Image in Focus
Periprostatic venous thrombosis
Periprostatic venous thrombosis
Autopsy and Case Reports, vol. 6, no. 3, pp. 3-5, 2016
Hospital Universitário da Universidade de São Paulo
Received: 20 May 2016
Accepted: 15 June 2016
Keywords: Cancer, Glioma, Neurosurgery, Pulmonary embolism, Periprostatic venous thrombosis
Figure
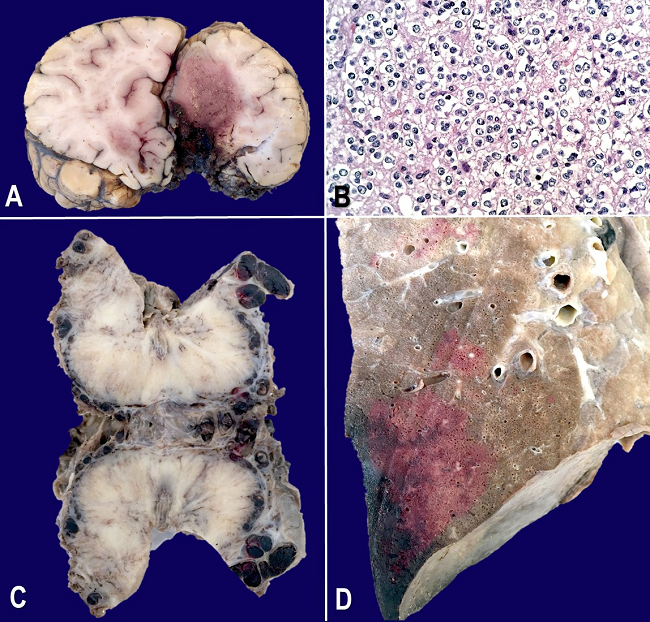
Pathological findings of a 33-year-old male who underwent a craniotomy for resection of a WHO grade 2 frontal lobe oligodendroglioma; A - Coronal section of the encephalic frontal lobe showing a poorly defined reddish smooth mass in the cortex and white matter, with enlargement of the affected area, especially the superior frontal gyrus on the left hemisphere; B - Photomicrography of the central nervous system tumor depicting a diffusely infiltrating glioma composed of monomorphic cells with uniform round vesicular nuclei, distinct small nucleoli, and perinuclear halo (“fried egg appearance”); C - Gross examination of the prostate gland and surrounding tissue with extensive recent periprostatic venous thromboses; D - Gross examination of the lung showing a wedge-shaped, hemorrhagic area, based on the pleura, which corresponds to a recent pulmonary infarct due to a pulmonary embolism.
Image courtesy Dr. Eduardo Paulino Júnior
Oligodendroglial tumors account for less than 10% of diffuse type gliomas, which are graded from low to high according to the WHO 2015 classification.1 Patients harboring brain tumors — especially those with high-grade gliomas (HGG) — have a higher risk of developing venous thromboembolism (VTE), including deep venous thrombosis (DVT) and/or pulmonary embolism (PE).2,3 Local synthesis of the tissue factor (TF), along with many other factors, is related to an increased VTE rate in these patients, especially those who have undergone cranial neurosurgical procedures — particularly a biopsy or a subtotal resection. The combination of a neurosurgical intervention and a remnant tumor constitute a higher risk for thromboembolic events.3 In a previous study,3 among 63 HGG patients who were followed over a median period of 348 days, 15 (24%) presented VTE; 6 (40%) had DVT, which was located in the lower extremity in five of them; and 9 (60%) had PE (three in combination with DVT).
TF,4-7 a potent procoagulant factor whose synthesis is up-regulated in a variety of neoplasms (including HGG), might play an important role in the VTE pathogenesis. TF acts as a high-affinity receptor/co-activator for the coagulation factor VII/VIIa and triggers the coagulation cascade. A complex TF/VIIa formation activates factor X and leads to the generation of thrombin, which catalyzes the formation of fibrin and the activation of platelets, resulting in vascular occlusion and ischemia as well as inflammation and angiogenesis. In glioma cells, the amount of TF expression correlates with the histological grade.
Tumor dormancy is influenced by TF.4,7 Thus, indolent human glioma cells deficient for TF remain viable in cell cultures, but are permanently dormant for nearly a year when they are injected at a specific site, while the expression of TF leads to a stepwise transition to latent and overt tumor growth phases — a process preceded by the recruitment of vascular cells (CD105+) and myeloid (CD11b+ and F4/80+) cells. Importantly, the microenvironment orchestrated by TF expression drives permanent changes in the phenotype gene expression profile, the DNA copy number, and the DNA methylation state of tumor cells that escaped from dormancy. Some authors postulate that procoagulant events in the tissue microenvironment (niche) may affect the fate of occult tumor cells, including biological and genetic progression to initiate full-blown malignancy.4
Periprostatic or paravaginal areas are rarely considered to be sites of clot origin in patients with PE.8,9 The majority of emboli have been demonstrated to originate in the veins of the legs. As far as we know, the first reported case of PE as a result of thrombosis from the periprostatic venous plexus in a young patient with a normal prostate gland and no history of prostate trauma was published in 2003.8 Three other cases were described three years later.9
In 1819, Gilbert Breschet provided the first detailed anatomic description of the vertebral venous plexus (VVP). It was described as a large plexiform valveless network of vertebral veins consisting of three interconnecting divisions and spanning the entire spinal column with connections to the cranial dural sinuses, which were distributed in a longitudinal pattern and ran parallel to the venae cavae with which they communicated, with multiple interconnections.10
In 1940, Oscar V. Batson reported the true functionality of the VVP by proving the continuity of the prostatic venous plexus with the VVP and proposed this route as the most plausible explanation for the distribution of prostate metastatic disease. With his seminal work, Batson reclassified the human venous system to consist of caval, pulmonary, portal, and vertebral divisions. Further advances in imaging technology confirmed Batson’s results. Today, the VVP is considered part of the cerebrospinal venous system, which is regarded as a unique, large-capacitance, valveless plexiform venous network in which flow is bidirectional. This system plays an important role in the regulation of intracranial pressure with changes in posture and venous outflow from the brain; whereas, in disease states, it provides a potential route for the spread of tumors, infections, or emboli.10
REFERENCES
1 Wesseling P, van den Bent M, Perry A. Oligodendroglioma: pathology, molecular mechanisms and markers. Acta Neuropathol. 2015;129(6):809-27. http://dx.doi.org/10.1007/s00401-015-1424-1. PMid:25943885.
2 Smith TR, Nanney AD 3rd, Lall RR, et al. Development of venous thromboembolism (VTE) in patients undergoing surgery for brain tumors: results from a single center over a 10 year period. J Clin Neurosci. 2015;22(3):519-25. http://dx.doi.org/10.1016/j.jocn.2014.10.003. PMid:25533212
3 Simanek R, Vormittag R, Hassler M, et al. Venous thromboembolism and survival in patients with high-grade glioma. Neuro-oncol. 2007;9(2):89-95. http://dx.doi.org/10.1215/15228517-2006-035. PMid:17327573
4 Magnus N, Garnier D, Meehan B, et al. Tissue factor expression provokes escape from tumor dormancy and leads to genomic alterations. Proc Natl Acad Sci USA. 2014;111(9):3544-9. http://dx.doi.org/10.1073/pnas.1314118111. PMid:24520174
5 Hamada K, Kuratsu J, Saitoh Y, Takeshima H, Nishi T, Ushio Y. Expression of tissue factor correlates with grade of malignancy in human glioma. Cancer. 1996;77(9):1877-83. http://dx.doi.org/10.1002/(SICI)1097-0142(19960501)77:9<1877::AID-CNCR18>3.0.CO;2-X. PMid:8646688
6 Jo JT, Schiff D, Perry JR. Thrombosis in brain tumors. Semin Thromb Hemost. 2014;40(3):325-31. http://dx.doi.org/10.1055/s-0034-1370791. PMid:24599439.
7 D'Asti E, Fang Y, Rak J. Brain neoplasms and coagulation-lessons from heterogeneity. Rambam Maimonides Med J. 2014;5(4):e0030. http://dx.doi.org/10.5041/RMMJ.10164. PMid:25386346.
8 Reddy PV, Solomon D. Pulmonary emboli from massive thrombosis of the periprostatic venous plexus mimicking acute respiratory distress syndrome. Chest. 2003;124(4):251S. http://dx.doi.org/10.1378/chest.124.4_MeetingAbstracts.251S.
9 Elhammady G, Schubeck AT, El-Najjar V, Robinson MJ. Postmortem demonstration of the source of pulmonary thromboembolism: the importance of the autopsy. Case Rep Vasc Med. 2011(2011):1-3. http://dx.doi.org/10.1155/2011/108215. PMid:22937459.
10 Nathoo N, Caris EC, Wiener JA, Mendel E. History of the vertebral venous plexus and the significant contributions of Breschet and Batson. Neurosurgery. 2011;69(5):1007-14, discussion 1014. PMid:21654535
Notes
Author notes
Correspondence *Eduardo Paulino Júnior Pathology and Forensic Department - Faculty of Medicine - Universidade Federal de Minas Gerais (UFMG) Av. Prof. Alfredo Balena, 190 - Belo Horizonte/MG - Brazil CEP: 30130-100 Phone: +55 (31) 3409-9755 edupatol@gmail.com
Conflict of interest declaration