Article / Clinical Case Report
Received: 29 June 2017
Accepted: 07 August 2017
DOI: https://doi.org/10.4322/acr.2017.025
ABSTRACT: Spontaneous regression (SR) of cancer, especially lung cancer, is a rare biological event with a mechanism that is not currently understood. Immunological mechanisms seem to be the stronger explanation in SR of a lung cancer. We report the rare case of SR of a lung adenocarcinoma stage IA, in a 75-year-old man, which was incidentally diagnosed and histologically confirmed. Due to the patient’s comorbidities and his poor pulmonary function, stereotactic radiotherapy was scheduled. However, by the time the treatment was due to start, the tumor was no longer detectable.
Keywords: Carcinoma, Non-Small-Cell Lung, Lung Neoplasms, Neoplasm Regression, Spontaneous.
CASE REPORT
Our patient was a 75-year-old Caucasian man with a medical history of heavy smoking, obstructive pulmonary disease, sleep apnea, arterial hypertension, infra-renal aortic aneurism, cardiac failure, endarterectomy of the ascending aorta, and aortic valve substitution.
He underwent a surveillance thoracoabdominal computed tomography (CT) scan 3 years ago that showed a suspicious 19 mm nodule in the right superior lobe (Figure 1), which was investigated by a transthoracic core biopsy. The pathology report revealed an adenocarcinoma with tubular pattern and same mucosecretory cells. The immunohistochemistry study with TTF1 was positive in neoplastic cells, to confirm the pulmonary origin of the adenocarcinoma (Figures 2A and 2B). A positron emission tomography (PET)-CT was performed and showed no other sites of radiotracer uptake, besides the pulmonary nodule (Figure 3) rendering the cT1N0M0 as stage IA.

Figure 1
Chest computed tomography scan revealing an irregular 19 mm nodule in the right superior lobe.
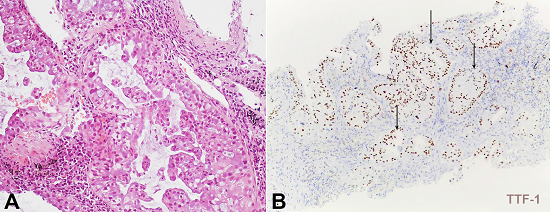
Figure 2
Microphotography of the lung biopsy. A - Acinar adenocarcinoma, with moderate pleomorphism (H&E, 200X); B - Positivity for TTF-1 (100X).
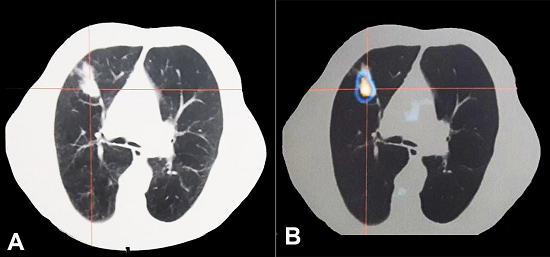
Figure 3
Chest positron emission tomography-computed tomography (PET-CT) (5 months after first CT, 3 months after biopsy). A - Axial CT acquisition; B - Increased 18F-deoxyglucose (FDG) uptake in the right superior lobe (standardized uptake value max = 6.8) without other FDG captation.
The patient then underwent pulmonary function tests that disclosed he was not a candidate for surgery (forced vital capacity [FVC]: 93.7%; forced expiratory volume in the first second [FEV1]: 40.9%; FEV 1/FVC ratio: 32.93%; and diffusion capacity of the lungs for carbon monoxide [DLCO]: 39.3%).
The case was analyzed in a multidisciplinary meeting, and was decided that stereotactic radiotherapy, would be the most appropriate treatment, because of his comorbidities and poor pulmonary function.
Three months after the core biopsy and 1 month after PET-CT, a planning CT scan before starting radiotherapy was conducted and the nodule was no longer seen. During this period, the patient didn’t have any infection, or started any new medication, namely systemic corticosteroid, or other immunosuppression. We performed sequential CT and PET-CT, which confirmed that the tumor had indeed disappeared (Figures 4 and 5). The histology was reviewed and the pathologist confirmed the diagnosis of lung adenocarcinoma.
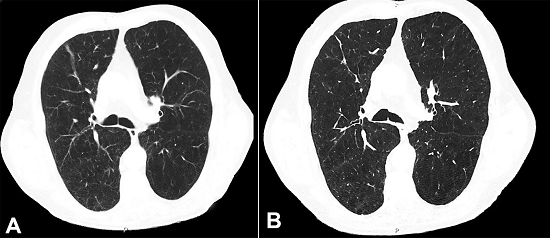
Figure 4
Chest computed tomography (CT). A - Six months after first CT and 4 months after the biopsy; note the vanishing of the right superior lobe 19 mm nodule; B - Absence of the nodule relapse 3 years after the diagnosis.
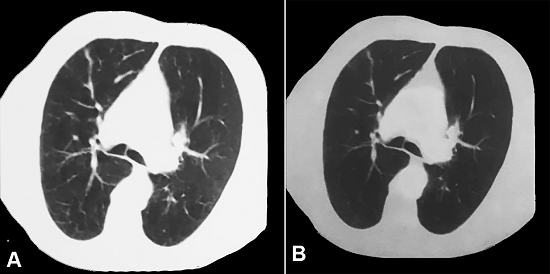
Figure 5
Chest positron emission tomography-computed tomography (PET-CT) performed 1 year after diagnosis. A - CT axial image acquisition; B - Absence of 18F-deoxyglucose captation.
The patient is currently undergoing regular follow-up examinations at this hospital, and has not shown any evidence of disease for the past 3 years.
This manuscript is in accordance with the institutional ethics committee, and the patient signed an informed consent.
DISCUSSION
Spontaneous regression (SR) of a cancer is defined as total or partial disappearance without treatment or in the presence of a known inappropriate/ineffective treatment in oncological diseases.1
This phenomenon is rare, but possible, and it has been found in several cases described in the literature. Everson and Cole,2 and Cole,3 reported 176 cases of SR from 1900 to 1964, with an estimated incidence of 1 out of 60,000-100,000 people with cancer.
The tumors in which this phenomenon is most frequently described are kidney cancer, neuroblastomas, and lymphomas.3 Currently, there are 17 well-documented case reports of lung cancer with SR (10 non-small cell lung cancer and 7 small cell lung cancer) (Table 1).4-20
Spontaneous remission of lung cancer proven in histological examinations: review of the literature
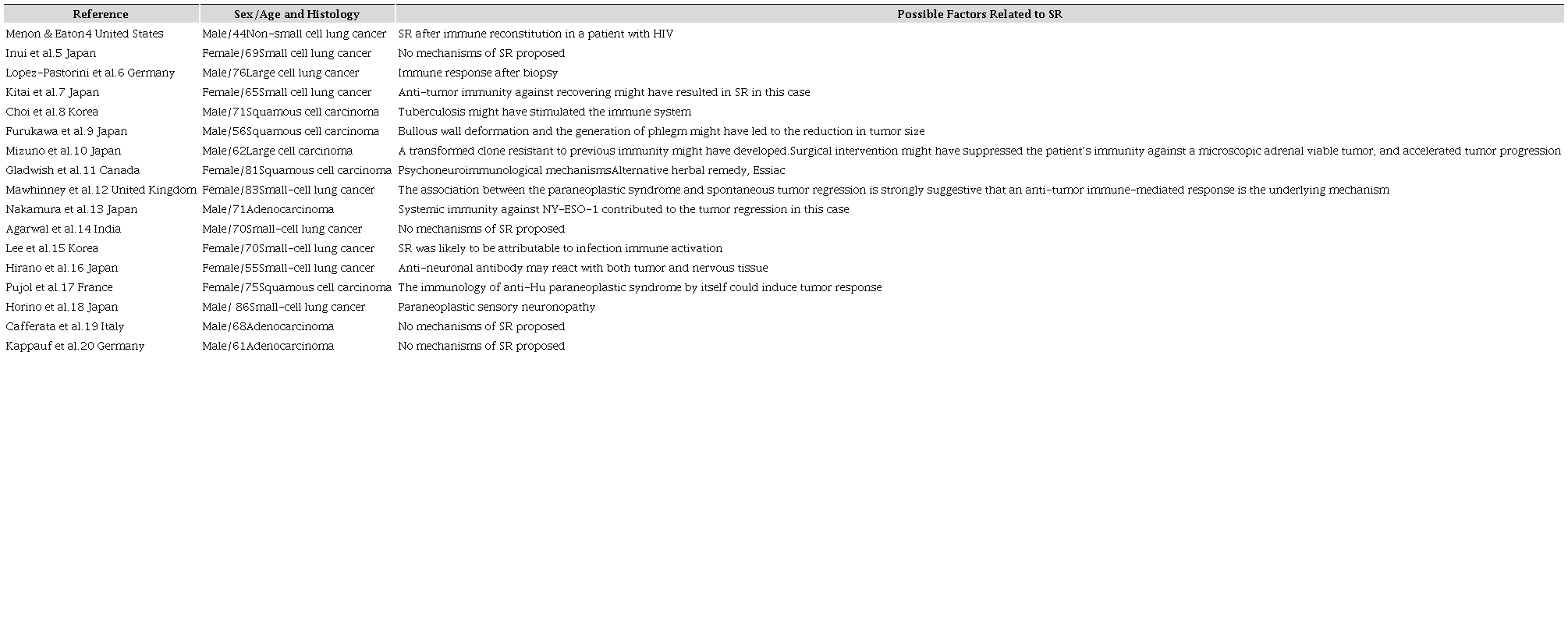
SR = spontaneous regression.
The exact mechanisms of the SR are unknown, but there are several hypotheses described in the literature; namely (i) immunological mechanisms; (ii) the existence of SR after a serious local infection; (iii) the suspension of immunosuppression therapy; (iv) immune reconstitution in HIV patients; and (v) paraneoplastic syndrome.21
Other possibly related factors described in the literature are: hormonal mechanisms; tumor necrosis; destruction of the tumor feeding artery during the biopsy; angiogenesis and telomerase inhibition; increased apoptosis; psycho-neurological factors; suspension of exogenous carcinogens; and the differentiation of malignant cells into benign ones.3,22
In this case, we did not find any certain mechanism of SR among those already described.
One possible explanation could be the destruction or emboli of the feeding artery of the tumor by the core needle biopsy. Another theory might be that the injury caused by this procedure could somehow elicit an inflammatory response or even release antigens that were hidden, with a consequent activation of the immune system.
Despite the absence of evidence of an immunological mechanism, such as paraneoplastic syndrome or an infection, we believe that the main mechanism in this patient’s case was probably his immune system activated by the needle core biopsy. Corroborating with this hypothesis is the recognition of lung cancer as an immunogenic tumor, especially in heavy smoking patients, which has been associated with response to immunotherapy (anti-PD1/PD-L1) and a higher neoantigen burden.5
CONCLUSION
The SR of a cancer is possible, and is a well-documented phenomenon in the literature. The mechanism of this event remains a mystery, and further research is essential to fully comprehend this unusual phenomenon.
In this case, the immune system of the patient activated by the needle core biopsy seems to be an important mechanism of SR.
REFERENCES
1 Kumar T, Patel N, Talwar A. Spontaneous regression of thoracic malignancies. Respir Med. 2010;104(10):1543-50. 20580882 http://dx.doi.org/10.1016/j.rmed.2010.04.026
2 Everson TC, Cole WH. Spontaneous regression of cancer. Philadelphia: WB Saunders; 1966.
3 Cole WH. Efforts to explain spontaneous regression of cancer. J Surg Oncol. 1981;17(3):201-9. 6166811 http://dx.doi.org/10.1002/jso.2930170302
4 Menon MP, Eaton KD. Spontaneous regression of non-small-cell lung cancer in AIDS after immune reconstitution. J Thorac Oncol. 2015;10(1):e1-2. 25654731 http://dx.doi.org/10.1097/JTO.0000000000000236
5 Inui M, Sano A, Asai I, Ito S, Tsuchiya T, Fukuda T. Spontaneous regression of small cell lung cancer. Cancer Treat Commun. 2015;3:21-3. http://dx.doi.org/10.1016/j.ctrc.2015.02.001
6 Lopez-Pastorini A, Plönes T, Brockmann M, Ludwig C, Beckers F, Stoelben E. Spontaneous regression of non-small cell lung cancer after biopsy of a mediastinal lymph node metastasis: a case report. J Med Case Reports. 2015;9(1):217. http://dx.doi.org/10.1186/s13256-015-0702-9
7 Kitai H, Sakakibara-Konishi J, Oizumi S, et al. Spontaneous regression of small cell lung cancer combined with cancer associated retinopathy. Lung Cancer. 2015;87(1):73-6. 25468200 http://dx.doi.org/10.1016/j.lungcan.2014.10.015
8 Choi SM, Go H, Chung D, Yim JJ. Spontaneous regression of squamous cell lung cancer. Am J Respir Crit Care Med. 2013;188(4):e5-6. 23947528 http://dx.doi.org/10.1164/rccm.201208-1417IM.
9 Furukawa M, Oto T, Yamane M, Toyooka S, Kiura K, Miyoshi S. Spontaneous regression of primary lung cancer arising from an emphysematous bulla. Ann Thorac Cardiovasc Surg. 2011;17(6):577-9. 21881362 http://dx.doi.org/10.5761/atcs.cr.10.01638
10 Mizuno T, Usami N, Okasaka T, Kawaguchi K, Okagawa T, Yokoi K. Complete spontaneous regression of non-small cell lung cancer followed by adrenal relapse. Chest. 2011;140(2):527-8. 21813532 http://dx.doi.org/10.1378/chest.10-2564.
11 Gladwish A, Clarke K, Bezjak A. Spontaneous regression in advanced non-small cell lung cancer. BMJ Case Rep. 2010;2010(1):bcr0720103147. 22802473 http://dx.doi.org/10.1136/bcr.07.2010.3147
12 Mawhinney E, Gray O, McVerry F, McDonnell GV. Paraneoplastic sensorimotor neuropathy associated with regression of small cell lung carcinoma. BMJ Case Rep. 2010;2010(1):bcr0120091486. 22802230 http://dx.doi.org/10.1136/bcr.01.2009.1486
13 Nakamura Y, Noguchi Y, Satoh E, et al. Spontaneous remission of a non-small cell lung cancer possibly caused by anti-NY-ESO-1 immunity. Lung Cancer. 2009;65(1):119-22. 19193472 http://dx.doi.org/10.1016/j.lungcan.2008.12.020
14 Agarwal P, Kapoor A, Khan A, Agarwal V. Spontaneous regression of an untreated lung cancer. Indian J Thorac Cardiovasc Surg. 2010;26(2):173-5. http://dx.doi.org/10.1007/s12055-010-0027-7
15 Lee YS, Kang H, Jang P, et al. Spontaneous regression of small cell lung cancer. Respirology. 2008;13(4):615-8. 18422866 http://dx.doi.org/10.1111/j.1440-1843.2008.01294.x.
16 Hirano S, Nakajima Y, Morino E, et al. A case of spontaneous regression of small cell lung cancer with progression of paraneoplastic sensory neuropathy. Lung Cancer. 2007;58(2):291-5. 17574297 http://dx.doi.org/10.1016/j.lungcan.2007.05.005
17 Pujol JL, Godard AL, Jacot W, Labauge P l. Spontaneous complete remission of a non-small cell lung cancer associated with anti-Hu antibody syndrome. J Thorac Oncol. 2007;2(2):168-70. 17410036 http://dx.doi.org/10.1097/JTO.0b013e31802f1c9d
18 Horino T, Takao T, Yamamoto M, Geshi T, Hashimoto K. Spontaneous remission of small cell lung cancer: a case report and review in the literature. Lung Cancer. 2006;53(2):249-52. 16790292 http://dx.doi.org/10.1016/j.lungcan.2006.05.011
19 Cafferata MA, Chiaramondia M, Monetti F, Ardizzoni A. Complete spontaneous remission of non-small-cell lung cancer: a case report. Lung Cancer. 2004;45(2):263-6. 15246199 http://dx.doi.org/10.1016/j.lungcan.2004.01.026
20 Kappauf H, Gallmeier WM, Wünsch PH, et al. Complete spontaneous remission in a patient with metastatic non-small-cell lung cancer. Ann Oncol. 1997;8(10):1031-9. 9402178 http://dx.doi.org/10.1023/A:1008209618128.
21 Sengupta N, MacFie TS, MacDonald TT, Pennington D, Silver AR. Cancer immunoediting and “spontaneous” tumor regression. Pathol Res Pract. 2010;206(1):1-8. 19945228 http://dx.doi.org/10.1016/j.prp.2009.10.001
22 Papac RJ. Spontaneous regression of cancer. Cancer Treat Rev. 1996;22(6):395-423. 9134002 http://dx.doi.org/10.1016/S0305-7372(96)90023-7.
Notes
Author notes
Correspondence Cristiana Marques Department of Oncology - Centro Hospitalar São João - University of Porto Alameda Prof. Hernâni Monteiro - Porto - Portugal CEP: 4200-319 Phone: +351 (91) 15 25 218 cristianapereiramarques@gmail.com
Conflict of interest declaration
