Article / Clinical Case Report
Reconstruction of the skull inverting the deformed surface of the bone after exeresis of a frontal arachnoid cyst
Reconstruction of the skull inverting the deformed surface of the bone after exeresis of a frontal arachnoid cyst
Autopsy and Case Reports, vol. 7, no. 2, pp. 69-73, 2017
Hospital Universitário da Universidade de São Paulo
Received: 23 February 2017
Accepted: 15 May 2017
ABSTRACT: Intracranial arachnoid cysts need to be operated on when they are causing symptoms and aesthetic problems. The aim of this case report was to describe a new method of reconstructing the skull by eliminating a left frontal bone deformity by turning the inside out and the outside inward, which provided good aesthetics and protected the region of surgical interest after the removal of an arachnoid cyst of the left frontal lobe.
Keywords: Arachnoid Cysts, Tomography, X-Ray Computed, Intracranial Pressure.
INTRODUCTION
Intracranial arachnoid cysts are bulging spaces containing cerebrospinal fluid inside the membranes, which originate by the splinting or duplication of the arachnoid layer.1 They frequently occur at the supratentorial compartment and are usually benign, but they may cause signs and symptoms, such as migraine, seizures, intracranial hypertension, cerebral compression, bone protrusion, and erosion. When aesthetic problems occur, or some or all of these symptoms are evident, the cyst needs to be operated on.2
The repair of the skull bone can be challenging, depending on several factors such as anatomy of the region, the kind of defect or deformity, and complex reconstruction.3 The aim of this manuscript is to describe a new method of the surgical removal of an arachnoid cyst by the reconstruction of a left frontal bone deformity by turning the bone segment inside out and the outside inward. This provided a good aesthetic result and protected the region of surgical interest (ROSI).
CASE REPORT
A 17-year-old female patient attended the neurosurgery department complaining of a palpable mass in the left frontal bone as well as headaches and seizures since the age of 8 years. She was born after a normal labor. Nine years later, when she attended the clinic, a physical exam was undertaken that revealed a firm and rounded palpable mass at the left frontal bone (Figure 1A).
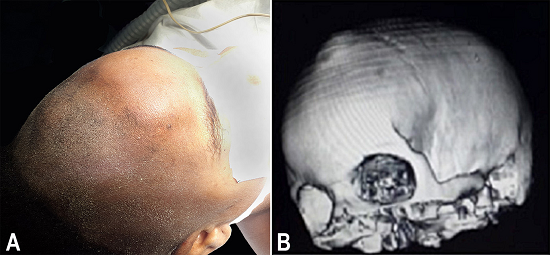
Figure 1
A - Panoramic view of the shaved head showing deformity of the left frontal bone; B - Computed tomography (CT) 3-D reconstruction showing a volume rendering view showing a protrusion of the left frontal bone.
On neurological exam, the patient had no focal signs. She had normal mental status and vital signs. She was conscious, and her pupillary reflex to light was normal, as were the muscular force, the deep tendon reflexes, and her sensibility. The computed tomography (CT) scan of her head showed a left frontal bone a protrusion (Figure 1B).
The CT scan also showed an underlying hypoattenuating, supratentorial lesion in the left frontal lobe and interhemispheric space, which was oval in shape with regular and well-defined borders, suggesting an arachnoid cyst that did not cause a shift in the midline structures when the left frontal lobe was compressed (Figure 2).
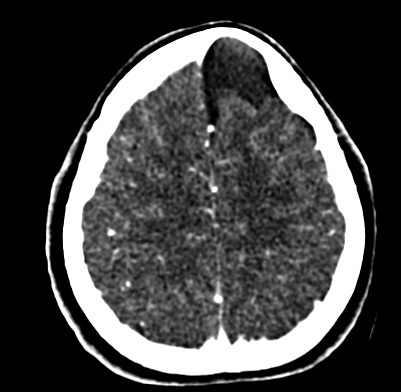
Figure 2
Brain CT - Axial view showing the left frontal cyst compressing the left frontal lobe.
The patient was operated on under general anesthesia in the supine position with her head in a neutral position. After the cranium was shaved and cleaned of hair, a bi-temporal incision was made. The underlying tissues were cut in a normal fashion until the left frontal bone deformity was revealed, which had a lilac color (Figure 3A). Six burr holes were made surrounding the deformity (Figure 3B). The bone dust was collected and the bridges between the holes were eliminated with a Gigli saw. A concave-convex bone flap was lifted, which revealed the arachnoid cyst (Figure 3C). The cyst membrane and 20 mL of the intracystic fluid (collected with a syringe) were sent for histological examination. After exeresis of the membrane, it was evident that the cerebral sulci at the level of the interhemispheric fissure and the adjacent areas of the left frontal lobe were flat and depressed due to compression by the cyst. The duramater was closed in a watertight fashion with polyester 5-0 (Figure 3D).
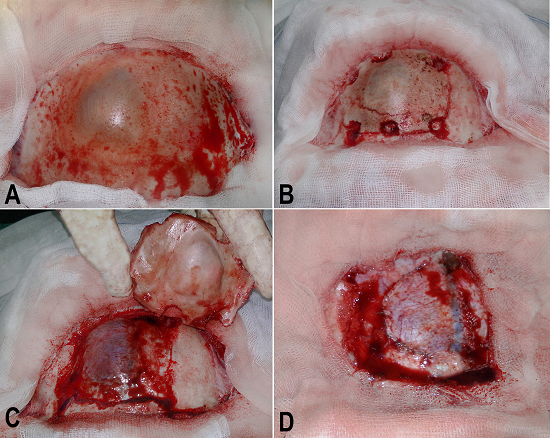
Figure 3
Intra operative steps. A - Macroscopic view of the left frontal bone showing a lilac color deformity; B - Six burr holes surrounding the protruding bone; C - The bone flap, the cyst, and the superior sagittal sinus; D - The duramater closed in a watertight fashion and the superior sagittal sinus.
An exeresis of the concave-convex and protruding surface of the bone flap was made using an electric saw, which created a free, smaller concave-convex fragment (Figure 4A). Three small holes were made in this free fragment as well as in the surrounding bone flap using a 2 mm low-speed drill. The free concave-convex fragment was placed after being turned inside out and upside down. This fragment was fixed to the surrounding bone using polyester 2-0 sutures (Figure 4B).
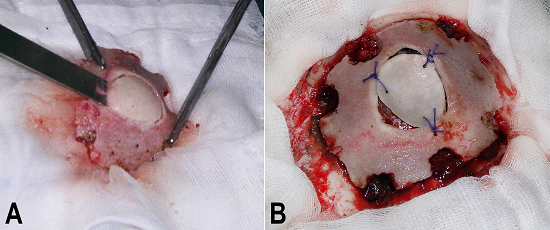
Figure 4
Bone flap management and replacement. A - Creating a free, smaller concave-convex fragment from the bone flap; B - The bone flap on the surgical area with the smaller concave-convex fragment fixed and the deformed surface inverted.
The resulting bone flap was returned to the skull, and the burr holes were filled with the bone dust that had been collected earlier during the burr placements. The closure was in the normal fashion using polyester 2-0 sutures.
The histological exam of the lesion confirmed the diagnosis of an arachnoid cyst. The patient was prescribed antibiotics, an anticonvulsant, and an analgesic during the postoperative period. A CT scan performed 1 week after surgery demonstrated the absence of the cyst and adequate surgical reconstruction (Figure 5A and 5B).
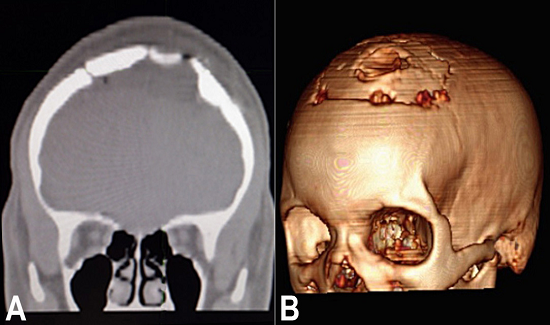
Figure 5
Brain CT. A - Coronal view showing the bone reconstruction after the inversion of the deformed surfaces, and the absence of the cystic lesion; B - 3-D reconstruction showing the restoration of the skull at the area of the craniotomy.
Ten days after surgery the patient was discharged. Currently, she is asymptomatic and her physical exam is normal.
DISCUSSION
Most arachnoid cysts are diagnosed at infancy and may cause symptoms during adolescence. In our study, the frontal localization of the cyst and the female sex of the patient were the uncommon features.4 Cysts must be operated on—independent of the age of the patient—if they are causing complications, such as high intracranial pressure, erosion, excavation, protrusions,5 or aesthetic problems, which were upsetting for the patient. In our case, the patient had seizures and migraines too. Because of these symptoms, the decision was made to operate.
The best treatment for arachnoid cysts is still controversial, and different techniques for the treatment and correction of deformities and defects caused by them have been published.6 Some techniques are decompression by craniotomy, endoscopic fenestration, stereotactic removal, ventriculoperitoneal shunt, and intracystic shunting.7 The method we used in the present case for exeresis of the cyst is a known method, which consisted of craniotomy, drainage, decompression, and the removal of the entire cyst membrane - but the method of reconstruction of the skull that we used is a new one.
Reconstruction of the skull is a procedure used to repair or reshape the skull.8 A variety of materials and methods have been used for the repair of cranial defects9 and to preserve the bone of the skull9 when it has been necessary to remove of part of it, as in the case of defects due to trauma or deformity caused by disease or pathological condition.
The method used for the reconstruction of our patient’s skull has not been published before. The piece of deformed bone was separated, inverted, put back, and fixed to the bone flap. The concept of combining the bone flap with the deformed area and inverting it is sufficient to eliminate the visible protrusion, which can upset the patient, and to aesthetically reshape the ROSI.
One option that can be added to this method is the use of biological glue (a fast-acting adhesive), by surrounding and involving the resulting external concavity of the inverted fragment.
This case study proposes an unpublished procedure for the reconstruction of the skull, which is different to previously published methods.10,11
CONCLUSION
An arachnoid cyst, which had caused painful and upsetting symptoms for the patient due to the cyst’s compression and bone protrusion, was surgically removed. The excision of the deformed area as a bone flap and the inversion of the concave-convex deformed surfaces by turning the inside out and the outside inwards, is a new and optional method, which provides protection to the ROSI and gives an aesthetically good result.
REFERENCES
1 Rengachary SS, Watanabe I. Ultrastructure and pathogenesis of intracranial arachnoid cysts. J Neuropathol Exp Neurol. 1981;40(1):61-83. 7205328 http://dx.doi.org/10.1097/00005072-198101000-00007
2 Gosalakkal JA. Intracranial arachnoid cysts in children: a review of pathogenesis, clinical features, and management. Pediatr Neurol. 2002;26(2):93-8. 11897472 http://dx.doi.org/10.1016/S0887-8994(01)00329-0.
3 Trivedi NP, Kuriakose, MA, Iyer S. Reconstruction in skull base surgery: review of current concepts. Indian J Plast Surg. 2007;40(12):52-29.
4 Johns Hopskin Hospital Pediatric Neurosurgery. Arachnoid cyst. Baltimore: Johns Hopskin; 2017 [cited 2017 Feb 23]. Available from: http://www.hopkinsmedicine.org/neurology_neurosurgery/centers_clinics/pediatric_neurosurgery/conditions/arachnoid_cysts.html
5 Gelabert-González, M Serramito-García R, Aran-Echabe E. et al. La fenestración endoscópica como tratamiento de los quistes aracnoideos intracraneales Endoscopic fenestration to treat intracranial arachnoid cysts. Salud(i)Ciencia. 2014;20, 586-91.
6 Harsh GR 4th, Edwards MS, Wilson CB. Intracranial arachnoid cysts in children. J Neurosurg. 1986;64(6):835-42. 3701434 http://dx.doi.org/10.3171/jns.1986.64.6.0835
7 Duz B, Kaya S, Daneyemez M, Gonul E. Surgical management strategies of intracranial arachnoid cysts: a single institution experience of 75 cases. Turk Neurosurg. 2012;22(5):591-8. PMid:23015336
8 Encyclopedia of Surgery Craniofacial reconstruction. 2017 [cited 2017 Feb 23]. Available from: http://www.surgeryencyclopedia.com/Ce-Fi/Craniofacial-Reconstruction.htm
9 Goiato MC, Anchieta RB, Pita MS, Santos DM. Reconstruction of skull defects: currently available materials. J Craniofac Surg. 2009;20(5):1512-8. 19816288 http://dx.doi.org/10.1097/SCS.0b013e3181b09b9a
10 Artico M, Ferrante L, Pastore FS, et al. Bone autografting of the calvaria and craniofacial skeleton: historical background, surgical results in a series of 15 patients, and review of the literature. Surg Neurol. 2003;60(1):71-9. 12865021 http://dx.doi.org/10.1016/S0090-3019(03)00031-4.
11 Rebouças DS, Ferreira TG, Andrade EL, Fortuna TC, Assis AF, Freitas CE. Abordagem cirúrgica de osteoma em osso frontal: relato de caso. Revista de Cirurgia e Traumatologia Buco-maxilo-facial. 2014;14(3), 09-14,.
Notes
Author notes
Correspondence Jorge Felix Companioni Rosildo Clinica Multiperfil - Department of Neurosurgery and Physiotherapy Rua do Futungo de Belas - Morro Bento - Luanda - Angola Phone: +244 226 434415 jfcompanioni@gmail.com
Conflict of interest declaration