Article / Clinical Case Report
Mantle cell lymphoma: involvement of nodal and extranodal sites in the head and neck, with multifocal oral lesions
Mantle cell lymphoma: involvement of nodal and extranodal sites in the head and neck, with multifocal oral lesions
Autopsy and Case Reports, vol. 7, no. 3, pp. 26-31, 2017
Hospital Universitário da Universidade de São Paulo
Received: 14 June 2017
Accepted: 16 August 2017
ABSTRACT: Mantle cell lymphoma (MCL) is a malignant B-cell neoplasm, which comprises monomorphic and small- to medium-sized mantle zone-derived lymphoid cells. It is characterized by chromosomal translocation t(11;14)(q13;q32) and CCND1 truncation, resulting in cell cycle deregulation. It is an aggressive type of non-Hodgkin lymphoma with a propensity to present with extranodal involvement. This study shows the case of an 80-year-old Caucasian male who complained of a 2-month progressive swelling on the right side of his face. The magnetic resonance imaging exam showed multifocal involvement of the head and neck, including oral manifestations, bilateral parotid glands, palate, tongue, and floor of the mouth. An incisional biopsy of the tumor mass was performed. The morphological and immunophenotypic findings were consistent with the diagnosis of MCL. The patient died 4 months later, without any chance of undergoing a therapeutic approach. Although MCL is a rare condition, it should be subjected to a differential diagnosis when affecting the maxillofacial area. Imaging exams and both immunohistochemical and morphological analyses are needed to reach the correct diagnosis. Here, we present an unusual MCL with multifocal involvement of the head and neck.
Keywords: Lymphoma, Mantle Cell, Oral Manifestations, Head and Neck Neoplasms, Magnetic Resonance Imaging, Salivary Glands.
INTRODUCTION
Non-Hodgkin lymphoma (NHL) most commonly presents in extranodal sites; that is, the gastrointestinal tract, followed by the head and neck region (especially Waldeyer’s ring), which are the most frequent locations of involvement.1-4 In the oral cavity, NHL is rare, accounting for less than 5% of all oral malignant neoplasms.4,5
Mantle cell lymphoma (MCL) represents 6% of all NHLs,1,2 which comprises monomorphic and small to medium-sized mantle-zone-derived lymphoid cells. It is characterized by chromosomal translocation t (11;14)(q13;q32) and CCND1 truncation, resulting in cell cycle deregulation.1,6,7 MCL is prevalent in male individuals during adulthood and affects patients in the sixth and seventh decades of life.2,5 Patients are usually diagnosed in the advanced stages of the disease, confirming the aggressive behavior of MCL.1,2
Few cases of MCL in the oral cavity have been reported, and most of them include the involvement of the palate and the tongue.8-10 Salivary glands are rarely affected, accounting for only 3% of the reported cases.7 Magnetic resonance imaging (MRI) is the method of choice for evaluating NHL, which assesses the exact tumor extension, the possible local and distant involvement, and the nodal status.7,11
The purpose of this study was to report the case of an extensive MCL that affected both the nodal and the extranodal sites in the head and neck region, as observed in MRI scans. To our knowledge, this is the first report of a multifocal MCL in the maxillofacial region.
CASE REPORT
An 80-year-old Caucasian man was referred to the Stomatology Department, because he presented with a swelling on the right side of his face, which he first noticed 2 months earlier. His medical history included chronic renal failure.
The extraoral examination revealed a swelling of the right parotid gland and the submandibular gland, as well as an extensive ipsilateral cervical lymphadenopathy. On intraoral examination, two masses were observed: one on the left side of the palate and the other on the floor of the mouth (Figure 1). Tongue mobility was normal and there was no evidence of paresthesia of the lingual nerve.
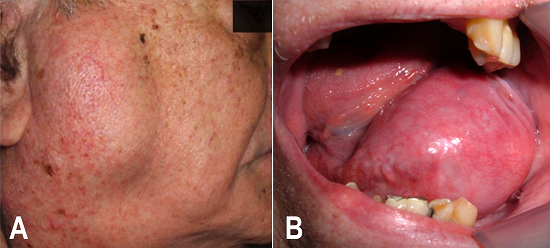
Figure 1
Clinical presentation of mantle cell lymphoma. A - The right parotid gland and submandibular regions are affected; B - A tumor mass is observed intraorally on the left side of the floor of the mouth.
Examination of the right parotid gland by MRI revealed a solid and expansive mass in the superficial lobe, which was characterized by a hyposignal and a hypersignal on a T1-weighted image (T1W) and a T2-weighted image (T2W), respectively. Another two nodular masses were observed in the inferior pole of the parotid gland. MRI also examined the contralateral parotid gland, and three small nodular masses were observed in the superficial lobe, which presented signal features similar to those on the right side. Moreover, a mass involving the left side of the palate showed continuity, with an ipsilateral narrowing of the pharyngeal airspace (Figure 2A and 2B). The posterior two-thirds of the tongue (left side) and both lingual tonsils showed expansive lesions. The epiglottis was posteriorly displaced and the vallecula was obliterated, leading to narrowing of the pharyngeal airspace (Figure 2C). Evidence of expansive masses was also noted on the floor of the mouth and in both sublingual and submandibular areas, without affecting the salivary glands. Bilateral lymphadenopathy was also observed, in contrast with the clinical examination findings (Figure 2D). Considering the clinical and imaging findings, the working diagnosis pointed to a malignant disease.
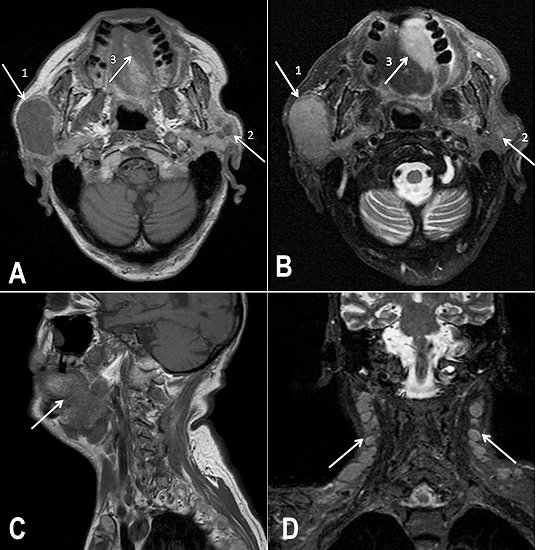
Figure 2
Cervical MRI: Axial view of: A - T1W image; B - T2W image. (1) Superficial lobe of the right parotid gland affected by the MCL. (2) Nodular formations in the superficial lobe of the left parotid gland. (3) Expansive lesion in the palate; C - Sagittal view of T1W image showing a tumor mass affecting the palate and its continuity to the pharyngeal airspace; D - Coronal view of T2W image showing the involvement of cervical lymph nodes. MRI = magnetic resonance imaging; T1W = T1-weighted; T2W = T2-weighted.
An incisional biopsy was performed on the floor of the mouth, and the histopathological examination showed a monotonous proliferation of small- to medium-sized lymphocytes, with slightly irregular nuclei and moderately dispersed chromatin. The growth pattern was predominantly diffuse, in contrast with a sparsely nodular pattern. Also, focal hyalinized vessels and scarce epithelioid histiocytes were observed. An immunohistochemical analysis revealed neoplastic cells, which were positive for CD20, CD5, and cyclin D1, but negative for CD3, CD4, and CD23 (Figure 3). The final diagnosis was MCL, and the patient died 4 months later.
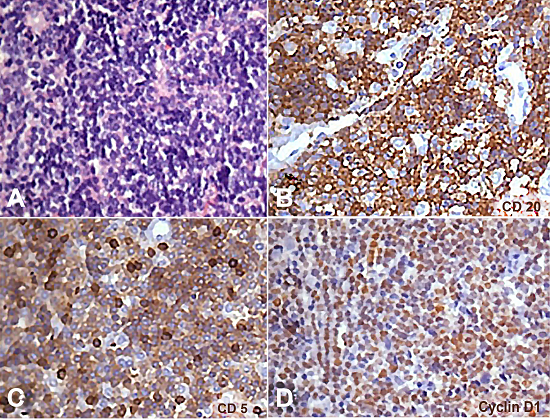
Figure 3
Photomicrography of the biopsy specimen. A - Monotonous lymphoid proliferation of small- to medium-sized lymphocytes (H&E, 100X); B, C, and D - Immunohistochemical profile showing positivity for CD20, CD5, and cyclin D1 in the neoplastic cells (400X).
The patient signed an informed consent.
DISCUSSION
NHL is considered the third most common malignancy in the oral cavity, although it accounts for less than 5% of all oral cancers. MCL is a rare and aggressive form of NHL, affecting adults ranging from middle age to older, with male predominance.2-5,10 The clinical course of MCL varies from an indolent disease to a rapidly progressive malignancy. A tumor mass, with or without ulceration, is the most common manifestation found in the oral cavity.6,8
The parotid glands are the major salivary glands most often affected by MCL.3,4,7,8,12,13 Primary presentation of MCL within the oral cavity is uncommom.4,8,12 Usually, MCL presents as a stage-III/IV disease at the time of diagnosis, with extranodal involvement, especially in the bone narrow, peripheral blood, gastrointestinal tract, spleen, and Waldeyer’s ring.1,8 Extranodal manifestations can be challenging for clinicians, since they may be multifocal manifestations of NHL in advanced stages, such as Burkitt lymphoma. In addition, there are two subgroups; namely, diffuse large B-cell lymphoma (DLBCL) and extranodal marginal zone B-cell lymphoma of the mucosa-associated lymphoid tissue (MALT), in which patients present with the involvement of several extranodal sites.14 As well as the aforementioned considerations, this case report includes both nodal and extranodal involvement by MCL in the head and neck with multifocal oral manifestation, which is extremely unusual.
Diagnosis of MCL requires both morphological and immunophenotypic analysis. Immunohistochemical analysis usually shows positivity for CD20, CD5, CD43, and remarkably cyclin D1, as well as immunoglobulin IgM and/or IgD. Moreover, SOX11 was identified to be exclusively overexpressed in MCL, including the cyclin D1-negative cases; however, MCL is negative for CD10, CD23, and BCL6.7-9,15 Furthermore, chromosomal translocation t(11;14)(q13;q32) and the presence of cyclin D1 (CCND1/PRAD1) genes in almost all cases is considered to be the primary genetic event. As a result, overexpression of the cyclin D1 protein is thought to lead to deregulation of the normal cell cycle, particularly in the G1/S phase transition.1,6,7,15,16 As indicated by morphological evaluation, most lesions exhibit cytologic features resembling centrocytes. A small subset may show blastoid or pleomorphic features, which are often associated with aggressive clinical behavior.8,16 The current case showed the cellular features of a classic variant of MCL, with a predominantly diffuse growth pattern and typical immunohistochemical findings, which confirmed the diagnosis.
Of all the available imaging methods, MRI offers the best soft tissue contrast and spatial resolution, with the advantage of not using ionizing radiation.11 For patients with palpable masses in the parotid gland area, MRI is the gold standard method, due to its precision in assessing the exact extension of the mass, the possible invasion of adjacent structures, the perineural spread, and the lymph node staging.7,11,12 Lymphomas exhibit homogenous signal patterns, with hyposignal and hypersignal intensities in T1W and T2W images, respectively.7,12 The clinical features and MRI findings of the current case study highlight the potential of MCL to disseminate—of which physicians should be aware—based on the suggestive multifocal manifestation of the disease.
MCL is characterized by an aggressive clinical course and a poor prognosis.1,6,7,8 The MCL International Prognostic Index (MIPI) stratifies the risk by taking into account the clinical and laboratory features, and classifies the patients into low, intermediate, and high-risk groups.1,6 Regardless of the MIPI classification, only 5%-10% of patients survive longer than 3 years.8,15 The heterogeneous biological behavior of the disease makes it difficult to establish a treatment of choice.1,15 Treatment varies from chemotherapy to a combination of chemotherapy and radiotherapy.8,10 Improvements in treatment have been achieved by using conventional chemotherapy together with autologous stem cell transplantation. However, no standard treatment for patients with MCL is currently available, and the disease is still considered to be incurable.6 Relatively few patients (30%) have a complete response to combination chemotherapy.15 The case reported herein presented an advanced stage of the disease at the time of diagnosis, and the patient unfortunately died before any treatment planning could be scheduled, thus confirming the poor prognosis of MCL.
CONCLUSION
This case report presents an unusual case of MCL with multifocal involvement in the head and neck region, including oral manifestation in the palate, tongue, and floor of the mouth. Although a rare condition, MCL should be subjected to differential diagnosis when it affects the maxillofacial area. Imaging exams plus morphological and immunophenotypic analyses are needed to establish the correct diagnosis. However, the diagnosis of MCL can be challenging because of its similarities to other types of NHL.
REFERENCES
1 Skarbnik AP, Goy AH. Mantle cell lymphoma: state of the art. Clin Adv Hematol Oncol. 2015;13(1):44-55. PMid:25679973
2 Zhou Y, Wang H, Fang W, et al. Incidence trends of mantle cell lymphoma in the United States between 1992 and 2004. Cancer. 2008;113(4):791-8. 18615506 http://dx.doi.org/10.1002/cncr.23608
3 Etemad-Moghadam S, Tirgary F, Keshavarz S, Alaeddini M. Head and neck non-Hodgkin’s lymphoma: a 20-year demographic study of 381 cases. Int J Oral Maxillofac Surg. 2010;39(9):869-72. 20538427 http://dx.doi.org/10.1016/j.ijom.2010.03.029
4 Triantafillidou K, Dimitrakopoulos J, Iordanidis F, Gkagkalis A. Extranodal non-Hodgkin lymphomas of the oral cavity and maxillofacial region: a clinical study of 58 cases and review of the literature. J Oral Maxillofac Surg. 2012;70(12):2776-85. 22494508 http://dx.doi.org/10.1016/j.joms.2012.01.018
5 Barnes L, Eveson JW, Reichart P, Sidransky D, editors. Pathology and genetics of tumours of the head and neck. Lyon: IARC Press; 2005. v. 9.
6 Chen Y, Wang M, Romaguera J. Current regimens and novel agents for mantle cell lymphoma. Br J Haematol. 2014;167(1):3-18. 24974852 http://dx.doi.org/10.1111/bjh.13000
7 Pilavaki M, Athanasiadou A, Iordanidis F, Karakozoglou T, Palladas P. Magnetic resonance imaging with pathological correlation in a case of mantle cell lymphoma of the parotid gland: a case report. J Med Case Reports. 2010;4(1):99. 20350332 http://dx.doi.org/10.1186/1752-1947-4-99
8 Guggisberg K, Jordan RC. Mantle cell lymphoma of the oral cavity: case series and comprehensive review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109(1):98-104. 19880332 http://dx.doi.org/10.1016/j.tripleo.2009.08.010
9 Kyo C, Kawaoka Y, Kinoshita K, Ohno H. Mantle cell lymphoma presenting with a tumor of the hard palate. Intern Med. 2010;49(15):1663-6. 20686311 http://dx.doi.org/10.2169/internalmedicine.49.3436
10 Guastafierro S, Falcone U, Celentano M, Cappabianca S, Giudice A, Colella G. Primary mantle-cell non-Hodgkin’s lymphoma of the tongue. Int J Hematol. 2008;88(2):206-8. 18629601 http://dx.doi.org/10.1007/s12185-008-0142-z
11 Burke CJ, Thomas RH, Howlett D. Imaging the major salivary glands. Br J Oral Maxillofac Surg. 2011;49(4):261-9. 20381221 http://dx.doi.org/10.1016/j.bjoms.2010.03.002
12 Lee YY, Wong KT, King AD, Ahuja AT. Imaging of salivary gland tumours. Eur J Radiol. 2008;66(3):419-36. 18337041 http://dx.doi.org/10.1016/j.ejrad.2008.01.027
13 Jaffe ES. Lymphoid lesions of the head and neck: a model of lymphocyte homing and lymphomagenesis. Mod Pathol. 2002;15(3):255-63. 11904341 http://dx.doi.org/10.1038/modpathol.3880521
14 Economopoulos T, Papageorgiou S, Rontogianni D, et al. Multifocal extranodal non-Hodgkin lymphoma: a clinicopathologic study of 37 cases in Greece, a Hellenic Cooperative Oncology Group study. Oncologist. 2005;10(9):734-8. 16249354 http://dx.doi.org/10.1634/theoncologist.10-9-734.
15 Lenz G, Dreyling M, Hiddemann W. Mantle cell lymphoma: established therapeutic options and future directions. Ann Hematol. 2004;83(2):71-7. 14669040 http://dx.doi.org/10.1007/s00277-003-0774-2
16 Gao J, Peterson L, Nelson B, Goolsby C, Chen YH. Immunophenotypic variations in mantle cell lymphoma. Am J Clin Pathol. 2009;132(5):699-706. 19846810 http://dx.doi.org/10.1309/AJCPV8LN5ENMZOVY
Notes
Author notes
Correspondence Juliane Piragine Araujo Discipline of Oral Radiology - Department of Stomatology - School of Dentistry - University of Sao Paulo (USP) Av. Professor Lineu Prestes, 2227 - Butantã - São Paulo/SP - Brazil CEP: 05508-000 Phone: +55 (11) 3091-7831 jupiragine@usp.br
Conflict of interest declaration