Article / Autopsy Case Report
Disseminated invasive aspergillosis in a prolonged stay in the intensive care unit
Disseminated invasive aspergillosis in a prolonged stay in the intensive care unit
Autopsy and Case Reports, vol. 7, no. 1, pp. 17-21, 2017
Hospital Universitário da Universidade de São Paulo
Received: 19 July 2016
Accepted: 03 February 2017
ABSTRACT: Aspergillus is a common cause of invasive mycosis, especially in immunocompromised individuals. We report the case of a 62-year-old male who was hospitalized after suffering severe physical injuries and died after few weeks of hospitalization. A medicolegal autopsy was conducted, and various organs were sent for histopathological examination of which heart, lungs, and kidneys showed extensive involvement by aspergillus. Thus, a diagnosis of disseminated invasive aspergillosis was made on autopsy, which itself is a rare entity. This case report illustrates a prolonged stay in the intensive care unit as a possible risk factor for the development of disseminated aspergillosis.
Keywords: Aspergillosis, Intensive Care Units, Multiple Trauma, Respiration, Artificial, Autopsy.
INTRODUCTION
Systemic mycosis is a rare disease that usually affects immunosuppressed patients. The incidence of systemic mycosis at postmortem in various studies varies from 0.98% to 10.4%.1 The prolonged use of antibiotics, immunosuppressive agents, and parenteral nutrition may act as contributing factors to the increased incidence of fungemia.2 Aspergillosis is a common cause of invasive mycosis and its incidence has risen following organ transplantation, chemotherapy, and other causes of immunosuppression.3 Aspergillosis is caused by Aspergillus fumigatum, A. flavus, and more rarely A. terreus, A. nidulans, and A. niger. The most common portal of entry of the organism is the respiratory system. A. fumigatum is the most prevalent fungal pathogen responsible for fatal invasive aspergillosis. It may also present as a primary cutaneous lesion in immunocompetent patients, although this is rare.1
CASE REPORT
A 62-year-old male was hospitalized after suffering severe physical injuries in an argument with the neighbors. The patient was diagnosed with multiple fractures including a fracture in the right clavicle and second, third, and fourth ribs of the right chest wall. There was no past medical history of diabetes mellitus, hypertension, tuberculosis, or any chronic illness. No history of immunosuppressive therapy or steroid intake was evident. The patient was in severe respiratory distress at the time of admission, and an emergency tracheostomy was done. He was prescribed broad-spectrum antibiotics and parenteral nutrition, but there was no improvement in his medical condition, which later required mechanical ventilation. He died after 3 weeks of hospitalization, and a medicolegal autopsy was conducted to ascertain the cause of death. Heart, both lungs, and pieces of liver, spleen, and kidneys were sent for histopathological examination to determine the cause of death.
On gross examination, the heart weighed 350 g and measured 14 × 10 × 4 cm. On cut section, multiple gray-yellow plaques were seen in the left ventricular wall, the interventricular septum, and the apex regions (Figure 1A). The lungs weighed 850 g (right lung) and 660 g (left lung) and measured 18 × 16 × 12 cm and 17 × 16 × 13 cm, respectively. The cut surface of both lungs showed multiple gray-white necrotic areas (Figure 1B). The liver and spleen were grossly unremarkable. The kidneys weighed 150 g (right kidney) and 130 g (left kidney) and measured 10 × 5 × 2 cm and 9 × 5 × 2 cm; the cut surface showed grey-yellow necrotic areas (Figure 2).
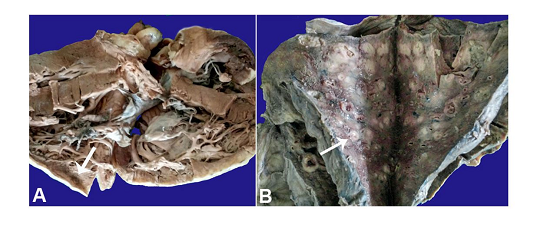
Figure 1
A - Gross specimen of the heart showing the grey-white area in the region of the interventricular septum and the right ventricular wall; B - Gross specimen of the lung showing multiple friable grey-white necrotic areas on the cut section.
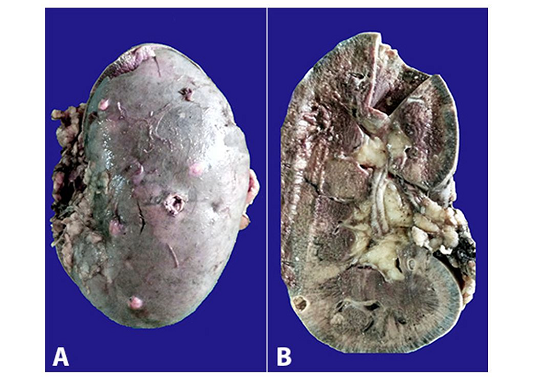
Figure 2
Gross examination of the kidney. A - Multiple nodular and cavitary lesions on the external surface; B - A cystic lesion on the cut surface.
Representative microsections examined from the left ventricular wall, the interventricular septum, and the apex of the heart showed infiltration by acute inflammatory infiltrate with focal areas of necrosis and the presence of branching septate hyphae with morphology resembling Aspergillus spp. Periodic acid-Schiff (PAS) and Gomori methenamine silver (GMS) stain of the fungus demonstrated the distinct dichotomous acute angle branching of septate hyphae with the orientation of the branches in a similar direction (Figure 3).
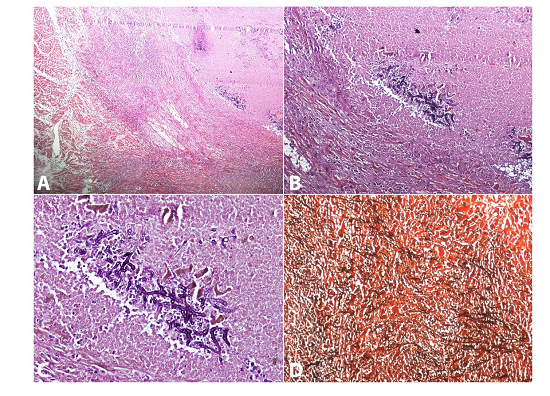
Figure 3
Photomicrophotographs of the heart, which reveal the destruction of cardiomyocytes intermingled with necrotic debris and fungal hyphae (A - H&E, 40X). The fungal hyphae were septate with acute angle branching, PAS positive (B - PAS, 100X & C - PAS, 400X) and GMS positive (D - GMS, 100X).
Representative microsections examined from lung specimens and kidney showed extensive multifocal areas of necrosis with acute and chronic inflammatory infiltrate, a few giant cells, and the presence of fungal hyphae with a morphology similar to Aspergillus spp. These fungal hyphae were again demonstrated with the help of PAS and GMS stains (Figure 4). Microsections examined from the liver and spleen were unremarkable. Thus, the post-mortem diagnosis was disseminated invasive aspergillosis.
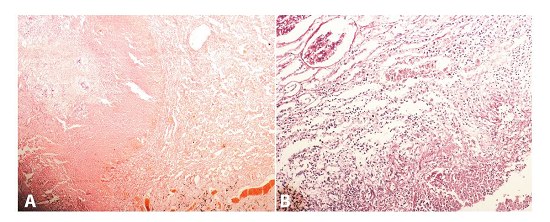
Figure 4
Photomicrophotographs of the lung (A - H&E, 100X) and kidney (B - PAS, 400X) revealing the presence of similar fungal hyphae.
DISCUSSION
Aspergillus is a ubiquitous mold. Although exposure to this pathogen is universal, the disease is quite uncommon. Host factors play a major role in determining the outcome following exposure. The main predisposing factors for fungal infection are debilitating disease, a continuity solution of the skin or mucous membranes providing a portal of entry and disturbance in the saprophyte-host relationship by immunosuppressive agents or antibiotics. The patients may have one or all of these predisposing conditions.2
Invasive aspergillosis has become an important cause of morbidity and mortality in immunocompromised or immunosuppressed patients. Common predisposing conditions for Aspergillus infection include neutropenia, prolonged antibiotic therapy, steroid therapy, AIDS, hematological malignancies, organ transplantation, cytotoxic therapy, diabetes mellitus, alcohol abuse, renal failure, hepatic failure, or any chronic debilitating disease. A prolonged stay in an intensive care unit with mechanical ventilation has also been implicated in the causation of invasive Aspergillus infection and was one of the predisposing factors in this case study.3 Recently, with an increase in the incidence of immunosuppressed patients, Aspergillus became the most common pathogenic mold worldwide. The average incidence of invasive aspergillosis on autopsy is around 0.19%. It is increasingly being reported in AIDS patients (1-12%) and as a common complication of chronic granulomatous disease (25-40%).1
Although fungus can colonize any organ, the lungs are the most commonly affected site. Inhalation of fungal spores is the main portal of entry to cause pulmonary infection. Common presenting symptoms of invasive aspergillosis are non-specific and include fever, cough, chest pain, dyspnea, malaise, and weight loss. Invasive pulmonary aspergillosis has several clinicopathological forms, including acute bronchopneumonia, angioinvasive aspergillosis, acute tracheobronchitis, miliary aspergillosis, and pleural aspergillosis.3 Apart from the pulmonary system, aspergillosis may present in other organs, including brain, heart, liver, spleen, kidney, thyroid gland, and lymph nodes.4
Disseminated aspergillosis may involve every organ in the body. As disseminated aspergillosis is a devastating disease, thorough clinical examination, laboratory and radiological investigations are required for early diagnosis and management. A high index of suspicion is required, especially in immunosuppressed individuals.3 Culture or microscopic examination of sputum or bronchoalveolar lavage specimens can be used to demonstrate colonization of the airways. Fine-needle aspiration cytology or biopsy can be done to demonstrate fungal hyphae followed by special stains, such as PAS and GMS, to aid in determining fungal morphology. Enzyme-linked immunosorbent assay (ELISA) is also a useful and specific test for the diagnosis of allergic bronchoalveolar aspergillosis.1 Radiographic investigations, such as the chest x-ray and computed tomography (CT) scan are helpful in the diagnosis of primary pulmonary infection. Thoracic CT scans are more sensitive than chest x-rays in detecting pulmonary lesions compatible with the diagnosis of aspergillosis. Aspergillus flavus-specific DNA in brain biopsy and serum specimens may be used to diagnose a case of cerebral aspergillosis.4
CONCLUSION
Disseminated aspergillosis is a devastating disease with multi-organ involvement and a high rate of mortality. Even with early diagnosis, the disease is difficult to treat due to extensive pulmonary and extra pulmonary involvement. Since the manifestations vary according to the host’s immune status and underlying lung disease, the clinical and radiographic features may vary. A vigorous and careful demonstration of fungi in highly suspicious cases, followed by empirical treatment, forms the mainstay of the management of disseminated aspergillosis.
REFERENCES
1 Aleksenko A, Gyasi RK, Gyasi RK. Disseminated invasive aspergillosis. Ghana Med J. 2006;40(2):69-72. PMid:17299570 http://dx.doi.org/10.4314/gmj.v40i2.36021
2 Cishek MB, Yost B, Schaefer S. Cardiac aspergillosis presenting as myocardial infarction. Clin Cardiol. 1996;19(10):824-7. PMid:8896916 http://dx.doi.org/10.1002/clc.4960191012
3 Vaideeswar P, Prasad S, Deshpande JR, Pandit SP. Invasive pulmonary aspergillosis: a study of 39 cases at autopsy. J Postgrad Med. 2004;50(1):21-6. PMid:15047994
4 Feng D, Heffner R, Wright J. Invasive aspergillosis extensively involving the brain and multiple organs in a bone marrow transplant patient. The Internet Journal of Pathology. 2007;7:1-7.
Notes
Author notes
Correspondence Sonu Kalyan Department of Pathology - Pandit Bhagwat Dayal Sharma Post Graduate Institute of Medical Sciences Dr. Sonu Kalyan, Room No-66, Girls hostel, PGIMS - Rohtak, 124001 - India Phone: +91 8397006757 dockalyan23@gmail.com
Conflict of interest declaration