Image in Focus
Pericarditis is the inflammatory process involving the pericardium as a result of a systemic disease or a primary pericardium disorder.1 The actual incidence of pericarditis is difficult to ascertain,2 most probably because of under-reported or misdiagnosed cases. In the 19th century, Sir William Osler stated that pericarditis was one of the most serious diseases overlooked by practitioners.3 Even so, the rate of hospitalization by this diagnosis is estimated in 3.32 cases per 100,000 person-years, which corresponds to 0.2% of all causes of hospitalization in cardiology centers,4 with an incidence of 1.06% found in autopsy case series.5
Didactically, pericarditis can be morphologically classified in five types: (i) fibrinous; (ii) serous; (iii) purulent; (iv) hemorrhagic; or (v) caseous.6 The image presented herein refers to a typical fibrinous pericarditis, also known as “bread and butter” pericarditis.7 In such an entity, the pericardium, which is regularly smooth and bright, becomes opaque and granular, and macroscopically resembles two pieces of buttered bread pressed together then pulled apart. The histology shows the deposition of fibrin and leukocytic exudate involving the pericardial leaflets.8
Antonio Benivieni (1443-1502), a Florentine physician and a contemporary of Leonardo da Vinci, was assigned the first description of fibrinous pericarditis. However, René Laennec (1781-1826), also known for creating the stethoscope, was the first to register the analogy of this type of pericarditis with “buttered bread”9 in his book, A Treatise on the Diseases of the Chest and on Mediate Auscultation10
The image presented in Figure 1 was obtained during the autopsy of a 25-year-old man who presented a 5-day history of high-grade fever, odynophagia, chest pain, and bloody sputum. He was hospitalized presenting marked leukocytosis with blasts in the peripheral blood smear and died 14 days later due to multiple organ failure. The autopsy revealed fibrinous pericarditis with a brighter yellow exudate than usual (probably due to hyperbilirubinemia, with direct and indirect bilirubin levels of 4.61 mg/dL and 2.07 mg/dL, respectively), lungs with “beefy red consolidation” due to alveolar edema, hemorrhage, hyaline membrane, and diffuse neutrophilic infiltrate. The patient’s bone marrow was hypercellular at the expense of immature myeloid cells with areas of necrosis. The immunohistochemical study evidenced diffuse positivity for myeloperoxidase; CD117-positivity for 30% of the viable cells; CD34-positivity for 1% of the viable cells; and negativity for the terminal deoxynucleotidyl transferase-all of which were consistent with the diagnosis of M3 acute myeloid leukemia (French-American-British classification).11
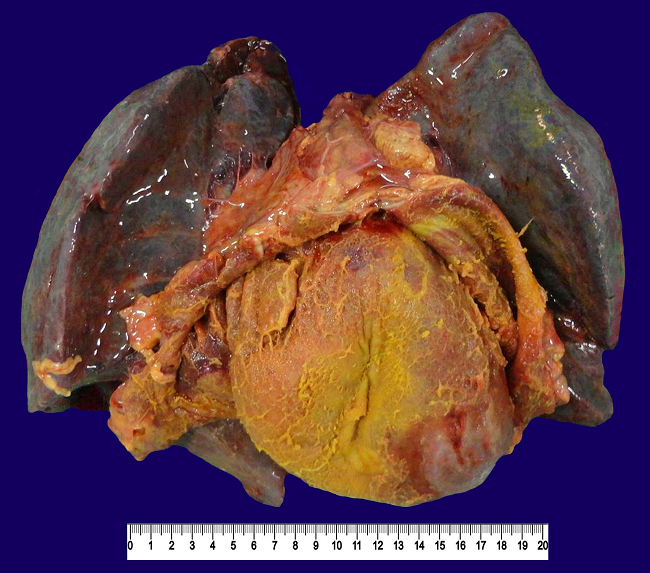
Figure 1
Gross view of the block of the thoracic organs showing the anatomic relationship between the lungs with “beefy red consolidation” and the heart recovered by bright yellow fibrin in a “bread and butter” pattern
Image courtesy Dr. Pedro Mansueto Melo de Souza and Dra. Conceição Aparecida Dornelas
Acute myocardial infarction, trauma/surgery, infection, uremia, systemic diseases, and neoplasia are among the most common causes of fibrinous pericarditis. Among the neoplasia, lung and breast malignancies stand out, followed by lymphomas and leukemia,12 although pericardial infiltration by nonlymphocytic leukemia is rarer.13 In a large case series of 420 postmortem examinations of the heart in acute leukemia,14 only 20 patients had symptoms of heart disease in life, and 9 of them had pericarditis at autopsy. In only 2 of the 9 patients, the pericarditis was the result of leukemic cell infiltrates into the pericardium; in 4 patients it was hemorrhagic; and in 2 it was pyogenic. Only 1 case remained with uncertain etiology, being fibrinous and unassociated with pericardial leukemic infiltrates, hemorrhages, or organisms, which also occurred in our case. The histopathologic study of the pericardium failed to reveal neoplastic cells, microorganisms, and viral inclusion; therefore, the precise etiology of the pericardial disease was not disclosed.
REFERENCES
1 Imazio M, Gaita F, LeWinter M. Evaluation and treatment of pericarditis: a systematic review. JAMA. 2015;314(14):1498-506. PMid:26461998 http://dx.doi.org/10.1001/jama.2015.12763
2 Troughton RW, Asher CR, Klein AL. Pericarditis. Lancet. 2004;9410(363):717-27. PMid:15001332 http://dx.doi.org/10.1016/S0140-6736(04)15648-1.
3 Osler W. The principles and practice of medicine: designed for the use of practitioners and students of medicine. 3th ed. New York: D. Appleton and Company; 1898 [cited 2016 Sept 9]. 694 p. Available from: https://archive.org/stream/principlespracti00osleuoft
4 Kyto V, Sipila J, Rautava P. Clinical profile and influences on outcomes in patients hospitalized for acute pericarditis. Circulation. 2014;130(18):1601-6. PMid:25205801 http://dx.doi.org/10.1161/CIRCULATIONAHA.114.010376
5 Friman G, Fohlman J. The epidemiology of viral heart disease. Scand J Infect Dis. 1993;88(Suppl):7-10. PMid:8516667
6 Kumar V, Abbas AK, Aster JC. Robbins & Cotran pathologic basis of disease. 9th ed. Philadelphia: Elsevier Saunders; 2015.
7 Waller BF, Taliercio CP, Howard J, Green F, Orr CM, Slack JD. Morphologic aspects of pericardial heart disease: part II. Clin Cardiol. 1992;15(4):291-8. PMid:1563133 http://dx.doi.org/10.1002/clc.4960150413
8 Klatt EC. Robbins & Cotran atlas of pathology. 3rd ed. Philadelphia: Elsevier Saunders; 2015.
9 Cohen MB. Cross your heart: some historical comments about fibrinous pericarditis. Hum Pathol. 2004;35(2):147-9. PMid:14991530 http://dx.doi.org/10.1016/j.humpath.2003.08.029
10 Laennec RTH. A treatise on the diseases of the chest and on mediate auscultation. London: R. Gilbert; 1824 [cited 2016 Aug 2]. 671 p. Available from: https://archive.org/details/treatiseondiseas1829laen
11 Bennett JM, Catovsky D, Daniel MT, et al. Proposed revised criteria for the classification of acute myeloid leukemia: a report of the French-American-British Cooperative Group. Ann Intern Med. 1985;103(4):620-5. PMid:3862359 http://dx.doi.org/10.7326/0003-4819-103-4-620
12 Roberts WC. Pericardial heart disease: its morphologic features and its causes. Proc Bayl Univ Med Cent. 2005;18(1):38-55. PMid:16200146
13 Chu J, Demello D, O’Connor DM, Chen S, Gale GB. Pericarditis as presenting manifestation of acute nonlymphocytic leukemia in a young child. Cancer. 1983;52(2):322-4. PMid:6574803 http://dx.doi.org/10.1002/1097-0142(19830715)52:2<322::AID-CNCR2820520222>3.0.CO;2-U.
14 Roberts WC, Bodey GP, Wertlake PT. The heart in acute leukemia: a study of 420 autopsy cases. Am J Cardiol. 1968;21(3):388-412. PMid:4295426 http://dx.doi.org/10.1016/0002-9149(68)90143-4.
Notes
Author notes
Correspondence *Pedro Mansueto Melo de Souza Department of Pathology and Forensic Medicine - Faculty of Medicine - Universidade Federal do Ceará (UFC) Rua Monsenhor Furtado, s/n - Rodolfo Teófilo - Fortaleza/CE - Brazil CEP: 60441-750 Phone: +55 (85) 988489581 pedro.mansueto.m.s@gmail.com
Conflict of interest declaration
