Article / Clinical Case Report
Mandible metastasis of small cell lung cancer mimicking a residual cyst
Mandible metastasis of small cell lung cancer mimicking a residual cyst
Autopsy and Case Reports, vol. 7, no. 1, pp. 37-41, 2017
Hospital Universitário da Universidade de São Paulo
Received: 27 November 2016
Accepted: 19 January 2017
ABSTRACT: Small cell lung carcinoma (SCLC) is an uncommon tumor characterized by an aggressive behavior with early metastasis, usually to the contralateral lung, liver, brain, and bones. There are only five cases of this particular tumor metastasizing to the oral cavity described in the English literature. We present the case of metastatic SCLC in the mandible with radiographic findings resembling a residual cyst. A 66-year-old man with previous diagnosis and treatment for a SCLC was referred to the Stomatology Department with a history of persistent pain in the mandible 1 year after the inferior right pre-molar tooth extraction. The radiographic exam showed a well-delimited radiolucent area on that extracted tooth’s region resembling a residual cyst. Biopsy was performed yielding the diagnosis of metastatic SCLC. The patient was referred to the clinical oncologist for chemotherapy. Although uncommon, this tumor should be included in the differential diagnosis of jawbone lesions, particularly when the patient presents a previous diagnosis of SCLC.
Keywords: Neoplasm Metastasis, Diagnosis, Oral, Small Cell Lung Carcinoma.
INTRODUCTION
Metastases to the oral cavity is uncommon, representing nearly 1% of all oral cavity malignancies, and are associated with bad prognosis, with the survival time ranging between 3.7 months to 8.25 months.1-4 Generally, the jaw is more commonly involved than the oral cavity’s soft tissues.2 Breast, lung, kidney, bone, and colon malignancy are most commonly related to oral metastasis, in that this descending order.5 In men, oral metastases derive most commonly from lung cancer. Non-small-cell lung cancer (NSCLC) accounts for 10-20% of all oral metastatic tumors, while oral metastases from (SCLC) are rarely reported in the English literature.6-9 Herein, we present an uncommon case of metastatic SCLC to the mandible, which was initially interpreted as a residual cyst due to its clinical and imaging characteristics.
CASE REPORT
A 66-year-old man was referred to the Stomatology Department complaining of pain in the right mandible over the past year. He reported the exodontia of the first inferior right premolar 1 year ago, which after 4 months, became the site of the current complaint. His medical history included the diagnosis of metastatic prostate adenocarcinoma being treated with goserelin acetate (Zoladex®) over the last 8 years. An SCLC and bone metastasis from the prostate adenocarcinoma were also diagnosed in the past year, and treated with cisplatin (CCDP) and zoledronic acid (Zometa®). Intraoral examination revealed a slightly bluish area located in the overlying mucosa of the edentulous alveolus of the right mandible (first premolar). X-ray revealed a unilocular, oval radiolucency of 0.5 × 0.7 cm with well-defined sclerotic borders (Figure 1).
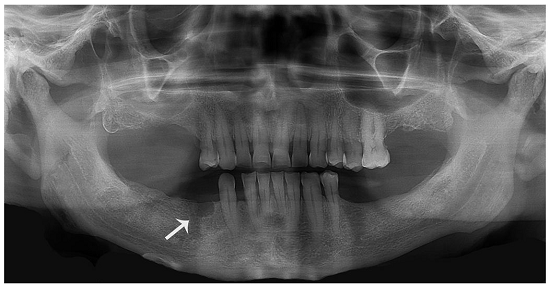
Figure 1
Initial panoramic radiograph showing a radiolucent oval image with radiopaque halo in the premolar region (arrow).
According to clinical and imaging findings, the main diagnostic hypothesis was a residual cyst. A surgical procedure was proposed and during surgery the solid macroscopic characteristics of the lesion corresponded to the cystic radiographic aspect. The histopathologic examination revealed remarkably basophilic irregular cells with scant cytoplasm and hyperchromatic nuclei exhibiting scattered crushing artifacts (Figure 2A, 2B and 2C). The immunohistochemical study revealed positivity for citokeratin 7, chromogranin A, and TTF-1 (Figure 2D, 3A and 3B respectively) rendering the diagnosis of metastatic SCLC.
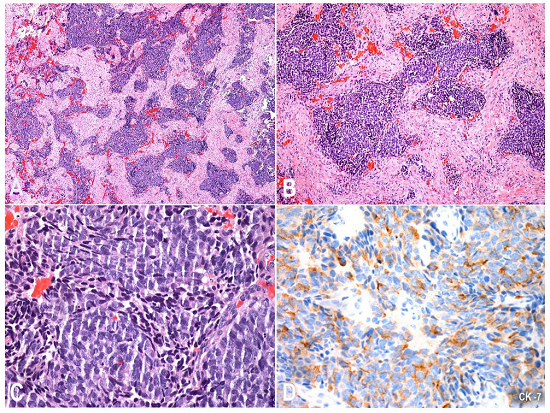
Figure 2
Photomicrography of the biopsy specimen showing in A and B - an infiltrative tumor composed of large cell blocks with irregular shapes and marked basophilia (H&E, 40X and 100X, respectively); C - Note that the cells had scant cytoplasm and hyperchromatic nuclei, some with crushing artifact (H&E, 400X). The immunohistochemical study showed in D positivity for cytokeratin 7 (200X).
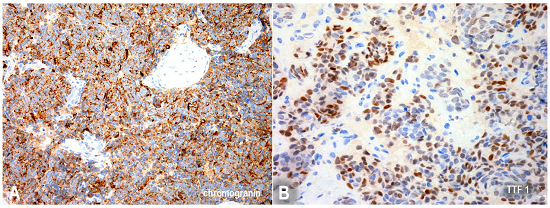
Figure 3
Photomicrography of the biopsy specimen showing in A positivity for chromogranin A (200X), and in B positivity for TTF-1 (200X).
The patient was referred to the Clinical Oncology Department and underwent chemotherapy with paclitaxel 60 mg/m2. After a 4-month follow-up, the patient was asymptomatic and the x-ray showed signs of bone neoformation (Figure 4).

Figure 4
Panoramic radiograph 1 month after chemotherapy, showing new bone formation in the previously metastatic region.
DISCUSSION
Lung cancer classification comprises two large groups: the NSCLC and the SCLC. NSCLC accounts for up to 80% of all lung cancers comprising adenocarcinoma, squamous cell carcinoma, and large cell carcinoma.10 On the other hand, the SCLC, which is of neuroendocrine origin, represents the remaining 20% of all lung cancer cases,11 has an aggressive behavior, and is strongly associated with cigarette smoking. The SCLC frequently (60-65%) metastasize in the early stages of the disease.12,13 However, as far as we know, to date, there are only five reported cases of metastatic SCLC to the oral cavity.6-9 The case presented herein showed an unusual SCLC metastasis to the mandible, which was initially misinterpreted as a residual cyst.
Hirshberg et al.2 reported 673 cases of metastatic oral tumors from 1916 to 2006, 112 cases (16.6%) of which originated in the lung and 58 (8.6%) cases were found in the jaw. This study showed a male predominance with a mean age of 52 years.2 Smaller series endorsed Hishberg et al.’s observation.1,3,7,14-20 However, most of these studies did not specify the lung cancer phenotype. Kim et al.6 reported one case of metastatic SCLC in a 60-year-old male patient presenting as a pedunculated and granular lesion on the right side of the tongue. Pektas and Gunhan8 reported the case of a 50-year-old woman with an erythematous, hemorrhagic soft tissue mass on the left mandibular gingiva. Lim et al.7 conducted a retrospective analysis of 41 Korean patients diagnosed with metastatic oral tumors and the lung was the second most common primary site (n = 9: 22%) with adenocarcinoma as the most common histologic variant, with only two cases of SCLC. The authors did not specify their clinical presentation.7 In a recent study with 44 patients with metastatic solid tumors to the oral cavity, Owosho et al.9 reported one patient with SCLC presenting a non-healing tooth infection as the clinical presentation of oral metastasis.
The clinical features of metastatic lesions differ depending on the involved site in the oral cavity. In the jawbones, most patients complain of swelling, pain, paresthesia and numbness. Usually, a rapid growing exophytic mass, particularly in the molar region, is observed, as well as misleading presentations such as toothache, dentoalveolar swelling, and loose teeth.1,3,7,14-20 In contrast to the reported cases of SCLC, which were clinically expressed as masses6,8 or dental infections,9 our case was characterized by an altered staining of the mucosa, which appeared bluish, and associated with pain. In agreement with the literature, the accurate diagnosis of oral metastasis may become difficult and challenging because of the unspecific characteristics of such lesions.2,8,16,17,20
Radiographically, most cases of metastatic lesions present as osteolytic areas poorly defined with a “moth eaten” appearance.2 The imaging study of our patient was quite different presenting a well-defined margin of the lesion. Consequently, the hypothesis of metastatic SCLC of the mandible was not initially taken into account. Based on the clinical/radiograph findings and previous history of the first premolar’s exodontia, the lesion was initially considered as an odontogenic lesion.
In this case, we emphasize the different forms of clinical and imaging presentation of oral metastases eventually mimicking benign lesions. Thus, it is important to add metastatic lesions in jawbone lesions as a differential diagnosis, especially when the patient has a previous history of cancer.
REFERENCES
1 Van der Wall RIF, Buter J, Van der Waal I. Oral metastases: report of 24 cases. Br J Oral Maxillofac Surg. 2003;41(1):3-6. PMid:12576032 http://dx.doi.org/10.1016/S0266-4356(02)00301-7.
2 Hirshberg A, Shnaiderman-Shapiro A, Kaplan I, Berger R. Metastatic tumours to the oral cavity- Pathogenesis and analysis of 673 cases. Oral Oncol. 2008;44(8):743-52. PMid:18061527 http://dx.doi.org/10.1016/j.oraloncology.2007.09.012
3 Murillo J, Bagan JV, Hens E, Diaz JM, Leopoldo M. Tumors metastasizing to the oral cavity: a study of 16 cases. J Oral Maxillofac Surg. 2013;71(9):1545-51. PMid:23800673 http://dx.doi.org/10.1016/j.joms.2013.03.017
4 Allon I, Pessing A, Kaplan I, Allon DM, Hirshberg A. Metastatic tumors to the gingiva and the presence of teeth as a contributing factor: a literature analysis. J Periodontol. 2014;85(1):132-9. PMid:23646853 http://dx.doi.org/10.1902/jop.2013.130118
5 Schneider KM, Martinez AY, Guglielmi M. Large cell neuroendocrine carcinoma: topic review and a unique case of metastasis to the mandible. J Maxillofac Oral Surg. 2015;14(1, Suppl 1):120-6. PMid:25861184 http://dx.doi.org/10.1007/s12663-012-0362-x
6 Kim RY, Perry SR, Levy DS. Metastatic carcinoma to the tongue: a report of two cases and a review of the literature. Cancer. 1979;43(1):386-9. PMid:216477 http://dx.doi.org/10.1002/1097-0142(197901)43:1<386::AID-CNCR2820430154>3.0.CO;2-G.
7 Lim SY, Kim SA, Ahn SG, et al. Metastatic tumours to the jaws and oral soft tissues: a retrospective analysis of 41 Korean patients. Int J Oral Maxillofac Surg. 2006;35(5):412-5. PMid:16473498 http://dx.doi.org/10.1016/j.ijom.2005.12.001
8 Pektas ZO, Gunhan O. Cytologically diagnosed metastatic small cell lung carcinoma in the mandibular soft tissue. Saudi Med J. 2013;34(5):539-41. PMid:23677273
9 Owosho AA, Xu B, Kadempour A, et al. Metastatic solid tumors to the jaw and oral soft tissue: a retrospective clinical analysis of 44 patients from a single institution. J Craniomaxillofac Surg. 2016;44(8):1047-53. PMid:27270028 http://dx.doi.org/10.1016/j.jcms.2016.05.013
10 Kamangar F, Dores GM, Anderson WF. Patterns of cancer incidence, mortality, and prevalence across five continents: defining priorities to reduce cancer disparities in different geographic regions of the world. J Clin Oncol. 2006;24(14):2137-50. PMid:16682732 http://dx.doi.org/10.1200/JCO.2005.05.2308
11 Van Meerbeeck JP, Fennell DA, De Ruysscher DKM. Small cell lung cancer. Lancet. 2011;378(9804):1741-55. PMid:21565397 http://dx.doi.org/10.1016/S0140-6736(11)60165-7.
12 Kato Y, Ferguson TB, Bennett DE, Burford TH. Oat cell carcinoma of the lung: a review of 138 cases. Cancer. 1969;23(3):517-24. PMid:5766496 http://dx.doi.org/10.1002/1097-0142(196903)23:3<517::AID-CNCR2820230301>3.0.CO;2-L.
13 Jackman DM, Johnson BE. Small-cell lung cancer. Lancet. 2005;366(9494):1385-96. PMid:16226617 http://dx.doi.org/10.1016/S0140-6736(05)67569-1.
14 Bodner L, Sion-Vardy N, Geffen DB, Nash M. Metastatic tumors to the jaws: a report of eight new cases. Med Oral Patol Oral Cir Bucal. 2006;11(2):E132-5. PMid:16505790
15 Hirshberg A, Leibovich P, Buchner A. Metastatic tumors to the jawbones: analysis of 390 cases. J Oral Pathol Med. 1994;23(8):337-41. PMid:7815371 http://dx.doi.org/10.1111/j.1600-0714.1994.tb00072.x.
16 Seoane J, Van der Waal I, Van der Waal RI, et al. Metastatic tumours to the oral cavity: a survival study with a special focus on gingival metastases. J Clin Periodontol. 2009;36(6):488-92. PMid:19508248 http://dx.doi.org/10.1111/j.1600-051X.2009.01407.x.
17 Shen ML, Kang J, Wen YL, et al. Metastatic tumors to the oral and maxillofacial region: a retrospective study of 19 cases in West China and review of the Chinese and English literature. J Oral Maxillofac Surg. 2009;67(4):718-37. PMid:19304027 http://dx.doi.org/10.1016/j.joms.2008.06.032
18 Siriwardena BSMS, Jayasooriya PR. Palitha Ratnayake, Tilakaratne WM. Metastatic tumours of the oral and maxillofacial region: a retrospective analysis of 18 cases. Merit Res J Biochem Bioinform. 2013;1(1):1-4.
19 Nawale KK, Vyas M, Kane S, Patil A. Metastatic tumors in the jaw bones: a retrospective clinicopathological study of 12 cases at Tertiary Cancer Center. J Oral Maxillofac Pathol. 2016;20(2):252-5. PMid:27601818 http://dx.doi.org/10.4103/0973-029X.185920
20 Maschino F, Guillet J, Curien R, Dolivet G, Bravetti P. Oral metastasis: a report of 23 cases. Int J Oral Maxillofac Surg. 2013;42(2):164-8. PMid:23196066 http://dx.doi.org/10.1016/j.ijom.2012.10.029
Notes
Author notes
Correspondence Graziella Chagas Jaguar Stomatology Department - A.C. Camargo Cancer Center Rua Prof. Antônio Prudente, 211 - Liberdade - São Paulo/SP - Brazil CEP: 01509-900 Phone: +55 (11) 2189-5129 graziaju@yahoo.com.br
Conflict of interest declaration