Article / Clinical Case Report
Rosai-Dorfman disease affecting the maxilla
Rosai-Dorfman disease affecting the maxilla
Autopsy and Case Reports, vol. 6, no. 4, pp. 49-55, 2016
Hospital Universitário da Universidade de São Paulo
Received: 02 October 2016
Accepted: 28 November 2016
ABSTRACT: Rosai-Dorfman disease (RDD), formerly called sinus histiocytosis with massive lymphadenopathy, is a non-neoplastic proliferative histiocytic disorder with behavior ranging from highly aggressive to spontaneous remission. Although the lymph nodes are more commonly involved, any organ can be affected. This study aimed to describe the features and the follow-up of a case of extranodal RDD. Our patient was a 39-year-old woman who was referred with an 11-month history of pain in the right maxilla. On clinical examination, some upper right teeth presented full mobility with normal appearance of the surrounding gingiva. Radiographic exams showed an extensive bone reabsorption and maxillary sinus filled with homogeneous tissue, which sometimes showed polypoid formation. An incisional biopsy demonstrated a diffuse inflammatory infiltrate rich in foamy histiocytes displaying lymphocytes emperipolesis. Immunohistochemistry showed positivity for CD68 and S-100, and negativity for CD3, CD20, and CD30. Such features were consistent with the RDD diagnosis. The patient was referred to a hematologist and corticotherapy was administrated for 6 months. RDD is an uncommon disease that rarely affects the maxilla. In the present case, the treatment was conservative, and the patient is currently asymptomatic after 5 years of follow-up.
Keywords: Histiocytosis, Sinus, Maxilla, Emperipolesis, Diagnosis, Oral.
INTRODUCTION
Rosai-Dorfman disease (RDD) or sinus histiocytosis with massive lymphadenopathy is a rare histiocytic disease of unknown etiology. Some studies have reported a relationship with autoimmune diseases, hematological malignancies, post-infectious conditions, and immune dysfunction.1,2
The most common clinical findings of RDD include extensive painless lymphadenopathy with fever, weight loss, anemia, night sweats, tonsillitis, nasal problems, and hepatosplenomegaly.3 Extranodal involvement can occur in the head and neck, particularly in the paranasal sinus and the nasal cavity. Exclusive bone lesions are exceptionally rare and usually have an unpredictable clinical course.4
The aim of this report is to describe a rare case of RDD affecting the maxilla in association with maxillary sinuses, mucosal thickening, and polypoid lesions. The differential diagnosis and prognosis are discussed.
CASE REPORT
A 39-year-old woman was seen at our institution complaining of teeth mobility and pain of the upper right teeth, which had lasted for 11 months. The patient was an artisan and addicted to marijuana. During the anamnesis, the patient denied any other symptoms or systemic alterations. On intra-oral evaluation, the clinical appearance of the upper teeth gingiva was normal (Figure 1). However, most of the upper teeth presented full mobility.
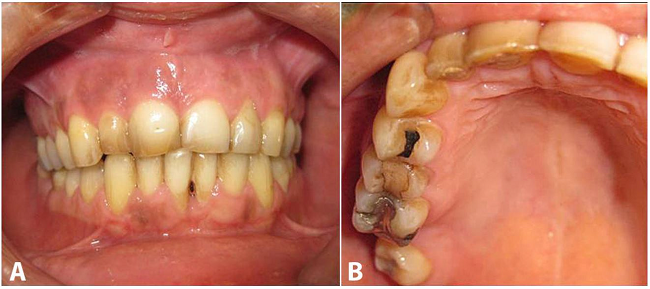
Figure 1
Intra oral examination - A and B showing no alteration of the upper teeth gingiva.
Radiographic exams showed a diffuse osteolytic image in the right maxilla with great destruction of the alveolar bone. The teeth had lost their bone support and presented characteristics of floating teeth. In addition, the lesion destroyed the cortical bone without the expansion of both the buccal and the palatal cortical plates. Polypoid lesions and mucosal thickening of both maxillary sinuses were also evident (Figures 2 and 3).
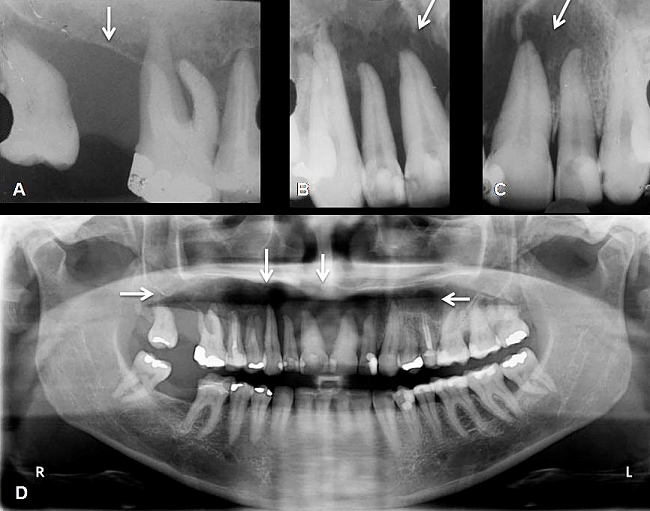
Figure 2
A-C - Periapical radiographs show a large reabsorption of the alveolar bone and floating teeth (arrows); D - Panoramic x-ray shows irregular osteolytic image in the right maxilla (arrows).
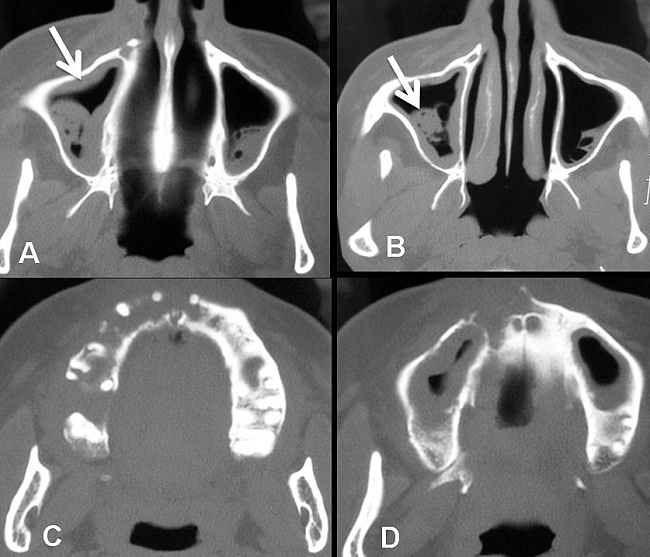
Figure 3
A - Axial computed tomography (CT) image of the paranasal sinuses showing the thickening of the sinus mucosa (arrow); B - Axial CT image of polypoid lesions within the sinus (arrow); C and D - Axial CT images of the maxilla showing an extensive reabsorption of alveolar bone of right maxilla.
The main clinical diagnostic hypotheses were Langerhans cell histiocytosis (LCH), NK/T-cell lymphoma, and sinus carcinoma. An incisional biopsy of the alveolar bone (upper right canine) was performed, and the histopathological analysis showed an intense diffuse mononuclear cell infiltration rich in xanthomatous cells, some of which had evident emperipolesis of the lymphocytes. Areas of necrosis were also observed (Figure 4A). The immunohistochemical reactions showed positivity for CD68 and S-100 protein in the xanthomatous cells, and negativity for CD3, CD20, CD30, and CD1a (Figure 4B-E). Considering the clinical, histopathological and immunohistochemical features, the final diagnosis was RDD involving the right maxilla and the sinus. The peripheral blood count showed mild anemia, and normal leukocyte and platelet counts.
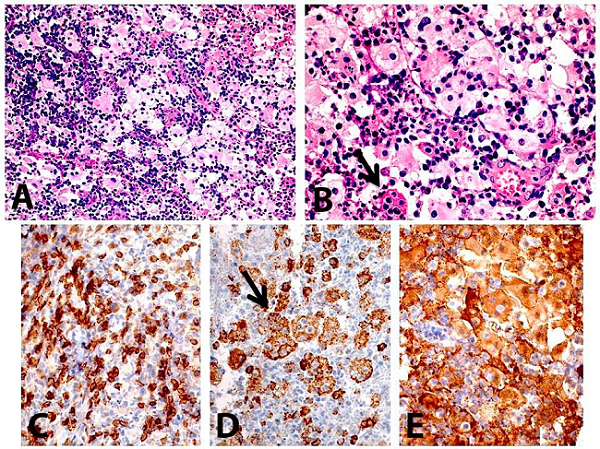
Figure 4
Photomicrography of the biopsy. A - A diffuse inflammatory infiltrate rich in xanthomatous macrophages (H&E 40X); B - Evident lymphocytes emperipolesis is also observed (arrow) (H&E 200X); C - CD3 positive for reactive cells (T lymphocyte cells); D - CD68 showed strong positivity for macrophages with lymphocytes emperipolesis (arrow); E - S-100 was positive in histiocytic cells.
The patient was referred to a hematologist who ruled out other sites involved trough of a bone scintigraphy and prescribed 40 mg daily of prednisone for 6 months duration, gradually tapering the dose up to a total of 10 months. Bone scintigraphy was undertaken and ruled out other sites of involvement of the skeleton. However, some teeth (right central incisor, right lateral incisor, right second pre-molar, right first molar, and right third molar) needed to be extracted due to their great mobility.
The disease showed no progression 15 months after the diagnosis, and the patient remained asymptomatic. After 5 years of treatment, the patient is still asymptomatic and follows a program of oral rehabilitation. The clinical and imaging examinations were steady (Figure 5).
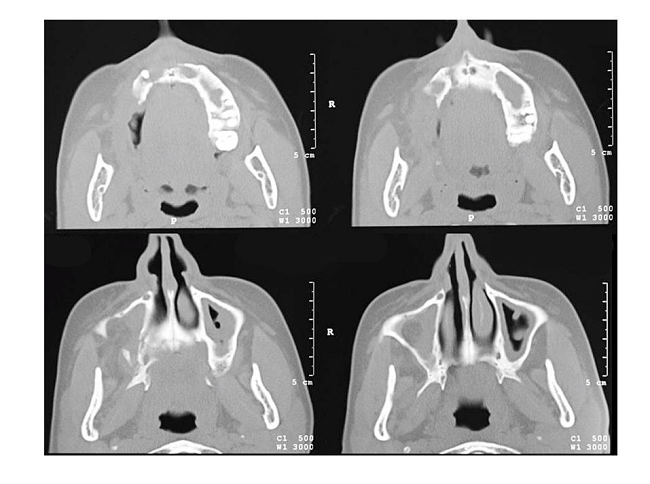
Figure 5
Axial CT images showing sinusopathy in both maxillary sinuses, and control of the bone reabsorption.
DISCUSSION
RDD is a rare disease of the hematopoietic system with approximately 1,000 cases reported in the English language literature as at 2012. The most common presentation is a painless cervical lymphadenopathy, but eventually the axillary and inguinal nodes become involved. Extranodal involvement is uncommon. However, skin, nasal cavity, and paranasal sinuses may be affected, along with systemic symptoms, such as fever, pain, weight loss, pharyngitis, and nasal obstruction. RDD can be found solely in the skeleton as isolated or multifocal osseous involvement. In the review by Foucar et al.,5 which involved 423 patients with RDD, 33 (7.8%) had osteolytic bone lesions and only 4 presented involvement of the jaw bones. Paranasal sinuses represent one of the two most common extranodal sites of RDD. Polyps or mass lesions are commonly observed, and approximately 70% of these patients show concomitant extranodal site involvement, which often involve the eyelid/orbit, skin, or oral cavity. Similarly, in our case, both paranasal sinuses and maxilla were affected, eventually representing extension of the same disease, and the main complaint of the patient was the pain.
Cardoso et al.6 reviewed the literature from 1969 to 2011 and found only eight cases of RDD affecting the maxillary bones (six females and two males, aged 18-56 years). In five of these patients, the maxilla was exclusively involved. In the present case, a 39-year-old woman referred intense pain in the region of the upper right maxilla. However, the pain was not associated with the teeth according to clinical, radiographic, and pulp vitality tests. X-ray and computed tomography showed an extensive osteolytic lesion involving the alveolar bone of the right maxilla, and bilateral sinusopathy. In addition, both the physical examination and the bone scintigraphy showed no other affected sites. RDD has nonspecific bone imaging findings that may be represented by ill-defined osteolytic or sclerotic lesions. Differential diagnosis of bone lesions includes LCH, metastatic tumor, osteomyelitis, lymphoma, and sarcoidosis.7-9
RDD etiology is uncertain; some studies suggested an inappropriate response of the immune system to the Epstein-Barr virus (EBV) and human herpes virus-6 infections. In fact, high levels of serum antibodies against EBV were found in patients with RDD.3,10 Other studies pointed out the association between RDD and LCH, or considered RDD as an unusual variant of LCH. Interestingly, synchronous or metachronous RDD and LCH were reported in 10 patients.11-13 Our patient had no systemic symptoms, except for a discrete anemia (hemoglobin 10.5g/dL [reference value: 12-14 mg/dL]).
The diagnosis of RDD was confirmed by histological and immunohistochemical studies. Macrophages exhibiting emperipolesis—expressing S-100 and CD1a-negative—can be considered almost pathognomonic for RDD.14 Such immunohistochemical characteristics were found in our case, which showed immunoreactivity for CD68, S-100, and CD3, and was negative for CD30 and CD1a. Furthermore, xanthomatous macrophages were also be observed.
There is no specific treatment for RDD. In a recent review dealing with a treatment strategy for RDD, 50% of patients did not require any treatment, while others received steroids, antibiotics, chemotherapy, radiation, surgery, and antifungal agents.15 According to Keskin et al.,8 surgery appears to be one of the most effective approaches in the treatment of RDD. However, corticosteroid therapy reduces the fever and the lymphadenopathy and is usually the treatment of choice for controlling the disease.15 In our case, corticotherapy was used in conjunction with a strict follow-up. The patient’s maxillary pain was controlled, but the mobility of all teeth of the right maxilla remained unchanged, which required the extraction of some of them. After a 5-year follow-up, the patient is well, and the disease is considered under control without any further treatment requirement.
RDD affecting the maxillary bone is extremely rare and requires a close follow-up by the dentist together with the medical team, as it can cause severe bone destruction, plus teeth mobility and loss. Conservative treatment should be considered in such cases, taking into account the possibility of a spontaneous remission.
REFERENCES
1 Thomson ER, Newman P, Dunstan S, Coull H. The Rosai Dorfman syndrome in a 50-year-old male. Br J Oral Maxillofac Surg. 1989;27(1):39-45. PMid:2920162 http://dx.doi.org/10.1016/0266-4356(89)90125-3.
2 Yontz L, Franco A, Sharma S, Lewis K, McDonough C. A case of Rosai-Dorfman disease in a pediatric patient with cardiac involvement. J Radiol Case Rep. 2012;6(1):1-8. PMid:22690274
3 Rosai J, Dorfman RF. Sinus histiocytosis with massive lymphadenopathy: a pseudolymphomatous benign disorder. Analysis of 34 Cases. Cancer. 1972;30(5):1174-88. PMid:5083057 http://dx.doi.org/10.1002/1097-0142(197211)30:5<1174::AID-CNCR2820300507>3.0.CO;2-S.
4 McAlister WH, Herman T, Dehner LP. Sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease). Pediatr Radiol. 1990;20(6):425-32. PMid:2202971 http://dx.doi.org/10.1007/BF02075199
5 Foucar E, Rosai J, Dorfman R. Sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease): review of the entity. Semin Diagn Pathol. 1990;7(1):19-73. PMid:2180012
6 Cardoso CL, Damante JH, Santos PSS, et al. Rosai-Dorfman disease with widespread oral-maxillofacial manifestations: a case report. J Oral Maxillofac Surg. 2012;70(11):2600-4. PMid:22330332 http://dx.doi.org/10.1016/j.joms.2011.12.015
7 Kademani D, Patel SG, Prasad ML, Huvos AG, Shah JP. Intraoral presentation of Rosai-Dorfman disease: a case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;93(6):699-704. PMid:12142877 http://dx.doi.org/10.1067/moe.2002.123495
8 Keskin A, Genç F, Günhan Ö. Rosai-Dorfman disease involving maxilla: a case report. J Oral Maxillofac Surg. 2007;65(12):2563-8. PMid:18022485 http://dx.doi.org/10.1016/j.joms.2006.10.003
9 Akyigit A, Akyol H, Sakallioglu O, Polat C, Keles E, Alatas O. Rosai-Dorfman disease originating from nasal septal mucosa. Case Rep Otolaryngol. 2015; 2015:1-3. http://dx.doi.org/10.1155/2015/232898
10 Levine PH, Jahan N, Murari P, Manak M, Jaffe ES. Detection of human herpesvirus 6 in tissues involved by sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease). J Infect Dis. 1992;166(2):291-5. PMid:1321861 http://dx.doi.org/10.1093/infdis/166.2.291
11 Wang KH, Cheng CJ, Hu CH, Leew WR. Coexistence of localized Langerhans cell histiocytosis and cutaneous Rosai-Dorfman disease. Br J Dermatol. 2002;147(4):770-4. PMid:12366428 http://dx.doi.org/10.1046/j.1365-2133.2002.04879.x.
12 O’Malley D, Duong A, Barry TS, et al. Co-occurrence of Langerhans cell histiocytosis and Rosai-Dorfman disease: possible relationship of two histiocytic disorders in rare cases. Mod Pathol. 2010;23(12):1616-23. PMid:20729813 http://dx.doi.org/10.1038/modpathol.2010.157
13 Kutty SA, Sreehari S. Co-occurrence of intracranial Rosai-Dorfman disease and Langerhans histiocytosis of the skull: case report and review of literature. Turk Neurosurg. 2015;25(3):496-9. PMid:26037195
14 Castillo BTD, Mata-Fernandez C, Soria VJR, Blanco VP, Loughlin G, Campos-Domínguez M. Self-healing extranodal cutaneous Rosai-Dorfman in a child. Pediatr Dermatol. 2015;32(6):e249-59. PMid:26391332 http://dx.doi.org/10.1111/pde.12676
15 Pulsoni A, Anghel G, Falcucci P, et al. Treatment of sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease): report of a case and literature review. Am J Hematol. 2002;69(1):67-71. PMid:11835335 http://dx.doi.org/10.1002/ajh.10008
Notes
Author notes
Correspondence Fabio Abreu Alves Stomatology Department - AC Camargo Cancer Center R. Prof. Antônio Prudente, 211 - Sao Paulo/SP - Brazil CEP: 01509-010 Phone +55 (11) 2189-5129 Fax +55 (11) 2189-5133 falves@accamargo.org.br
Conflict of interest declaration