ABSTRACT:
Phosphorus is a nonmetallic irritant used in various sectors like rodenticide, firecracker industries, match industries, and fertilizers. Phosphorus poisoning is responsible for deaths among children and adults. Accidental yellow phosphorus poisoning is frequently reported in children, whereas suicidal consumption is not uncommon amongst adults. Herein, we present the case of a 30-year-old female patient who ingested Ratol paste containing yellow phosphorus in an attempt to commit suicide. Her initial chief complaints were nausea, vomiting along with loose motion during hospitalization, followed by a symptomless phase with stable vitals on the 2nd day, and managed conservatively. She took discharge against the medical advice. Later on, she was readmitted in the same hospital, after two days, complaining of generalized weakness, bodily pain, drowsiness, loss of appetite, and breathing difficulties. She developed severe complications due to the intoxication and died. An autopsy was performed. The histopathological and the toxicological examination were carried out. We found characteristic features in different organs due to yellow phosphorus toxicity. We concluded the cause of death as hepatic encephalopathy and multi-organ dysfunction syndrome caused by the yellow phosphorus poisoning.
Keywords:PhosphorusPhosphorus,Hepatic encephalopathyHepatic encephalopathy,Multiple organ failureMultiple organ failure.
Carátula del artículo
Article / Autopsy Case Report
A fatal case of multi-organ failure in acute yellow phosphorus poisoning
 Jai Prakash Soni
Jai Prakash Soni
Gajra Raja Medical College, India
Pankaj Suresh Ghormade
All India Institute of Medical Sciences, India
Swapnil Akhade
All India Institute of Medical Sciences, India
Krishnadutt Chavali
All India Institute of Medical Sciences, India
Bedanta Sarma
All India Institute of Medical Sciences, India
Autopsy and Case Reports, vol. 10, no. 1, 2020
São Paulo, SP: Universidade de São Paulo, Hospital Universitário
Received: 16 October 2019
Accepted: 06 January 2020
INTRODUCTION
In India, around 70% of rural households still depend primarily on agriculture for their livelihood.1 The unchecked growth of rodents like rats around the household and sometimes in farms and fields can be problematic because of the potential disease spreading undoing the food supply and consequent economic loss. Hence, rodenticides are widely marketed in India, and various preparations are available, such as the yellow phosphorus in the form of Ratol paste and powder. This preparation is cheap and easily available in the open market and online e-commerce sites in India, which contribute to the frequently reported cases of suicides due to Ratol ingestion. Accidental consumption of Ratol paste at home is not uncommon amongst children. Rodenticides containing 3-5% yellow phosphorus are currently available, and Ratol paste contains 3%.2 It is highly toxic and does not have any antidote. Accidental poisoning is very common by Ratol paste since it is very similar to toothpaste.3-5 Yellow phosphorus is also used in fireworks and matches, which leads to chronic poisoning in workers.6 Yellow phosphorus is a kind of non-metallic protoplasmic poison. It is rapidly absorbed from the digestive tract and is primarily metabolized by the liver.7 The smallest fatal dose is 8 mg, but the usual fatal dose is 1 mg/kg.8 Vomitus after phosphorus ingestion is luminescent and has a characteristic garlic odor. If the patient survives the initial gastrointestinal irritation phase, hepatic toxicity ensues secondary to a systemic poisoning. Herein, we report a fatal case of suicidal yellow phosphorus poisoning.
CASE REPORT
A 30-years-old female patient was admitted to the Department of Trauma & Emergency Medicine of a tertiary care hospital complaining of burning sensation in mouth, nausea, and vomiting. The garlicky odor exhaled from the vomitus. Her husband provided the information of 10-12g Ratol paste ingestion about 2 hours before. Gastric lavage was done with 1:5000 KMnO4 along with activated charcoal. She was conscious with a blood pressure of 140/80 mmHg, pulse rate of 84 beats per minute, and respiratory rate of 20 per minute. Results of different tests at the time of admission are shown in Table 1.
Table 1
Results of Laboratory investigations
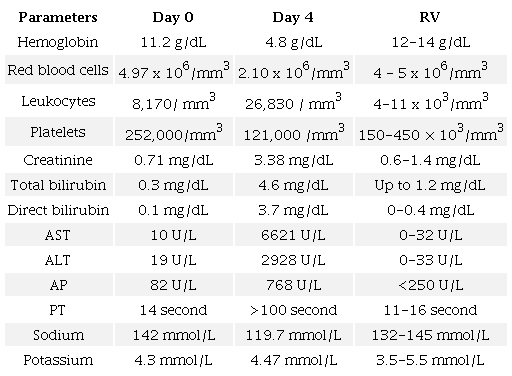
Bedside ultrasonography (USG) of the abdomen was unremarkable. Symptomatic management was done along with N-acetylcysteine (NAC). On the 2nd day, her clinical status improved, and she was asymptomatic. The patient and their relative took discharge despite insistent medical advice to remain hospitalized. On the 4th day, the patient returned to the hospital with generalized weakness, bodily pain, drowsiness, and breathing difficulty. She was drowsy with hypotension (blood pressure of 88/58 mmHg), tachycardia (110 bpm), and tachypnea.
On general examination, icterus was present. Laboratory workups on the 4th day are shown in Table 1. A bedside abdominal USG showed hepatomegaly and fatty changes. Hence, a provisional diagnosis of yellow phosphorus poisoning with hepatic encephalopathy and multiorgan failure was made. On the 5th day, the patient develops sudden onset of bradycardia, hypotension, and rapidly led to the patient’s death, with no possibilities to perform liver transplantation. An autopsy was conducted.
AUTOPSY FINDINGS
On postmortem examination, scleral icterus was present. Both pleural cavities were filled with hemorrhagic fluid, approximately 350 ml each. Interlobular fissures of both lungs showed petechial hemorrhages. The weight of both lungs was 410g and 455g for right and left one respectively (RV; 450g and 375 g respectively). On the cut section, the lungs were congested. Pinpoint hemorrhage was present over the heart surface. The weight of the heart was about 270g (RV; 243 g). The peritoneal cavity was filled with 750 ml of a hemorrhagic effusion. The stomach mucosa was hemorrhagic. Pinpoint to pinhead size petechial hemorrhages were present over the mesenteries, liver, and kidneys (Figure 11B). Yellowish discoloration of the liver, kidneys, and brain surfaces was present. Weight of liver was about 1100g (RV; 1100 g); for right and left kidneys, it was 114g and 129g, respectively (RV; for both 288 g); and for the brain, it was 1177g (RV; 1233 g). The cut section of the liver (Figure 1C) and kidneys (Figure 1D) showed pinpoint hemorrhage.
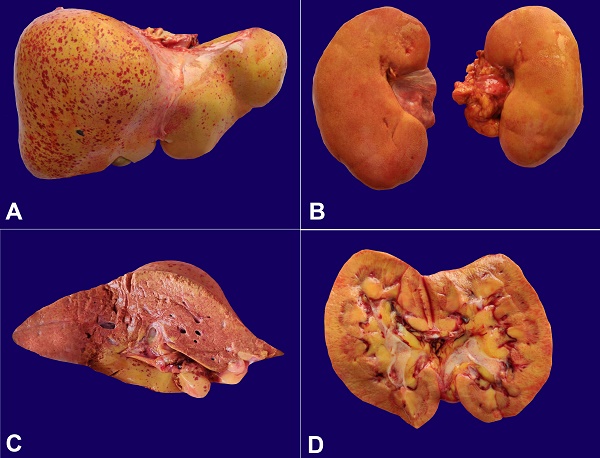 Figure 1
Gross examination of: A – Liver showing pinhead size hemorrhage over the liver surface and yellowish discoloration; B – Kidneys with pinpoint size hemorrhage over the kidney surface and yellowish discoloration; C – Liver cut-surface depicting pinpoint hemorrhages within the hepatic parenchyma; D – Kidney cut section with pinpoint hemorrhage and yellowish discoloration of the renal parenchyma.
Figure 1
Gross examination of: A – Liver showing pinhead size hemorrhage over the liver surface and yellowish discoloration; B – Kidneys with pinpoint size hemorrhage over the kidney surface and yellowish discoloration; C – Liver cut-surface depicting pinpoint hemorrhages within the hepatic parenchyma; D – Kidney cut section with pinpoint hemorrhage and yellowish discoloration of the renal parenchyma.
Histopathological examination of the lung showed acute interstitial inflammatory cell infiltrates along with multiple focal alveolar hemorrhages in both lungs (Figure 22B). The heart showed focal necrotic fibers with focal acute myocarditis (Figure 2C).
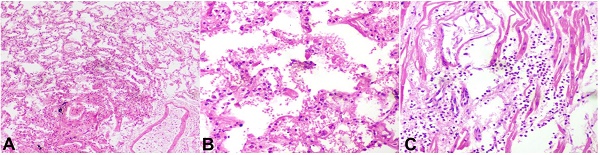 Figure 2
Photomicrographs of the lung (A and B) and the heart (C). A and B – Depict inflammatory cell infiltrates along with focal alveolar hemorrhage (H&E, 4X and 10X respectively); C – Depicts focal necrotic fibers with neutrophilic infiltrate suggestive of focal acute myocarditis. (H&E, 10X).
Figure 2
Photomicrographs of the lung (A and B) and the heart (C). A and B – Depict inflammatory cell infiltrates along with focal alveolar hemorrhage (H&E, 4X and 10X respectively); C – Depicts focal necrotic fibers with neutrophilic infiltrate suggestive of focal acute myocarditis. (H&E, 10X).
The liver showed non-zonal necrosis, karyorrhexis, vacuolization, intracellular bile pigment deposition, mild periportal inflammation, and piecemeal necrosis (Figure 33B). Kidneys showed vacuolization of proximal tubular cells and multifocal necrosis of lining epithelial cells with sparing of glomeruli (Figure 3C). Pancreas showed focal fat necrosis along with necrosis of large areas of pancreatic parenchyma (Figure 3D). Bone marrow histology was not carried out. All features are suggestive of multiorgan failure comprising of submassive hepatic necrosis, focal acute myocarditis, acute renal tubular necrosis, and pancreatic necrosis typical of phosphorus poisoning, which was confirmed after qualitative chemical analysis report showed the presence of phosphorus in tissues sampled during the autopsy.
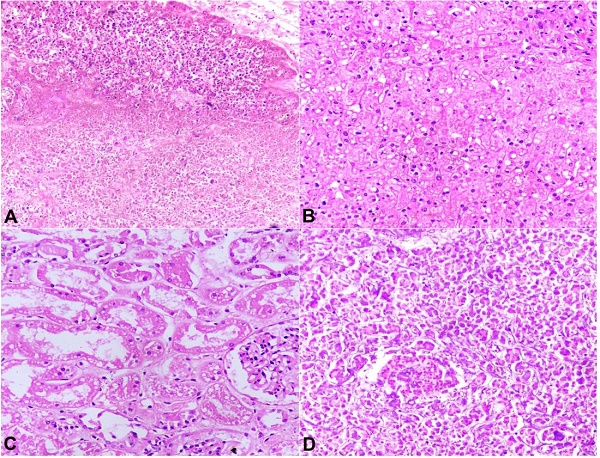 Figure 3
Photomicrographs of the liver (A, B), Kidney (C), and Pancreas (D). A – Shows non-zonal necrosis, karyorrhexis, vacuolization, and piecemeal necrosis (H&E, 4X), B – Shows vacuolization in liver tissue (H&E, 10X); C – shows vacuolization of the proximal tubular cells and multifocal necrosis of lining epithelial cells with sparing of the glomeruli (H&E, 10X); D – shows parenchymal necrosis of pancreas (H&E, 10X).
Figure 3
Photomicrographs of the liver (A, B), Kidney (C), and Pancreas (D). A – Shows non-zonal necrosis, karyorrhexis, vacuolization, and piecemeal necrosis (H&E, 4X), B – Shows vacuolization in liver tissue (H&E, 10X); C – shows vacuolization of the proximal tubular cells and multifocal necrosis of lining epithelial cells with sparing of the glomeruli (H&E, 10X); D – shows parenchymal necrosis of pancreas (H&E, 10X).
DISCUSSION
Yellow phosphorus is a toxic substance that is used in match industries, fireworks industries, and rodenticide products.9 Developing and underdeveloped countries have reported intoxication with yellow phosphorus, but rarely in developed countries. In developing countries, the intoxication generally results from accidental oral ingestion, although suicidal ingestion is also not uncommon.10,11
Ratol paste contains 3% of yellow phosphorus, a far more toxic substance than the red phosphorus.12,13 Yellow phosphorus is categorized as a highly lethal rodenticide when ingested doses exceed 1 mg/kg. In our case, the deceased ingested approximately 10-12gms of yellow phosphorus rodenticide. As reported in the literature, victims of yellow phosphorus poisoning may be initially symptomatic; however, recovery is observed after 2-3 days, and later on, features of acute liver failure develop.12In our case, the patient had a similar progression of complications. Hence, we surmise that patients with acute yellow phosphorus poisoning should be monitored closely for a week since mortality is not recorded after 8 days.14
Yellow phosphorus not only affects the liver, but its toxic effects are also observed in the central nervous system which includes restlessness, irritability, drowsiness, lethargy, stupor, or coma due to liver disfunction;15,16 cardiovascular toxicity with arrhythmias and hemodynamic instability;12,13 acute tubular necrosis and bone marrow toxicity like thrombocytopenea.17 Fernandez and Canizares18 reviewed 15 cases of yellow phosphorus poisoning and found that 87% of the patient after yellow phosphorus poisoning have some hepatic derangement and 27% developed fulminant hepatic failure and died. Liver histology shows steatohepatitis and necrosis. Santos et al.19 described three cases of white phosphorus intoxication with acute liver failure secondary to the consumption of firecrackers. In one case, liver injury improved with supportive care, in the other, the patient required liver transplantation, and the third case had a fatal outcome. Similarly, Nalabothu et al.4 found a 28% mortality rate in his study, mostly related to the Model for End-stage Liver Disease (MELD) score. MELD score greater than 40 was related to death, while the survivors presented the score lower than 12. Our patient’s highest MELD score was 36. McCarron16 found a range of 23-73% mortality in yellow phosphorus toxicity depending on clinical manifestations, those with early central nervous system manifestations had a poorer prognosis. There is no antidote for phosphorus poisoning,12,15 and the only treatment is early decontamination followed by monitoring of liver function and supportive care.12,13 Some researchers recommend gastric lavage with 1:5000 potassium permanganate followed by activated charcoal and mineral oil cathartic.16,17 Fernandez et al.18 found that NAC showed no benefit; but on the contrary, Nalabothu et al.4 suggest that the early use of NAC improves outcomes for all rodenticide poisonings with liver failure and survival rates varied with the timing of NAC administration. In this setting, the survival rate was 76% if NAC was administered on Day 1, 40% if administered on the 2nd day, and 23% if administered on or after the 3rd day after the rodenticide ingestion.4 However, this outcome is confounded by an early gastric lavage in patients that were hospitalized immediately after the rodenticide ingestion. In our case, NAC was administered on day 1 after a confirmed history of yellow phosphorus poisoning; however, the outcome was unfavorable. Yellow phosphorus is rapidly absorbed through the gastrointestinal mucosa, and approximately 70% are accumulated in the liver within 2 to 3 hours. It also accumulates to a lesser extent in the heart (12%), kidneys (4%), pancreas (0.4%), and brain (0.39%), and also leads to damage in those organs.16 Histopathological changes, in our case, were mainly detected in the lungs, heart, liver, kidneys, and pancreas. No significant pathological change, other than congestion, was observed in the brain. These characteristic histopathological findings are fat infiltration, vacuolization, necrosis in different organs, mainly liver, kidney along with focal myocarditis. The multiorgan failure, with fulminant hepatic failure, acute tubular necrosis, and toxic myocarditis, is responsible for the fatal outcome. The toxic effect of yellow phosphorus occurs in the endoplasmic reticulum and the mitochondria, leading to (i) a decreased synthesis of the apolipoprotein portion of the very low-density lipoproteins (VLDL), (ii) decrease production of adenosine triphosphate (ATP) and (iii) inhibit the fatty acid oxidation. This combined effect leads to fat deposition and cellular damage in different organs.20
CONCLUSION
Yellow phosphorus is a cheap and effective rodenticide. However, the number of accidental poisoning and deaths among children and adults can be neglected. We agree with several other authors in banning the use of yellow phosphorus in rodenticides and fireworks in its currently packaged and lethal form. We have also discussed diagnosis and management in the case of liver failure from yellow phosphorus and its prognosis. Early and excellent supportive care is the key factor in reducing morbidity and mortality.
Abbreviations: ALT = Alanine Aminotransferase; AP = Alkaline Phosphatase; AST = Aspartate Aminotransferase; ATP = Adenosine Triphosphate; NAC = N-acetylcysteine; RV = Reference Value; USG = Ultrasonography; VLDL = Very Low-Density Lipoproteins.
References
Brent J, Wallace KL, Burkhart KK. Phosphorus. In: Brent J, Wallace KL, Burkhart KK, Phillips SD, Donovan JW, editors. Critical Care Toxicology – Diagnosis and management of the critically poisoned patient. Philadelphia, PA: Elsevier Mosby; 2005. pp. 851-61.
Karanth S, Nayyar V. Rodenticide-induced hepatotoxicity. J Assoc Physicians India. 2003;51:816-7. PMid:14651148.
Nalabothu M, Monigari N, Acharya R. Clinical profile and outcomes of rodenticide poisoning in tertiary care hospital. IJSRP. 2015;5:1-12.
Chikkaveeraiah SK, Marijayanth M, Reddy PK, Kaluvakuri S. Clinical profile and outcome of rodenticide poisoning in patients admitted to a tertiary care teaching hospital in Mysore, Karnataka. India. Int J Res Med Sci. 2016;4:5023-7. http://dx.doi.org/10.18203/2320-6012.ijrms20163811.
González-Andrade F, López-Pulles R. White phosphorous poisoning by oral ingestion of firecrackers or little devils: Current experience in Ecuador. Clin Toxicol (Phila). 2011;49(1):29-33. http://dx.doi.org/10.3109/15563650.2010.547860. PMid:21288149.
Ghoshal AK, Porta EA, Hartroft WS. The role of lipo-peroxidation in the pathogenesis of fatty livers induced by phosphorus poisoning in rats. Am J Pathol. 1969;54(2):275-91. PMid:5765566.
Kannan K. Modi A textbook of medical jurisprudence and toxicology. 25th ed. New Delhi: Lexis Nexis Butterworths Wadhwa; 2016. p. 57.
Lee WM, Larson AM, Stravitz RT. AASLD position paper: the management of acute liver failure: Update. Hepatology. 2011;55:965-67.
Saoji AA, Lavekar AS, Salkar HR, Pawde GB, Tripathi SS. A case on suicidal poisoning associated with Ratol and a perspective on yellow phosphorus poisoning. Int J Re Sci&Techi. 2014;10:223-5.
Notes
Notes
How to cite: Soni JP, Ghormade PS, Akhade S, Chavali K, Sarma B. A fatal case of multi-organ failure in acute yellow phosphorus poisoning. Autopsy Case Rep [Internet]. 2020;10(1): e2020146.
https://doi.org/10.4322/acr.2020.146
Ethical Concerns: As per the law of India, if an autopsy is performed in a medicolegal case the consent of the family member is not desired. Being a medicolegal autopsy case report the identity and credentials of the victim are kept confidential and the clearance from the institutional ethics committee is not warranted.
Financial support: None
Conflict of interest declaration
Conflict of interest: None
Author notes
Author contributions: All authors contributed equally to this work from performing the autopsy to writing the manuscript. All authors proofread and approved the final paper’s version to be published.
Correspondence Jai Prakash Soni Gajra Raja Medical College - Department of Forensic Medicine and Toxicology Gwalior, Madhya Pradesh, 474009 Gwalior – Madhya Pradesh – India Phone: +91 8349400899dr.jaiprakashsoni@gmail.com
