Letter to the Editor
Intramedullary teratoma
 Adilson José Manuel de Oliveira
Vinicius Monteiro de Paula Guirado
Vitor Nagai Yamaki
Fernando Pereira Frasseto
Adilson José Manuel de Oliveira
Vinicius Monteiro de Paula Guirado
Vitor Nagai Yamaki
Fernando Pereira Frasseto
Intramedullary teratoma
Autopsy and Case Reports, vol. 9, no. 4, e2019105, 2019
Hospital Universitário da Universidade de São Paulo
Received: 08 June 2019
Accepted: 01 July 2019
Keywords: Teratoma, Spinal Cord Neoplasms, Neurosurgery
Dear Editor,
We present a case of a young woman with an intramedullary lesion and symptoms of spinal cord compression (lower limbs weakness and urinary retention). The MRI images rendered the preoperative differential diagnoses of neurofibroma and schwannoma; however, teratoma was suspected with the intraoperative findings, which was confirmed by the histological report. Teratoma of the central nervous system is a rare entity that originates from the embryonic tissues of the three primary embryonic leaflets classified as (i) mature, (ii) immature and (iii) malignant. The intramedullary teratoma comprises 0.2% of all central nervous system tumors. The clinical picture varies according to the site of the lesion, and the most frequent location is the medullary cone. The outcome is usually favorable when a complete resection is feasible. Although complete resection was not possible in our case, the patient had symptomatic improvement. We present the case of a 35-year-old female, who was referred to our emergency department with a 3-month history of intense low back pain radiating to the lower limbs without any specific dermatome distribution, followed by a progressive loss of the lower limbs’ muscular strength, and urinary retention over the last month. On the neurological examination, the patient presented a grade-III muscular strength for the hip flexion and extension on de right side, and grade-IV on the left side; foot drop on the right side, bilateral L1 to L5 hypoesthesia, bilateral exaggerated patellar reflex, and bilateral Babinski sign. The laboratory workup was normal, the lumbar spine computed tomography (CT) showed intra-spinal canal injury with scarce zones of calcification in the topography of the second to the fourth lumbar vertebra (Figure 1A), and the magnetic resonance imaging (MRI) showed intramedullary lesion with a heterogeneous aspect in T2 and T1 weighted images, the later showed marked enhancement after gadolinium injection (Figure 1B).
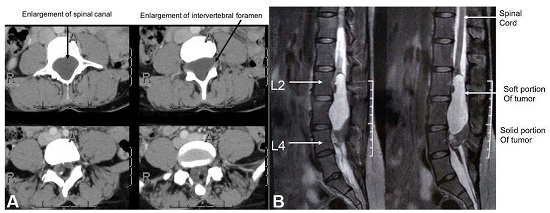
Figure 1
A – spine CT axial plane showing intraspinal lesion with enlargement of vertebral canal suggesting a slow growing lesion; B – Spine MRI, sagittal plane showing lumbosacral region showing a heterogenous intramedullary lesion from L2 to L4 levels.
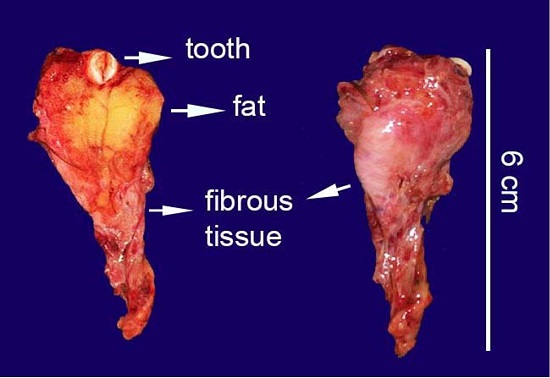
Figure 2
Gross view of the surgical specimen, ventral, and dorsal views are showing fat, fibrous tissues, and a tooth.
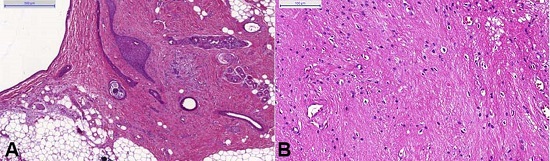
Figure 3
Photomicrographs of the surgical specimen. A – presence of mature, adult-type tissues - skin with cutaneous appendages, connective, and adipose tissues; B – neural component, predominantly composed of glial cells and neuropil.
- 1.
1
Always consider all diagnostic hypotheses for intramedullary lesions, even the rarest ones such as teratomas because it can change the surgical approach, the differential diagnosis is challenging because of unspecific clinical features mainly when the associated spinal malformations lacks.4
- 2.
2
Partial resection with preservation of neurological function is a valid option, although most authors advocate radical resection there are reports of partial resections with favorable clinical outcomes and low rates of symptomatic recurrences.5
References
Hosoi K. Intradural teratoid tumors of the spinal cord. Arch Pathol. 1931;11:875-83.
Traul DE, Shaffrey ME, Schiff D, Part I. Spinal-cord neoplasms—intradural neoplasms. Lancet Oncol. 2007;8(1):35-45. http://dx.doi.org/10.1016/S1470-2045(06)71009-9. PMid: 17196509
Hamada H, Kurimoto M, Hayashi N, Hirashima Y, Matsumura N, Endo S. Intramedullary spinal teratoma with spina bifida. Childs Nerv Syst. 2001;17(1-2):109-11. http://dx.doi.org/10.1007/s003810000399. PMid: 11219616
Barahona EA, Olvera JN, Liquidano ME, et al. A special case of intramedullary teratoma in an adult: Literature review. Rev Med Hosp Gen Mex. 2018;81(4):237-42.
Ak H, Ulu MO, Sar M, Albayram S, Aydın S, Uzan M. Adult intramedullary mature teratoma of the spinal cord: Review of the literature illustrated with an unusual example. Acta Neurochir. 2006;148(6):663-9. http://dx.doi.org/10.1007/s00701-006-0755-z. PMid: 16523223
Allsopp S, Sgouros S, Barber P, Walsh AR. Spinal teratoma: is there a place for adjuvant treatment? Two cases and a review of the literature. Br J Neurosurg. 2000;14(5):482-8. http://dx.doi.org/10.1080/02688690050175364. PMid: 11198778
Notes
Author notes
Correspondence : Adilson José Manuel de Oliveira Alameda Santos, 663, Apt 34B – Cerqueira Cesar – São Paulo/SP – Brazil CEP: 01419-000 Phone: +55 (11) 99779-2709 adilsonvalmont@gmail.com
Conflict of interest declaration