Image in Focus
Cardiac Myxoma
Cardiac Myxoma
Autopsy and Case Reports, vol. 6, no. 2, pp. 5-7, 2016
Hospital Universitário da Universidade de São Paulo
Keywords: Heart Neoplasms, Myxoma
Figure
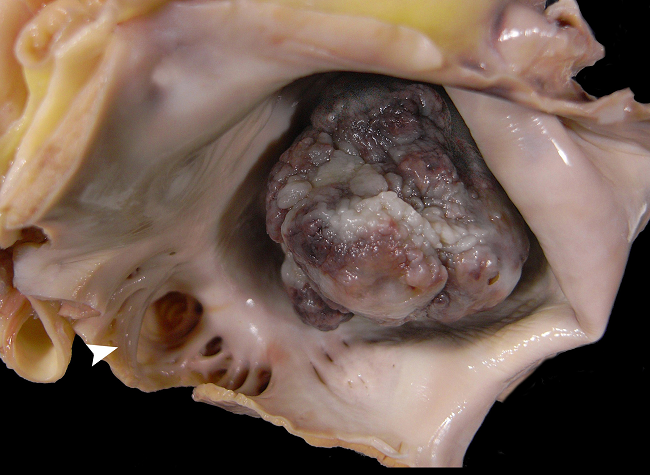
Huge left atrial myxoma (measuring 4.0 × 3.5 cm) occupying almost the whole atrial cavity. Note the warty appearance of the tumor surface. The left atrial appendage (arrowhead) is open and does not show thrombosis.
Image courtesy Dr. Vera Demarchi Aiello
Primary cardiac tumors (PCT) are rare, accounting for 0.0017-0.03% in autopsy series,1,2 in contrast to metastatic tumors of the heart, which are 30 times more frequent.3,4 Nearly 75% of PCT are benign and most often represented by a myxoma in 50% of cases in the adult population.5
The World Health Organization defines a cardiac myxoma (CM) as a neoplasm composed of stellate to plump, cytologically bland, mesenchymal cells set in a myxoid stroma.6
Approximately 95% of CMs occurs isolated in a wide range of age. However, they occur more frequently among women in the fifth or sixth decade of life.7-9
For a time, myxomas were believed to arise from endocardial thrombi10 and some evidence suggests an association with Herpes simplex virus 1 infections11; however, their tumoral histogenesis remains unknown. Meanwhile, ultrastructure analysis—added to immunohistochemical investigation—suggests that CM is more likely derived from a pluripotent mesenchymal stem cell or sub-endothelial cell. Chromosomal clonal abnormalities, mostly on chromosome 2, 12, and 17, appear to be implicated in the myxoma formation, although defects on chromosome 1q32, the loss of the Y chromosome, and the telomeric association of chromosome 13 and 15, have also been involved.12-14
CMs are mostly pedunculated and solitary, and arise primarily adjacent to the lamina of the fossa ovalis (corresponding to the embryonic septum primum) and develop in the left atrium in 75% of cases, followed by the right atrium (18%),15 the right and left ventricles (3% in each), and the valves (1%).15-20 Multiple myxomas represent 5% of the cases, half of which are of bilateral origin.21
Although CM is a benign tumor, reports on its malignancy are well-known, which include: (i) local relapse; (ii) local invasiveness; and (iii) distant metastasis.12 The potential for malignant transformation is controversial, despite the publication of some reports of sarcomas arising from CM recurrences.22,23
Clinical manifestations of CMs are protean and may vary from asymptomatic cases (with a tumor < 4 cm) to unexpected sudden death (generally caused by blood flow obstruction or embolization). In most cases, the clinical presentation will depend on the tumor size, mobility, and location. One or more symptoms of the following triad will usually be present: (i) embolic phenomena (present in 30-40% of cases and usually associated with a villous surface of the tumour)24; (ii) intracardiac flow obstruction (present in almost 50% of cases); and (iii) constitutional symptoms (present in 20-60% of cases). In general, the most common signs and symptoms are non-specific and include dyspnea, palpitation (due to atrial fibrillation), lower limbs edema, hepatomegaly, angina, syncope, cough, and pulmonary edema. The constitutional symptoms, characterized by fatigue, fever, myalgia, arthralgia, and weight loss, are probably related to interleukin-6 cytokine production.25
The diagnosis of a CM is mostly done with echocardiography, both transthoracic and transesophageal, which represent the imaging modality of choice, although the latter permits precise information for the scheduling of surgery. Due to the rarity and consequent unfamiliarity of most general practitioners with this entity, CMs are sometimes misdiagnosed. Differential diagnosis should include intracardiac thrombus and other cardiac tumors.
REFERENCES
1 Benjamin HS. Primary fibromyxoma of the heart. Arch Pathol (Chic). 1939;27:950.
2 Straus R, Merliss R. Primary tumor of the heart. Arch Pathol (Chic). 1945;39:74.
3 Lam KY, Dickens P, Chan AC. Tumors of the heart. A 20- year experience with a review of 12,485 consecutive autopsies. Arch Pathol Lab Med. 1993;117(10):1027-31. PMid:8215825
4 Reynen K. Frequency of primary tumors of the heart. Am J Cardiol. 1996;77(1):107. http://dx.doi.org/10.1016/S0002-9149(97)89149-7. PMid:8540447
5 Silverman NA. Primary cardiac tumors. Ann Surg. 1980;191(2):127-38. http://dx.doi.org/10.1097/00000658-198002000-00001. PMid:7362282
6 Burke AP, Tazelar H, Gomez-Roman JJ, Loire R, et al. World Health Organization: tumours of the lung, pleura, thymus and heart. Lyon: IARC Press; 2004.
7 Goodwin JF. Diagnosis of left atrial myxoma. Lancet. 1963;1(7279):464-8. http://dx.doi.org/10.1016/S0140-6736(63)92359-6. PMid:13949121
8 Kusumi T, Minakawa M, Fukui K, et al. Cardiac tumor comprising two components including typical myxoma and atypical hypercellularity suggesting a malignant change. Cardiovasc Pathol. 2009;18(6):369-74 PMid:18619858
9 Wold LE, Lie JT. Cardiac myxomas: a clinicopathologic profile. Am J Pathol. 1980;101(1):219-40. PMid:7446701
10 Ryou KS, Lee SH, Park SH, Park J, Hwang SK, Hamm IS. Multiple fusiform myxomatous cerebral aneurysms in a patient with Carney complex. J Neurosurg. 2008;109(2):318-20. http://dx.doi.org/10.3171/JNS/2008/109/8/0318. PMid:18671646
11 Li Y, Pan Z, Ji Y, et al. Herpes simplex virus type 1 infection associated with atrial myxoma. Am J Pathol. 2003;163(6):2407-12. http://dx.doi.org/10.1016/S0002-9440(10)63595-X. PMid:14633612
12 Amano J, Kono T, Wada Y, et al. Cardiac Myxoma: Its origin and tumor characteristics. Ann Thorac Cardiovasc Surg. 2003;9(4):215-21. PMid:13129418
13 Richkind KE, Wason D, Vidaillet HJ. Cardiac myxoma characterized by clonal telomeric association. Genes Chromosomes Cancer. 1994;9(1):68-71. http://dx.doi.org/10.1002/gcc.2870090112. PMid:7507703
14 Dobin S, Speights VO Jr, Donner LR. Addition (1)(q32) as the sole clonal chromosomal abnormality in a case of cardiac myxoma. Cancer Genet Cytogenet. 1997;96(2):181-2. PMid:9216729
15 Burke AP, Virmani R. Cardiac myxoma. A clinicopathologic study. Am J Clin Pathol. 1993;100(6):671-80. http://dx.doi.org/10.1093/ajcp/100.6.671. PMid:8249916
16 Yoshikai M, Kamohara K, Fumoto H, Kawasaki H. Left ventricular myxoma originating from the papillary muscle. J Heart Valve Dis. 2003;12(2):177-9. PMid:12701789
17 Cina SJ, Smialek JE, Burke AP, Virmani R, Hutchins GM. Primary cardiac tumors causing sudden death: a review of the literature. Am J Forensic Med Pathol. 1996;17(4):271-81. http://dx.doi.org/10.1097/00000433-199612000-00001. PMid:8947350
18 Karlof E, Salzberg SP, Anyanwu AC, Steinbock B, Filsoufi F. How fast does an atrial myxoma grow? Ann Thorac Surg. 2006;82(4):1510-2. http://dx.doi.org/10.1016/j.athoracsur.2005.11.014. PMid:16996968
19 McCarthy PM, Schaff HV, Winkler HZ, Lieber MM, Carney JA. Deoxyribonucleic acid ploidy pattern of cardiac myxomas. Another predictor of biologically unusual myxomas. J Thorac Cardiovasc Surg. 1989;98(6):1083-6. PMid:2586124
20 Japa D, Mashhadi M, Peter S. Giant left Atrial Myxoma Induces Mitral Valve Obstruction and Pulmonary Hypertension. J Clin Diagn Res. 2016;10(1):ED08-09. PMid:26894077
21 Vijan V, Vupputuri A, Nair RC. An unusual case of biatrial myxoma in a young female. Case Rep Cardiol. 2016(2016):1-3. http://dx.doi.org/10.1155/2016/3545480
22 Shinfeld A, Katsumata T, Westaby S. Recurrent cardiac myxoma: seeding or multifocal disease? Ann Thorac Surg. 1998;66(1):285-8. http://dx.doi.org/10.1016/S0003-4975(98)00481-0. PMid:9692493
23 Kasugai T, Sakurai M, Yutani C, et al. Sequential malignant transformation of cardiac myxoma. Acta Pathol Jpn. 1990;40(9):687-92. PMid:2260476
24 Oliveira R, Branco L, Galrinho A, et al. Cardiac myxoma: a 13-year experience in echocardiographic diagnosis. Rev Port Cardiol. 2010;29(7-8):1087-100. PMid:21066964
25 Wang JG, Li YJ, Liu H, Li NN, Zhao J, Xing XM. Clinicopathologic analysis of cardiac myxomas: Seven years’experience with 61 patients. J Thorac Dis. 2012;4(3):272-83. PMid:22754666
Notes
Author notes
Correspondence Vera Demarchi Aiello Surgical Pathology Section - Laboratory of Pathology - Heart Institute - Hospital das Clínicas - Universidade de São Paulo (USP) Av. Dr. Enéas C. Aguiar, 44 - São Paulo/SP - Brazil CEP: 05403-000 Phone: + 55(11) 2661-5252 E-mail: anpvera@incor.usp.br
Conflict of interest declaration