Image in Focus
Eisenmenger syndrome
Eisenmenger syndrome
Autopsy and Case Reports, vol. 7, no. 1, pp. 5-7, 2017
Hospital Universitário da Universidade de São Paulo
Keywords: Hypertension, Pulmonary, Heart Septal Defects, Atrial, Heart Failure
Eisenmenger syndrome (ES) stands for pulmonary hypertension, reversal of the central shunt’s flow, and cyanosis secondary to any congenital heart defect (CHD) associated with non-repaired intra- or extra-cardiac communication.1 In this syndrome, the original central left-to-right shunt reverses the direction to right-to-left due to long-standing pulmonary hypertension and high pulmonary vascular resistance turning to systemic or supra-systemic levels, and due to structural obstructive pulmonary vascular disease.
In 1897, the Austrian doctor, Victor Eisenmenger (1864-1932), firstly described this syndrome in the article entitled “The congenital ventricular septal defects of the heart” published in the German medical journal Zeitschrifft für Klinische Medizin,2 reporting the case of a 32-year-old man with clubbing fingers, cyanosis since infancy, the presence of a systolic murmur and a pronounced second heart sound. Over the patient’s last 3 years of life, he began presenting dyspnea, which evolved to heart failure, and he died due to a massive hemoptysis. At the autopsy, pulmonary hemorrhage was confirmed along with a ventricular septal defect, a right ventricular hypertrophy accompanied by an overriding aorta and atheromatosis of the major pulmonary arteries. In the years since Eisenmenger’s descriptions were published, they were better understood and became appropriate to the practice of cardiology. The name of Doctor Eisenmenger is eponymously attached to this entity. However, at the time the first case was reported, neither pulmonary hypertension nor pulmonary arteriolar disease were known.3,4 The pulmonary hypertension and the increase in the pulmonary vascular resistance associated with ES were not described until the 1950s.
The chronic pulmonary overflow and the transmission of high systemic pressure to the pulmonary circulation secondary to the central left-to-right shunt induced, over time, the pulmonary vascular change characterized by the decrease of the overall cross-sectional area of the pulmonary arteriolar bed. This pulmonary vascular physical injury may cause mechanical stretch and intimal tears accompanied by histological changes with increased intrinsic elastase production and vascular endothelial growth factors, which will further give rise to intimal hyperplasia and medial hypertrophy of peripheral pulmonary arteries. Moreover, endothelial dysfunction, platelet activation, and increased thromboxane and endothelin levels will cause obstructive pulmonary lesions and pulmonary hypertension.5-8 Eventually, typical atherosclerotic lesions develop in the pulmonary arteries. However, the pulmonary resistance will show clinical significance only when two-thirds of the pulmonary vascular bed is compromised.9 At this point, those patients who still do not present oxygen desaturation become cyanotic, signaling the reversal of the central shunt. The progressive hypoxemia and central cyanosis of the adult patient with ES will result in reduced quality of life and premature death due to multi-systemic abnormalities, such as coagulation disorders, heart failure, renal insufficiency, and hypertrophic osteoarthropathy.9
Factors influencing the development of advanced pulmonary vasculopathy in subjects with atrial septal defect have not been completely explored. In adults, the general belief (though not proved) is that long exposure to altered flow conditions, which is largely dependent on right ventricular compliance, could alter pulmonary vascular cell biology via shear and stretch forces. However, ES features may be present in young adults with pre-tricuspid defects. Furthermore, advanced pulmonary vascular disease may be seen in young infants with no previous features of pulmonary overcirculation.10
Thus, the development of ES depends on the heart defect, its size and location (higher prevalence in post-tricuspid defects), and to factors that remain to be determined.9
The population of adults with congenital heart disease (known under the acronym of GUCH: grown-up congenital heart disease) is growing at an acceleration rate of 5% per year. In the USA, more than 1 million adults have CHD. 10% of the cases present pulmonary hypertension, 30% of them due to unrepaired defects. ES will develop in half of these patients with unrepaired cardiovascular defects.11 Although less frequent, large atrial septal defects will cause pulmonary hypertension during the second or third decade of life. These patients present a long asymptomatic period with an adjusted lower exercise capacity until adolescence or early adulthood. Gradually, exercise intolerance, cyanosis, exertion dyspnea, syncope, chest pain, heart failure, hyperviscosity syndrome (secondary to erythrocytosis), and rhythm disturbances (particularly atrial fibrillation) supervene.9 Hemoptysis is a common presentation of ES, which can be due to pulmonary embolism and infarction, rupture of the dilated pulmonary artery or thin pulmonary arteriole, coagulation disturbances, or thrombocytopenia. Although long-term survival has been reported, patients with ES usually die between 30 and 35 years old.1
Physical examination of a patient with ES will show cyanosis, clubbing fingers, and parasternal lift from right ventricle hypertrophy. Plus, a tactual closure of the pulmonary valve may be felt. In the case of ES due to atrial septal defect, the widely and fixed split of the S2 is invariably present, and a tricuspid regurgitation murmur may be audible. There will be signs of right heart failure as hepatomegaly, and a third heart sound may be present.
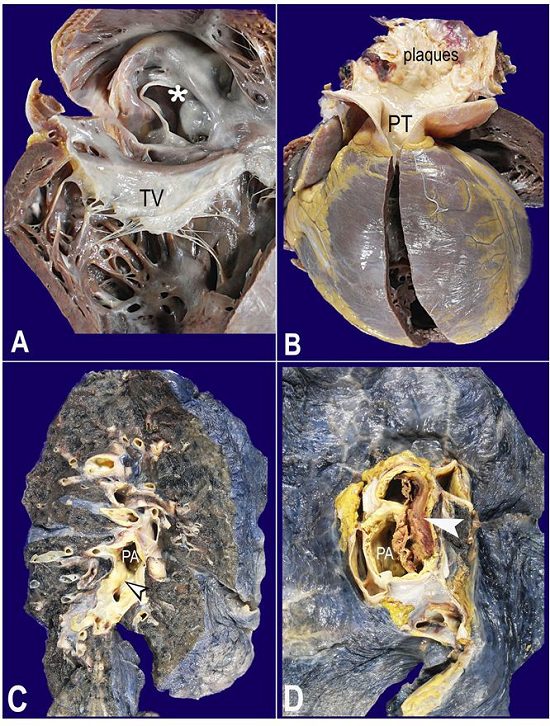
The Figure shows macroscopic lesions typical of ES, from a 56-year-old male patient with a non-repaired atrial septal defect. Right ventricle dilation and large atrial septal defect measuring 3.5 × 3.0 cm can be seen, as well as a prominent right ventricle, dilation and severe atherosclerosis of the pulmonary artery, prominent dilation and atherosclerosis of the right pulmonary artery and parenchymal branches, and partial thrombosis of the right pulmonary artery.
Figure
A and B - Gross examination of the heart. A - Opened right cardiac chambers. The asterisk marks the atrial septal defect located at the fossa ovalis (so-called secundum defect); B - The right ventricle hypertrophy and pulmonary artery trunk (PT) dilation with atherosclerotic plaques; C and D - Macroscopic findings of the lungs; C - The dilation and atherosclerosis of the pulmonary artery (PA) (arrowhead points to a plaque) and its branches; D - PA thrombosis (white arrowhead). TV = tricuspid valve.
Pictures courtesy of Dr. Luiz Alberto Benvenuti
ACKNOWLEDGEMENTS
The authors are very grateful to Dr. Vera Demarchi Aiello and Dr. Antônio Augusto Barbosa Lopes for the evaluation and supplementation of this manuscript.
REFERENCES
1 Wood P. The Eisenmenger syndrome or pulmonary hypertension with reversed central shunt. BMJ. 1958;2(5099):755-62. PMid:13572894 http://dx.doi.org/10.1136/bmj.2.5099.755
2 Eisenmenger V. Die angeborenenDefecte derKammerscheidewand des Herzens. Zeitschrifft für Klinische Medizin. 1897;32(Suppl.):1-28.
3 Duke M. Victor Eisenmenger (1864-1932): the man behind the syndrome. J Med Biogr. 2017;25(1):52-5. PMid:25745871
4 Partin C. The evolution of Eisenmenger’seponymic enshrinement. Am J Cardiol. 2003;92(10):1187-91. PMid:14666927 http://dx.doi.org/10.1016/j.amjcard.2003.07.028
5 Celermajer DS, Cullen S, Deanfield JE. Impairment of endothelium-dependent pulmonary artery relaxation in children with congenital heart disease and abnormal pulmonary hemodynamics. Circulation. 1993;87(2):440-6. PMid:8425291 http://dx.doi.org/10.1161/01.CIR.87.2.440
6 Rabinovitch M. Elastase and the pathobiology of unexplained pulmonary hypertension. Chest. 1998;114(3, Suppl):213S-24S. PMid:9741572 http://dx.doi.org/10.1378/chest.114.3_Supplement.213S.
7 Yoshibayashi M, Nishioka K, Nakao K, et al. Plasma endothelin concentrations in patients with pulmonary hypertension associated with congenital heart defects. Evidence for increased production of endothelin in pulmonary circulation. Circulation. 1991;84(6):2280-5. PMid:1959183 http://dx.doi.org/10.1161/01.CIR.84.6.2280
8 Fuse S, Kamiya T. Plasma thromboxane B2 concentration in pulmonary hypertension associated with congenital heart disease. Circulation. 1994;90(6):2952-5. PMid:7994842 http://dx.doi.org/10.1161/01.CIR.90.6.2952
9 Kaemmerer H, Mebus S, Schulze-Neick I, et al. The adult patient with Eisenmenger Syndrome: a medical Update after Dana Point Part I: epidemiology, clinical aspects and diagnostic options. Curr Cardiol Rev. 2010;6(4):343-55. PMid:22043211 http://dx.doi.org/10.2174/157340310793566154
10 Lopes AA, Mesquita SM. Atrial septal defect in adults: does repair always mean cure? Arq Bras Cardiol. 2014;103(6):446-8. PMid:25590922
11 Roth TS, Aboulhosn JA. Pulmonary hypertension and congenital heart disease. Cardiol Clin. 2016;34(3):391-400. PMid:27443136 http://dx.doi.org/10.1016/j.ccl.2016.04.002
Notes
Author notes
Correspondence Fernando Peixoto Ferraz de Campos Internal Medicine Division - Hospital Universitário - Universidade de São Paulo Avenida Professor Lineu Prestes, 2565 - São Paulo/SP - Brazil CEP: 05508-000 Phone: +55 (11) 3091-9275 fpfcampos@gmail.com
Conflict of interest declaration