Article / Autopsy Case Report
Idiopathic Lipoid Pneumonia: An incidental finding in autopsy specimen
 Shreya Sadhu
Shreya Sadhu
Idiopathic Lipoid Pneumonia: An incidental finding in autopsy specimen
Autopsy and Case Reports, vol. 10, no. 1, 2020
São Paulo, SP: Universidade de São Paulo, Hospital Universitário
Received: 04 October 2019
Accepted: 23 December 2019
DOI: 10.4322/acr.2020.143
ABSTRACT: Lipoid pneumonia is a rare form of pneumonia which was initially described to be caused by inhalation or aspiration of fatty substances. Certain autopsy studies have reported the incidence to be 1.0-2.5%. Based on the mode of lipid acquisition, it has been classified into endogenous, exogenous or idiopathic types. Almost 50% of the patients with lipoid pneumonia are asymptomatic, and may be discovered by chance during routine chest imaging. In symptomatic patients, the symptoms are non- specific. However, it can produce inflammatory pneumonitis that can progress to irreversible pulmonary fibrosis as seen in our case. We present a case of a 53-year-old deceased male. A piece of one of his lungs was received after autopsy, which appeared normal grossly. There was no history of any illness before death. Microscopy revealed interstitial fibrosis with collection of foamy macrophages in alveolar spaces and cholesterol crystals surrounded by inflammatory reaction including occasional giant cells. The clinical picture and radiologic changes in cases of lipoid pneumonia can mimic bacterial pneumonia and tuberculosis. The occupational history is of extreme importance and should always be investigated.
Keywords: Pneumonia, macrophages, Lipids.
INTRODUCTION
Lipoid pneumonia, also called cholesterol pneumonia, is a rare form of pneumonia which was initially described to be caused by inhalation or aspiration of fatty substances. This entity was first described in the initial half of the twentieth century by Laughlen GF1 in one adult, one infant and two children after repeated inhalation of nasopharyngeal oil droplets . Since then, many cases of lipoid pneumonia have been reported occurring in all age groups, and in association with various other medications, substances, exposures and diseases. Although data on the precise incidence of lipoid pneumonia in the general population are lacking, certain autopsy studies have reported the incidence to be 1.0-2.5%.2
Based on the mode of lipid acquisition, it has been classified into endogenous, exogenous, or idiopathic types. The exogenous type is commoner and associated with the use of mineral oil for the treatment of constipation, whereas the endogenous type is usually secondary to bronchial obstruction or associated with pulmonary fat embolism, alveolar proteinosis, and lipid deposit diseases. The idiopathic form, also rare, has been described in smokers.3
Herein, we present the case of a 53-year-old deceased male whose heart and a piece of one of the lungs was received after post-mortem for histopathological examination in our department.
CASE REPORT
After the performance of the autopsy by a medical officer in the General Hospital, a piece of one of the lungs of a 53-year-old deceased male was received along with whole heart fixed in 10% formalin, in our department for histopathological examination. Post-mortem papers revealed no significant history of illness before death, since the person was unknown/unclaimed. The cause of death on autopsy seemed natural. The lung specimen weighed 10g and measured 5 x 2.5 x 1 cm, which external as well as cut surface, as seen on serial sectioning was unremarkable. There were no signs of airway obstruction
Hematoxylin and eosin stained microsections from this lung piece were examined under the light microscope and revealed congestion, interstitial lymphoplasmacytic infiltrate, interstitial fibrosis with a collection of foamy macrophages in alveolar spaces and cholesterol crystals surrounded by inflammatory reaction including occasional giant cells in almost all fields (Figure 1). These were surrounded by areas of fibrosis at few places that varied in intensity and completeness in these sites, thus fibrosis being the consequence rather than the cause of the process. Surrounding normal lung parenchyma could also be made out staining for mycobacteria and fungi were negative.
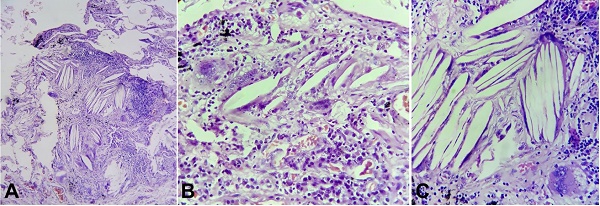
Figure 1
Photomicrographs of sections from the lung. A – Cholesterol clefts along with chronic interstitial inflammation (H&E, 100X); B – Cholesterol clefts along with numerous foamy lipid laden macrophages and dense lymphoplasmacytic infiltrate (H&E, 400X); C – a multinucleated giant cell with cholesterol clefts; an early manifestation in the development of cholesterol granulomas (H&E,400X).
A diagnosis of idiopathic lipoid pneumonia was made. Staining for fat using Sudan IV was attempted. However, sections could not be cut due to formalin-fixed specimen being received for histopathology.
The heart weighed 340g (reference range 248-431 g) and appeared normal on gross examination. Representative microsections did not show any significant pathological change, and also the coronary arteries were unremarkable.
DISCUSSION
Lipoid pneumonia is an unusual cause of pneumonia. It has been reported in various age groups and different clinical settings. Apart from case reports of lipoid pneumonia in children treated with mineral oil-based nasal drops for common cold and in adults with oily laxative abuse, some other reported risk factors include nasopharyngeal anatomic defects or neuromuscular weakness predisposing to aspiration, extremes of age, recurrent loss of consciousness, occupational exposure in fire eaters4 and forceful feeding of animal fat in children with a view to regularize bowel habits.3,5
Exogenous lipoid pneumonia has also been described with the use of petroleum jelly, milk, poppy seed oil, and egg yolk. It has also been reported in patients with prolonged facial application of petrolatum for erythrodermic psoriasis. Some reports have also shown association with excessive use of lip balm and flavored lip gloss.6-8
The endogenous type is comparatively less common and usually occurs secondary to bronchial obstruction or in association with pulmonary fat embolism, alveolar proteinosis, and lipid deposit diseases such as alveolar phospholipoproteinosis, Niemann-Pick disease, Wegener granulomatosis and undifferentiated connective tissue diseases. The idiopathic form has been described in healthy smokers.3
The pathophysiology of lipoid pneumonia is not clearly understood. Lipids float on the surface of gastric fluids. Hence, these oil-based medications may enter the airway due to regurgitation and aspiration. These aspirated particles of oil are usually bland and non-irritating, and do not stimulate a cough reflex. Therefore, these particles easily reach the lower respiratory airways facilitating aspiration even in the absence of risk factors. Once in the airways, these particles inhibit the mucociliary clearance and thus, their expulsion is further impaired. Deposited lipids cannot be metabolized due to lack of enzymes in humans, but are rather emulsified and engulfed by the alveolar macrophages in which they can remain for a long time. Following disruption of macrophages, these are released into the alveoli in a timely fashion. A giant cell reaction is then elicited, which further leads to fibrosis and disruption of alveoli and bronchus.3,9,10
Almost 50% of the patients of lipoid pneumonia are asymptomatic and may be discovered by chance during routine chest imaging. In symptomatic patients also, the symptoms are nonspecific (chest pain, cough or dyspnea) and vary according to the duration of exposure, and amount of oil aspirated.8
Exogenous lipoid pneumonia can present in acute and chronic forms, the former being described in elderly and children being treated for constipation and the latter occurring as a consequence of continuous aspiration of various materials in the work environment. The chronic form is comparatively less common. Guarachi et al.11 reported a case of chronic exogenous lipoid pneumonia in a patient who was a gas station attendant and siphoned excess gasoline (petroleum derivative like mineral oil).
Apart from the clinical history, the presence of distinct histologic characteristics also helps in differentiation between the exogenous and endogenous forms. These include the detection of extracellular lipid material, the appearance of intracytoplasmic vacuoles (cholesterol clefts) in alveolar macrophages (as seen in our case), the distribution of macrophages in the lung tissue, and the physicochemical characteristics of the oil.12 It is also characterized by giant cell granulomatous reaction (hence also called lipid granulomatosis), chronic inflammation and alveolar and interstitial fibrosis.13
The different characteristics of oils can be detected according to histochemical reactions: on Sudan IV and oil red O staining, mineral oils (in case of exogenous lipoid pneumonia) show a positive reaction as a yellow or orange color while in the endogenous variety a positive staining is seen as red color.12
Radiologic findings can also aid in diagnosis; however, these too are nonspecific, varying from perihilar opacity to extensive areas of consolidations with air bronchogram.2,13 These features are seen mainly in the lower and posterior lobes of lungs. Hence, the appearance may mimic that of lobar pneumonia. Thus, it is justified to include lipoid pneumonia in the differential diagnosis of chronic, delayed or repeated pneumonia.14
In our case, the patient died of a natural cause, and features of lipoid pneumonia were seen on histopathology of the lung. History of any such exposures or diseases that could lead to the endogenous variety of lipoid pneumonia could not be ruled out. However, the post-mortem chart did not specify any illness prior to death. Lipid laden macrophages may remain dormant for a long duration and release the lipid into the alveoli when they lyse, thus inciting an inflammatory reaction. This is the likely mechanism for a patient being asymptomatic as in our case. Staining for fat using Sudan IV was attempted. Any past chest radiographs/ CT scans of the deceased also could not be traced. We hereby report this case due to its non-specific findings and very low incidence.
CONCLUSION
Lipoid pneumonia in healthy adults is an unusual condition, and its diagnosis can be delayed since the clinical picture and radiologic changes can mimic bacterial pneumonia and tuberculosis. The occupational history is of extreme importance and should always be investigated. The case we described belonged to the idiopathic lipoid pneumonia category. It can produce inflammatory pneumonitis that can progress to irreversible pulmonary fibrosis, as seen in our case. It is therefore required that this entity be kept in mind while examining the histopathology microsections of autopsy cases to avoid misdiagnosis.
REFERENCES
Laughlen GF. Studies on pneumonia following nasopharyngeal injections of oil. Am J Pathol. 1925;1(4):407-14. PMid:19969662.
Baron SE, Haramati LB, Rivera VT. Radiological and clinical findings in acute and chronic exogenous lipoid pneumonia. J Thorac Imaging. 2003;18(4):217-24. http://dx.doi.org/10.1097/00005382-200310000-00002. PMid:14561906.
Madan K, Walia R, Kumar J, Jain D, Guleria R, Venkatnarayan K. Diesel siphoner’s lung: exogenous lipoid pneumonia following hydrocarbon aspiration. Lung India. 2014;31(1):63-6. http://dx.doi.org/10.4103/0970-2113.125986. PMid:24669087.
Kitchen JM, O’Brien DE, McLaughlin AM. Perils of fire eating. An acute form of lipoid pneumonia or fire eater’s lung. Thorax 2008;63(5):401-439.
Annobil SH, Morad NA, Khurana P, Kameswaran M, Ogunbiyi O, al-Malki T. Reaction of human lungs to aspirated animal fat (ghee): A clinicopathological study. Virchows Arch. 1995;426(3):301-5. http://dx.doi.org/10.1007/BF00191368. PMid:7773510.
Hadda V, Khilnani GC, Bhalla AS, Mathur S. Lipoid pneumonia presenting as non resolving community acquired pneumonia: A case report. Cases J. 2009;2(1):9332. http://dx.doi.org/10.1186/1757-1626-2-9332. PMid:20062592.
Betancourt SL, Martinez-Jimenez S, Rossi SE, Truong MT, Carrillo J, Erasmus JJ. Lipoid pneumonia: spectrum of clinical and radiologic manifestations. AJR Am J Roentgenol. 2010;194(1):103-9. http://dx.doi.org/10.2214/AJR.09.3040. PMid:20028911.
Becton DL, Lowe JE, Falletta JM. Lipoid pneumonia in an adolescent girl secondary to use of lip gloss. J Pediatr. 1984;105(3):421-3. http://dx.doi.org/10.1016/S0022-3476(84)80017-7. PMid:6590825.
Graef I. Pulmonary changes due to aspirations of lipids and mineral oil. Am J Pathol. 1935;11:862-3.
Rahaghi F, Varasteh A, Memarpour R, Tashtoush B. Teppanyaki/Hibachi Pneumonitis: An exotic cause of exogenous lipoid pneumonia. Case Rep Pulmonol. 2016;2016:1-12. http://dx.doi.org/10.1155/2016/1035601. PMid:27965910.
Guarachi GIY, Moreira VB, Ferreira AS, Sias SMA, Rodrigues CC, Teixeira C. Case Rep Pulmonol. 2014;1-4. http://dx.doi.org/10.1155/2014/358761.
Sias SMA, Daltro PA, Marchiori E, et al. Clinic and radiological improvement of lipoid pneumonia with multiple bronchoalveolar lavages. Pediatr Pulmonol. 2009;44(4):309-15. http://dx.doi.org/10.1002/ppul.20918. PMid:19283836.
Laurent F, Philippe JC, Vergier B, et al. Exogenous lipoid pneumonia: HRCT,MR, and pathologic findings. Eur Radiol. 1999;9(6):1190-6. http://dx.doi.org/10.1007/s003300050815. PMid:10415259.
Marchiori E, Zanetti G, Escuissato DL, et al. Pneumonia lipo’ıdica em adultos: aspectos na tomografia de alta resoluc. Radiol Bras. 2007;40:315-9. http://dx.doi.org/10.1590/S0100-39842007000500007.
Notes
Author notes
Correspondence Shreya Sadhu Junior Resident - Department of Pathology Pt. B.D. Sharma PGIMS, Rohtak – India Phone: +91 9599310328shreyasadhu328@gmail.com
Conflict of interest declaration