Carátula del artículo
Article / Clinical Case Report
Pleomorphic hyalinizing angiectatic tumor of the mesorectum: a rare case and review of literature
 Vigneshwaran Balasubiramaniyan
Vigneshwaran Balasubiramaniyan
All India Institute of Medical Sciences, India
Dillip Muduly
All India Institute of Medical Sciences, India
Swagatika Samal
All India Institute of Medical Sciences, India
Madhabananda Kar
All India Institute of Medical Sciences, India
Mahesh Sultania
All India Institute of Medical Sciences, India
Susama Patra
All India Institute of Medical Sciences, India
Prasanta Kumar Das
All India Institute of Medical Sciences, India
Autopsy and Case Reports, vol. 9, no. 3, e2019097, 2019
São Paulo, SP: Universidade de São Paulo, Hospital Universitário
Received: 04 April 2019
Accepted: 25 May 2019
CASE REPORT
A 30-year-old female presented complaining of dysmenorrhea for 1 year. She had normal bladder and bowel habits. A pelvic examination revealed an extra-rectal mass on the right para-rectal space, pushing the uterus towards the left side. The rectal mucosa was normal. Contrast-enhanced computed tomography of the abdomen and pelvis showed the presence of a well-defined mass with heterogenous contrast-enhancement in the left presacral area abutting the left lateral wall of the rectum (
Figure 1).
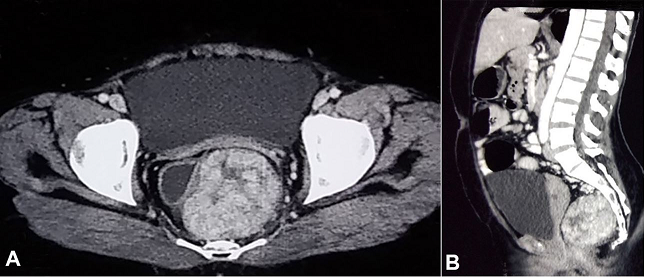 Figure 1
A and
B – Pelvic computed tomography after contrast medium injection revealing heterogeneously enhancing mass in the pelvis abutting the lateral wall of rectum with clear fat planes with uterus.
Figure 1
A and
B – Pelvic computed tomography after contrast medium injection revealing heterogeneously enhancing mass in the pelvis abutting the lateral wall of rectum with clear fat planes with uterus.
A guided core needle biopsy confirmed PHAT. An exploratory laparotomy was performed, followed by a wide excision of the mass, and hysterectomy and bilateral salpingo-oophorectomy. At the 12-month follow-up the patient was well with no evidence of relapsed disease.
On gross examination, a globular and capsulated mass measuring 7.5 × 6 × 4.5 cm was identified. The cut surface was solid with small cystic spaces and large areas of hemorrhage without any necrosis or calcification (
Figure 2).
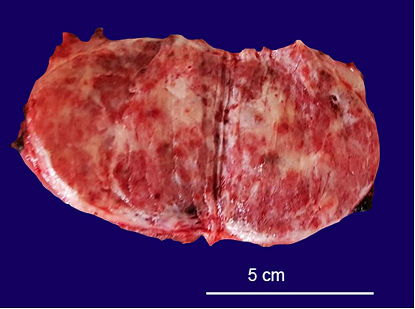 Figure 2
Gross examination of the tumor revealing a globular encapsulated mass measuring 7.6 × 4.5 cm. The cut surface shows predominantly a solid mass with small cystic spaces and areas of hemorrhage.
Figure 2
Gross examination of the tumor revealing a globular encapsulated mass measuring 7.6 × 4.5 cm. The cut surface shows predominantly a solid mass with small cystic spaces and areas of hemorrhage.
Microscopic examination revealed the presence of a well-encapsulated tumor composed of numerous ecstatic vascular channels with fibrin deposition, myxoid change, and hyaline degeneration. (
Figure 3) On immunohistochemistry, the stromal cells were diffusely positive for CD34, but negative for S100, smooth muscle actin, and MDM2 (
Figure 4A,
4B). The MIB1 labeling index was approximately 1%–2% in the highest proliferating areas. (
Figure 4C) Perl Prussian blue staining demonstrated iron deposits in the lesion (
Figure 4D). With these findings, the final diagnosis of PHAT was made.
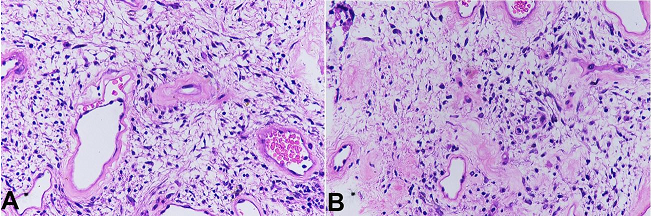 Figure 3
Photomicrographs of the tumor.
A – Ectatic hyalinized vessels and intervening spindle shaped stromal cells (H&E, 40X).
B – Infiltration of mixed inflammatory cells into the stroma (H&E, 40X).
Figure 3
Photomicrographs of the tumor.
A – Ectatic hyalinized vessels and intervening spindle shaped stromal cells (H&E, 40X).
B – Infiltration of mixed inflammatory cells into the stroma (H&E, 40X).
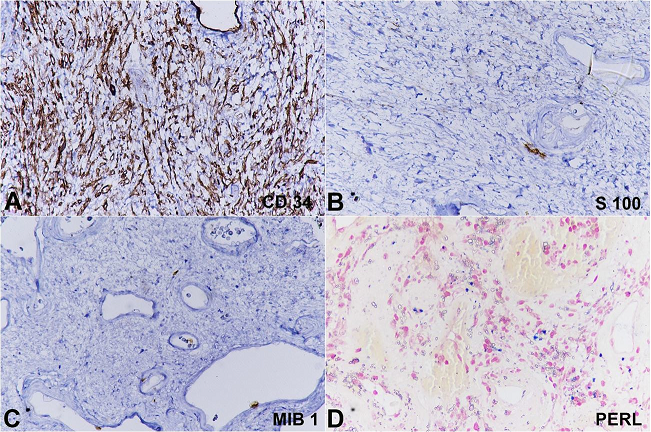 Figure 4
Photomicrographs of the tumor showing the stromal cells diffusely and strongly positive for CD34 (
A), while negative for S100 (
B).
C – The MIB1with 1%-2% of positivity.
D – Perl Prussian blue staining demonstrates intracytoplasmic and extra cellular iron deposition.
Figure 4
Photomicrographs of the tumor showing the stromal cells diffusely and strongly positive for CD34 (
A), while negative for S100 (
B).
C – The MIB1with 1%-2% of positivity.
D – Perl Prussian blue staining demonstrates intracytoplasmic and extra cellular iron deposition.
DISCUSSION
Pleomorphic hyalinizing angiectatic tumor (PHAT) is a rare spindle cell neoplasm with an uncertain cell of origin. PHAT has a predilection for involving subcutaneous tissues, most commonly those of the extremities. However, there are case reports describing PHAT arising from buccal mucosa, perineum, scrotum, and renal hilum.
1,2 To date, this is the third PHAT to be described in the pelvic region.
PHAT has been classified as a benign tumor with uncertain tissue of differentiation according to the latest WHO classification of soft tissue tumors.
3 Since its first description, approximately 120 cases of PHAT have been described in the English literature.
4 The largest series, to date, was described by Folpe and Weiss
5 and included 41 cases. The median age of onset is 53 years, ranging from 10 to 83 years. There is a female to male preponderance (4:3) with subcutaneous tissue the most common area, and the lower extremity the most common location. Other less frequently affected sites include the trunk, upper extremities, axilla, inguinal region, perineum, buttock, back, oral cavity, and scrotum.
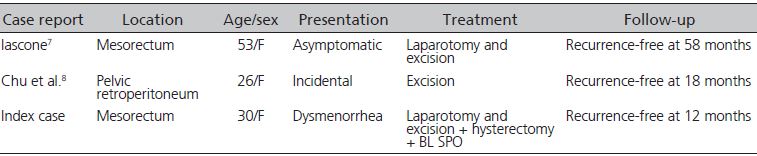
6 Various studies have shown local recurrence rates of 30%-50% on long-term follow-up. However, no metastases have been documented. Previously, only two cases of PHAT arising from the pelvic cavity have been described (
Table 1).
Table 1
Case reports of pelvic PHAT
The most striking feature of this tumor is the hyalinizing angioectatic vasculature. Smith et al.
9 had proposed two theories regarding the formation of hyalinized vessels. The first mechanism suggests that tissue injury caused by tumor infiltration may lead to the release of vasoactive mast cell products with subsequent increased vascular permeability within the tumor. The second mechanism postulates that the encroachment of the advancing tumor on normal vessels may cause endothelial damage and exudation of plasma contents with subsequent organization, leading to the formation of perivascular hyaline deposits. Folpe and Weiss
5 proposed that the vascular changes occur very early even without significant spindle cell proliferation. Further, the characteristic pleomorphism of classic PHAT is a late, time-dependent, degenerative phenomenon.
Studies have shown that PHAT tumor cells consistently express vimentin, CD34, and vascular endothelial growth factor.
10 Less frequently, CD99 and Factor XIIIa are expressed. The tumor cells were consistently negative for CD68, actin, desmin, and S100. Differentiation from Schwannoma is based on S100 negativity. Immunostaining for vimentin, CD34, and CD99 has failed to suggest a clear cell of origin. In the present case, on immunostaining the tumor cells were diffusely positive for CD34 and negative for S100, SMA, and MDM2.
Our imaging finding of a well-defined mass with heterogeneous contrast enhancement and many surrounding dilated vessels is similar to other published reports
8,11 (
Figure 1). This may be considered as a common imaging feature of PHAT. The presence of high-density areas on non-contrast computed tomography (CT), which did not show any enhancement, was probably due to hemorrhage within the lesion, and was confirmed by the histopathologic study.
Chu et al.
12 reported the magnetic resonance imaging features as a well-defined mass showing isointense and slight hypointense on T1-weighted images, and isointense and hyperintense on T2 weighted images. Contrast enhanced images showed heterogenous enhancement with large vessels showing flow void sign. Positron emission tomography-CT revealed a well-defined mass with no FDG uptake correlating with the low mitotic rate.
Though PHAT has a low mitotic rate and an absence of documented metastases, aggressive recurrences can lead to significant morbidity. Therefore, it is considered to be a borderline (intermediate grade) soft tissue sarcoma rather than a benign one. A high recurrence rate of 30%–50% has been documented with the majority of cases being marginally resected.
10 Folpe and Weiss
5 described a case of PHAT recurring as a case of myxoid pleomorphic sarcoma 4 years later in the same location.
Currently, the standard treatment for extremity PHAT is wide local excision with a tumor-free margin. In pelvic PHAT, a tumor-free margin can be considered adequate. Due to the small number of cases, there is no robust evidence of the role of adjuvant therapy in PHAT. Adjuvant radiotherapy has been used in various case series to decrease the local recurrence rate, but further evidence is required before advocating its use.
8 Chemotherapy has no role in view of the absence of any distant metastases.
