline. J Bone Miner Res. 2019; [cited 1 Jun 2024]; 34(4):579–604. Available from: https://academic.oup.com/jbmr/article/34/4/579/7606010 DOI: https://doi.org/10.1002/jbmr.3657
3. Rendina D, et al. Diagnosis and treatment of Paget's disease of bone: position paper from the Italian Society of Osteoporosis, Mineral Metabolism and Skeletal Diseases (SIOMMMS). J Endocrinol Invest . 2024; [cited 3 Jun 2024]; 47(6):1335–60. Available from: https://link.springer.com/content/pdf/10.1007/s40618-024-02318-1.pdf. DOI: https://doi.org/10.1007/s40618-024-02318-1.PMID:38488978.
4. Pariente A. Alkaline phosphatase. EMC - Tratado de Medicina. 2024; [cited 25 Jun 2024]; 28(3):1–5. Available from: https://www.sciencedirect.com/science/article/abs/pii/S1636541024492994 DOI: https://doi.org/10.1016/S1636-5410(24)49299-4.
5. Singer FR, Bone HG III, Hosking DJ, Lyles KW, Murad MH, Reid IR, Siris ES. Paget's disease of bone: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab . 2014; [cited 2 Jun 2024]; 99(12):4408–22. Available from: https://academic.oup.com/jcem/article/99/12/4408/2833929 DOI: https://doi.org/10.1210/jc.2014-2910.
6. Menéndez-Bueyes LR, Soler Fernández MC. Paget's disease of bone: an approach to its historical origins. Reumatol Clin. 2017; [cited 6 Jun 2024]; 13(2):66–72. Available from: https://www.sciencedirect.com/science/article/abs/pii/S2173574317300011.
7. Choi YJ, Sohn YB, Chung YS. Updates on Paget's disease of bone. Endocrinol Metab (Seoul). 2022; [cited 24 Jun 2024]; 37(5):732–43. Available from: https://synapse.koreamed.org/articles/1516079575 DOI: https://doi.org/10.3803/EnM.2022.1575.PMID:36327984;PMCID:PMC9633214.
8. Alonso N, Calero-Paniagua I, del Pino-Montes J. Clinical and genetic advances in Paget's disease of bone: a review. Rev Osteoporos Metab Miner. 2017; [cited 8 Jun 2024]; 15(1):37–48. Available from: https://www.pure.ed.ac.uk/ws/portalfiles/portal/30397360/art_10.1007_s12018_016_9226_0.pdf . DOI: https://doi.org/10.1007/s12018-016-9226-0 .
9. Ralston SH, Layfield R. Pathogenesis of Paget disease of bone. Calcif Tissue Int. 2012; [cited 13 Jun 2024]; 91(2):97–113. Available from: https://www.researchgate.net/profile/Stuart-Ralston/publication/224867639_Pathogenesis_of_Paget_Disease_of_Bone/links/5761cd3808aeeada5bc501bd/Pathogenesis-of-Paget-Disease-of-Bone.pdf . DOI: https://doi.org/10.1007/s00223-012-9599-0 .
10. Chung PYJ, Beyens G, Boonen S, Papapoulos S, Geusens P, Karperien M, et al. Most of the genetic risk for Paget's disease of bone is explained by genetic variants near the CSF1, OPTN, TM7SF4, and TNFRSF11A genes. Hum Genet. 2010; [cited 11 Jun 2024]; 128(6):615–26. Available from: https://ris.utwente.nl/ws/portalfiles/portal/6834764/Chung10majority.pdf . DOI: https://doi.org/10.1007/s00439-010-0888-2 .
11. Maatallah K, Ben Nessib D, Labbène E, Ferjani H, Bouaziz M, Kaffel D, et al. Paget's disease of bone in patients under 40 years: two case reports and review of the literature. Sultan Qaboos Univ Med J. 2021; [cited 12 Jun 2024]; 21(1):e127–31. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC7968898/pdf/squmj2102-e127-131.pdf . DOI: https://doi.org/10.18295/squmj.2021.21.01.019.
12. Wang QY, Fu SJ, Ding N, Liu SY, Chen R, Wen ZX, et al. Clinical features, diagnosis and treatment of Paget's disease of bone in mainland China: a systematic review. Rev Endocr Metab Disord. 2020; [cited 7 Jun 2024]; 21(4):645–55. Available from: https://link.springer.com/article/10.1007/s11154-020-09544-x . DOI: https://doi.org/10.1007/s11154-020-09544-x.
13. Ralston SH, Layfield R. Pathogenesis of Paget disease of bone. Calcif Tissue Int. 2012; [cited 13 Jun 2024]; 91(2):97–113. Available from: https://www.researchgate.net/profile/Stuart-Ralston/publication/224867639_Pathogenesis_of_Paget_Disease_of_Bone/links/5761cd3808aeeada5bc501bd/Pathogenesis-of-Paget-Disease-of-Bone.pdf . DOI: https://doi.org/10.1007/s00223-012-9599-0 .
14. Rodriguez J. Drug-induced osteonecrosis: benefit/risk profile of bisphosphonate use [online thesis]. Valladolid: University of Valladolid; 2021. Available from: https://uvadoc.uva.es/handle/10324/1757.
15. Escobar López EA, López López J, Marques Soares MS, Chimenos Küstner E. Bisphosphonate-associated osteonecrosis of the jaw: a systematic review. Odontoestomatol. 2007; [cited 14 Jun 2024]; 23(2). Available from: https://scielo.isciii.es/pdf/odonto/v23n2/original4.pdf.
16. Corral Gudiño L. Paget's disease of bone: 1877–2023. Etiology and approach to a disease in epidemiological transition. Med Clin (Barc). 2023; [cited 16 Jun 2024]; 161(5):207–16. Available from: https://www.sciencedirect.com/science/article/pii/S0025775323002592 DOI: https://doi.org/10.1016/j.medcli.2023.05.005.
17. Rianon NJ, Bordes JK. Paget disease of bone for primary care. A.M APm Physician. 2020; [cited 19 June 2024]; 102(4):224–8. Available from: https://www.aafp.org/pubs/afp/issues/2020/0815/p224.pdf.
18. Lee JK, Kang YK, Wang PW, Hong SM. Paget's disease of bone affecting peripheral limb: difficulties in diagnosis: a case report. J Bone Metab . 2020; [cited 20 Jun 2024]; 27:71–5. Available from: https://ubmed.ncbi.nlm.nih.gov/32190611/
19. Tan A, Ralston SH. Clinical presentation of Paget's disease: evaluation of a contemporary cohort and systematic review. Calcif Tissue Int . 2014; [cited 23 Jun 2024]; 95:385–92. Available from: https://www.proquest.com/docview/1609058381?pq-origsite=gscholar&fromopenview=true&sourcetype=Scholarly%20Journals.
20. D. Merlotti, L. Gennari, G. Martini, F. Valleggi , V. De Paola, A. Avanzati , R. Nuti, Comparison of different intravenous bisphosphonate regimens for Paget 's disease of bone, J. Bone Miner. Res. [cited 3 Jun 2024]; 22 (10) (2007) 1510 – 1511. Available at: https://onlinelibrary.wiley.com/doi/pdfdirect/10.1359/jbmr.070704.
Información adicional
redalyc-journal-id: 5728