Review Article
Gelatinous transformation of bone marrow: rare or underdiagnosed?
Gelatinous transformation of bone marrow: rare or underdiagnosed?
Autopsy and Case Reports, vol. 7, no. 4, pp. 8-17, 2017
Hospital Universitário da Universidade de São Paulo
Received: 01 October 2017
Accepted: 24 October 2017
ABSTRACT: Gelatinous transformation of the bone marrow (GTBM) is a rare hematologic entity, which was first described by Paul Michael in 1930. GTBM is mostly associated with caloric intake/anorexia nervosa, although it also has been described accompanying other pathologic conditions, such as malignancy, systemic lupus erythematosus, HIV infections. Even though the diagnostic features of the hematopoietic tissue, such as hypoplasia, adipose cell atrophy, and deposition of a gelatinous substance in the bone marrow (which stains with Alcian blue at pH 2.5) are quite specific, the underlying pathogenic mechanisms remain poorly understood. Considering the evidence of reversibility—notably in cases of malnutrition and anorexia—this entity should be kept high on cards as a possible differential diagnosis of patients presenting with cytopenias and associated weight loss or starvation, especially in developing countries with nutritionally deprived populations. On an extensive review of the literature aimed at comprehensively addressing the evolution of the GTBM from the past century until now, we conclude that the lack of clinical suspicion and awareness regarding this pathologic entity has led to misdiagnosis and delayed diagnosis.
Keywords: Bone Marrow Disease, Bone Marrow Examination, Bone Marrow.
INTRODUCTION
Gelatinous transformation of bone marrow (GTBM)—also known as starvation marrow—gelatinous degeneration and serous atrophy of bone marrow is a well-defined hematologic entity.1,2 Although the first references were noticed in works of Virchow (1821-1902), Herter (1865-1910), and Adami (1862-1926), it was Paul Michael, in 1930, who first reported 11 cases of GTBM in the bone marrow of autopsied cases.1 A large number of studies published at the end of the 20th century worldwide, considered GTBM as a histologic pattern originating from an associated cause rather than being a disease entity by itself.3
In fact, GTBM has been described in association with a variety of clinical scenarios, chiefly in the young with malnourishment and anorexia.3,4 In cases with high clinical suspicion, the diagnosis can be easily established by studying the bone marrow aspirate or bone biopsy with Alcian blue staining at pH 2.5, which loses positivity after pre-treatment with hyaluronidase.3 The reported rare incidence of GTBM might just be the tip of the iceberg, with the lack of clinical suspicion being the most probable culprit for so few diagnoses.
This review was undertaken to study the epidemiological behavior and incidence of GTBM reports over the years while focusing on clinical profiles, hematologic parameters and investigations, and proposed pathogenic mechanism.
MATERIAL AND METHODS
In our pre-specified protocol, we used the keywords “gelatinous transformation/degeneration of the bone marrow, starvation marrow, and serous atrophy of the marrow” to identify the target papers for a systematic literature search. The databases, PubMed, Medline, Google Scholar and Research Gate, were accessed to retrieve the articles published until June 2017.
Case and series reports, original research articles, images, letters to editors with titles having the aforementioned keywords were included in the study. Data including the first author’s last name, publication year, country of origin and total number of cases reported in each study was compiled. All open access articles and abstracts of subscribed articles were included in the study.
Articles published in a language other than English for which no translation or English abstract was available, were excluded.
All articles fulfilling inclusion criteria were reviewed in duplicate and independently, and data extraction was held by two authors (KKS & GSS).
All articles were assessed for following variables: total number of studies published with total number of cases; clinical profile including age, sex and the associated disease; altered hematological indices; diagnostic work-up modality (cytological and/or histologic parameters of bone marrow); reversal or improvement with treatment; and additional information reported with respect to the pathogenesis of GTBM by the different authors.
Data were compiled in chronological order (decade wise); however, no quantitative data synthesis or statistical analysis could be performed due to considerable clinical and mathematical heterogeneity of the compiled data.
RESULTS
Our literature search gathered 79 papers (N) with relevant titles, amounting the total of 522 reported cases (n) as shown in Table 1. Of these 79 papers, 66 were in the English language while 13 were in other languages, such as French, German, Dutch, and Polish. Of these 13 studies, 4 had an English language abstract. Hence the remaining 09 articles (n = 26) were excluded.

BMA = bone marrow aspirate; BMB = bone marrow biopsy; btw = between; EPO = erythropoietin; GTBM = gelatinous transformation of bone marrow; NA = not available; PRBCs = packed red blood cells; SLE = systemic lupus erythematosus.* No full published article was available during this time period; hence, data interpretation is limited.** Mehta et al.16 reported in 22/75 cases of HIV (86% males, mean age: 33 years; all were anemic, 50% cases hypocellular, aspirate more difficult).*** Jain et al.4 (India) studied 43 cases, 14 of which were children; mostly presented anemia and malnourishment.
A final list of 70 titles was compiled, which comprised 48 full articles (n = 394) and only 22 Abstracts (n = 102). Out of these, 48 open access articles were subjected to review by two authors independently and the remaining 22 subscribed articles only with abstracts were reviewed for available data.
We observed that the research articles on GTBM, which constituted the bulk of cases, had limited information on the parameters of the individual cases. Hence, the scope for statistical analysis of data was limited. However, an overall trend was established based on the available data.
Incidence of Gelatinous Transformation of Bone Marrow Over the Last Century
The first available published study on GTBM by Paul Michael (1930) comprised a total of 11 cases.1 Over the following three decades, no published data were available. In 1967, a study by Pearson5 surfaced, reporting GTBM in three cases of anorexia nervosa. In the subsequent decade; two more studies were published by Tavassoli et al.6 (1976) and Seamen et al.2 (1978) who described the condition in 9 and 14 cases, respectively. In the 1980s, six more studies were published, describing the condition in seven different patients. However, no open access article could be found on a literature search of the archives till 1990.7-12 The number of studies tripled (N = 18) in the 1990s with a total of 52 cases reported,13-30 including one original research article by Mehta et al.16 who described the condition in 22 patients with HIV—the first ever study from India—by Ray et al.17 in 1992, and another one by Basu et al.26 At the dawn of the 21st century, a deluge of research articles on GTBM were published. Among them, 21 new studies appeared in the first decade itself, including the largest study by Bohm3 (2000) who studied 80,000 bone marrow samples and reported the GTBM incidence of 0.2%.3,4,31-49 In the last 7 years, 30 new studies comprising 117 cases were published.50-79 Thus, a total of 79 studies with 522 individual cases of GTBM have been published in the last 87 years (Table 1). These data clearly indicate a rising trend in reporting the condition, especially in the last two decades.
Clinical Profiles
Our analysis showed a total of 236 male patients compared to 160 females with a M:F ratio of 1.5:1. Cases were divided into four age groups: <15 years, 16-40 years, 41-60 years and >60 years. In the initial studies, the most commonly involved age group was 40-60 years and >60 years with an occasional case in the <15 years age group. However, with more cases of young patients being reported in the past two decades, a total of 143 cases were noted in the age group of 15-40 years, followed by the elderly age group of >60 years (103).
In our analysis, a total of 70 cases were seen in the <15 years age group (Table 1). The most common reported etiologies associated with GTBM were anorexia nervosa, and malnutrition or malabsorption with weight loss (47 cases). Similarly, the majority of cases, reported by Jain et al.4 (the largest case series from India), also concluded that malnutrition is the most common condition associated with GTBM. Further GTBM associated with malignancy was reported in 109 cases and comprised several types of cancers, such as hepatocellular carcinoma,64 oral cancers,74 along with primary malignancies of the bone marrow, such as acute myeloid leukemia (AML),14 and chronic myeloid leukemia (CML)47. Another 60 cases were associated with different types of infective agents excluding those reported in HIV patients.16 A total of 17 cases of aplastic anemia with GTBM were reported in study by Sen et al.37 As in cases of malignancy, HIV infection and chronic infections, like tuberculosis, where weight loss is quite often an associated complaint, there seems to be an overlap leading to an underestimation of cases of GTBM associated with anorexia and malnutrition. A total of 40 cases were labeled as miscellaneous, which comprised different associated diseases, such as systemic lupus erythematosus,15,49 visceral Leishmaniasis,17 hemochromatosis;48 and metabolic abnormalities, such as hyperthyroidism, adrenal insuffiency,74 pyrexia of unknown origin, and alcoholic pancreatitis have also been published.
Investigations
The most common altered laboratory parameter found in the majority of the cases was the presence of at least one peripheral cytopenia. In this setting, anemia was the most common. In some of the larger series, almost 100% of the cases were reported to have anaemia.4,16,37,63 Pancytopenia as the initial presentation was present in 22 cases.58,64,65,68,70,73 However, cytopenias were occasionally lacking,41,71 and a single case of myelofibrosis, accompanied by GTBM, had leukocytosis along with thrombocytosis.31
In all cases, the diagnosis was initially achieved either on a bone marrow aspirate or bone marrow biopsy; however, the bone marrow biopsy was reported to be the method of choice mainly in cases with a dry tap on bone marrow aspiration.3,63 Histological examination was characterized by different patterns of bone marrow cellularity, varying from hypocellularity to normocellularity—or even cases of hypercellularity with focal areas of hypocellularity surrounding the gelatinous deposits.31,63,65,66 Böhm3 graded the bone marrows from 1 to 4 based on the severity of gelatinous transformation.
Bone marrows were stained with Alcian blue at pH 2.5 along with routine H&E stains and additional stains like Congo Red, and periodic acid-Schiff to rule out other differential diagnoses.
Prognosis
Pearson5 and Tavassoli et al.6 firstly reported the reversibility of GTBM on animal experiments. In our review, we found 35 cases that showed the disappearance of the GTBM on follow-up on repeated biopsy/aspirate after the initiation of treatment, which was either in the form of nutritional diet (15 cases),58,60,62,66 packed red blood cell (PRBCs) transfusion (one case),57 granulocyte colony stimulating factor (G-CSFs) (three cases)51 or treatment of the underlying disease.
DISCUSSION
Since 1930, there has been an increasing number of reported cases of GTBM. From the advent of the 21st century, more than 50 studies were published accounting for more than 400 new cases (Table 1). The majority of these cases were from countries like India where GTBM was unheard of before the 1990s. The reported incidence of GTBM varies from 0.2%,3 to 4.4%37 and 4.8%.66 This rising trend in its incidence over the years indicates that GTBM, in the current scenario, is anything but rare. On review of the literature, Seaman et al.2 seems to aptly describe GTBM as “Not uncommon,” whereas the majority of studies continue to report it as “a rare condition.” Based on our analysis, we conclude that the low incidence observed in the 20th century can be ascribed to the lack of awareness about the existence of such an entity.
Overall, there is a male preponderance in the cases reported so far.3,37 However, in certain studies, like Abella et al.,36 all 22 cases reported were females while in study by Mehta et al;16 86% cases were males. This may probably be due to a selection bias in such studies. Young adults and the elderly constitute the most commonly affected age;3 however, there has been an increase in the number of cases reported in the pediatric age group over last two decades, most of which have been reported from India.4,37,65 Hence, it is noteworthy that no age group is immune to the condition, and thus GTBM should not be neglected as a differential diagnosis in any age group.
The underlying disease spectrum associated with GTBM is heterogeneous. The most common association had been reported with cases of malnourishment/starvation resulting from various causes like anorexia, chronic infections, or malignancy.1 Though most of the initial case reports were associated with non-hematopoietic malignancies, recently GTBM has been reported in association with various hematopoietic malignancies like AML,14,18,25 acute promyelocytic leukemia (APML) on All Trans Retinoic Acid,70 acute lymphocytic leukemia (with and without dasatinib),61,63 CML on imatinib,47,55,56,72 CML in chronic phase,50 myelodysplastic syndrome,45,59 multiple myeloma33 and myelofibrosis,31 which also have been published from all over the world. In many of these cases, marked weight loss with anorexia was present,44,63,74,77 thus pointing to the possibility that the underlying mechanism resulting in the development of GTBM remains the same as in the cases of chronic infections and malignancies, anorexia, and malnutrition.
A remarkable number of patients had bi- or pancytopenia at the initial presentation, and almost all had anemia, irrespective of the underlying associated disease. Even though no correlation between the severity of GTBM and the peripheral hematological parameters have been reported,3,63 it still should be kept in the differential diagnosis of cytopenias. Regarding the investigation modality, bone marrow biopsy appears to be the gold standard, and it appears preferable to perform trephine biopsy along with aspirate in suspected cases rather than doing aspirate alone. In 2010, Sims80 described the characteristic findings of patchy areas of hyperintensity in T2-weighted images in cases of GTBM detected by magnetic resonance imaging (MRI). However, there are cases of GTBM misdiagnosed as spinal tumours32 or misinterpreted as technical errors on MRI.75
The diagnosis is easily achieved in bone marrow biopsy, which exhibits the features of hematopoietic hypoplasia, adipose cell atrophy, and the deposition of gelatinous substance in bone marrow that stains with Alcian blue at pH 2.5 (Figure 1).1,3,6 However, a large number of cases present normocellular or hypercellular marrows or focal areas of hypocellularity surrounding the gelatinous substance, which easily can be misinterpreted as bone marrow edema, necrosis, or amyloid. The misinterpretation occurs with a lack of suspicion or knowledge of this entity. (Table 2).3,69 Recently, GTBM post-chemotherapy has been reported without fat atrophy.18,33 Although the pathogenesis of GTBM remains unknown, the majority of the studies, especially in cases of nutritional deprivation, agree upon a common pathophysiologic mechanism of fat mobilization in the face of starvation followed by the deposition of hyaluronic acid.This excessive accumulation of extracellular gelatinous material interferes with the hematopoietic microenvironment leading to the suppression of hematopoiesis, which is reflected as peripheral blood cytopenias.51,59
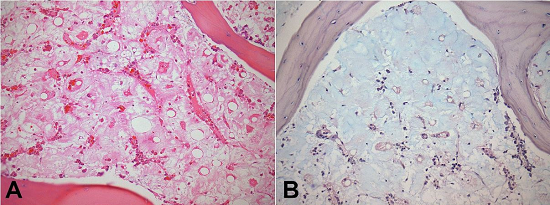
Figure 1
Photomicrography of the bone marrow. A - marked hypocellularity of the hematopoietic cells and scant fat tissue immersed in an amorphous eosinophilic material (H&E, 200X); B - this stains blue with Alcian blue staining (200X). This is consistent with the diagnosis of gelatinous transformation of the bone marrow in an autopsy case of a severely malnourished corpse (Figures provided by Dr. Aloísio Felipe-Silva, MD, PhD; chief of the Anatomic Pathology Service, Hospital Universitário, University of São Paulo).

GTBM = gelatinous transformation of bone marrow; PAS = periodic acid-Schiff.
In GTBM associated with infectious diseases, as in HIV infection, the secretion of cytokines, such as interleukin (IL)-1, IL-2, and the tumor necrosis factor, are considered to be the driving factors.43 Similarly, it may hold true for the cases associated with malignancy. Alternate theory suggests that the tumor cells may play a role in the initiation of hyaluronic acid formation.11 In the cases of GTBM following chemotherapy, the inhibition of tyrosine kinase activity leads to the blockage of downstream signal pathways affecting extracellular matrix deposition, and adipocyte differentiation has been proposed as the possible mechanism.72 Local milieu factors of the marrow as the systemic “stress factors” have been proposed as the inciting factors for the development of GTBM in cases associated with aplastic anaemia.37
Long-term outcomes and the prognosis of GTBM have not been well documented yet. A few authors have stated that GTBM, by itself, does not have any prognostic significance, and that the survival of patients who develop GTBM is dependent on the nature and stage of the underlying disease at the time of the diagnosis.3,18,37,70,81 However, with the increasing number of case reports showing an improvement of the GTBM in patients after balanced nutrition,81 PRBCs,57, G-CSFs,51 erythropoietin,58 the irreversibility of GTBM has been questioned. Mant and Faragher81 reported that GTBM is a temporary condition, which reverses on balanced nutrition in cases of anorexia nervosa. The timely diagnosis and early treatment in such cases would reduce the costs of long-term health care expenses,51 especially in developing countries, like India.
CONCLUSION
From an extensive review of the literature, we conclude that GTBM is a condition that is underdiagnosed because of the lack of clinical suspicion. Though large-scale prospective studies are required to establish the pathogenesis, GTBM should be considered as a differential diagnosis in all cases presenting with weight loss, malnutrition, and refractory peripheral cytopenias—irrespective of age profile and associated co-morbidities.
ACKNOWLEDGMENT
We are indebted to Dr. Fernando Peixoto Ferraz de Campos, MD, Hospital Universitário, University of São Paulo, São Paulo, SP, Brazil, for his efforts in securing the photomicrographs, and Dr. Aloísio Felipe Silva, MD, PhD, Chief of the Anatomic Pathology Service Hospital Universitário, University of São Paulo, for providing the photographs for the manuscript.
REFERENCES
1 Michael P. Gelatinous degeneration of the bone marrow. J Pathol Bacteriol. 1930;33(3):533-8. http://dx.doi.org/10.1002/path.1700330304
2 Seaman JP, Kjeldsberg CR, Linker A. Gelatinous transformation of the bone marrow. Hum Pathol. 1978;9(6):685-92. 730150 http://dx.doi.org/10.1016/S0046-8177(78)80051-3.
3 Böhm J. Gelatinous transformation of the bone marrow: the spectrum of underlying diseases. Am J Surg Pathol. 2000;24(1):56-65. 10632488 http://dx.doi.org/10.1097/00000478-200001000-00007
4 Jain R, Singh ZN, Khurana N, Singh T. Gelatinous transformation of bone marrow: a study of 43 cases. Indian J Pathol Microbiol. 2005;48(1):1-3. PMid:16758772
5 Pearson HA. Marrow hypoplasia in anorexia nervosa. J Pediatr. 1967;71(2):211-5. 4226478 http://dx.doi.org/10.1016/S0022-3476(67)80074-X.
6 Tavassoli M, Eastlund DT, Yam LT, Neiman RS, Finkel H. Gelatinous transformation of bone marrow in prolonged self-induced starvation. Scand J Haematol. 1976;16(4):311-9. 132697 http://dx.doi.org/10.1111/j.1600-0609.1976.tb01156.x.
7 Clarke BE, Brown DJ, Xipell JM. Gelatinous transformation of the bone marrow. Pathology. 1983;15(1):85-8. 6222282 http://dx.doi.org/10.3109/00313028309061408
8 Maréchaud R, Abadie JC, Babin P, Lessart M, Sudre Y. Reversible bone marrow hypoplasia in a case of male anorexia nervosa. Ann Med Interne. 1985;136(1):36-40. PMid:4003995
9 Steinberg SE, Nasraway S, Peterson L. Reversal of severe serous atrophy of the bone marrow in anorexia nervosa. JPEN J Parenter Enteral Nutr. 1987;11(4):422-3. 3112434 http://dx.doi.org/10.1177/0148607187011004422
10 Woessner S, Lafuente R, Martin E, Florensa L, Marill MR. Gelatinous transformation of the bone marrow. Cyto-histologic, histochemical and ultrastructural study of a case. Sangre. 1988;33(2):147-9. PMid:2969624
11 Ifrah N, Saint-Andre JP, Gentile L, et al. Gelatinous transformation of the bone marrow: manifestation of an acute leukemia? Acta Haematol. 1989;82(3):165-8. 2510441 http://dx.doi.org/10.1159/000205369
12 Taguchi H, Enzan H, Shibuya K, et al. Gelatinous transformation of the bone marrow in anorexia nervosa: report of two cases. Journal of the Japan Soc Reticuloendothel Sys. 1990;30(3):193-9. http://dx.doi.org/10.3960/jslrt1961.30.193
13 Jensen KD, Anagnostaki L. Gelatinous bone marrow transformation. Ugeskr Laeger. 1990;152(3):171-2. PMid:2105551
14 Feng CS. Gelatinous transformation of marrow in a case of acute myelogenous leukemia post-chemotherapy. A J Hematol. 1991;38(3):220-2.
15 Feng CS, Ng MH, Szeto RS, Li EK. Bone marrow findings in lupus patients with pancytopenia. Pathology. 1991;23(1):5-7. 2062568 http://dx.doi.org/10.3109/00313029109061430
16 Mehta K, Gascon P, Robboy S. The gelatinous bone marrow (serous atrophy) in patients with acquired immunodeficiency syndrome: Evidence of excess sulfated glycosaminoglycan. Arch Pathol Lab Med. 1992;116(5):504-8. PMid:1580754
17 Ray R, Bhoria U, Varma N, Bambery P, Dash S. Gelatinous transformation of bone marrow. J Assoc Physicians India. 1992;40(4):277-8. PMid:1452541
18 Feng CS. A variant of gelatinous transformation of marrow in leukemic patients post-chemotherapy. Pathology. 1993;25(3):294-6. 8265250 http://dx.doi.org/10.3109/00313029309066592
19 Sicard D, Casadevall N, Wyplosz B, Picart F, Blanene P. Anorexia nervosa and gelatinous transformation of bone marrow. Nouv Rev Fr Hematol. 1994;36(Suppl 1):S85-6. PMid:8177724
20 Bailly D, Lambin I, Garzon G, Parquet PJ. Bone marrow hypoplasia in anorexia nervosa: a case report. Int J Eat Disord. 1994;16(1):97-100. 7920588 http://dx.doi.org/10.1002/1098-108X(199407)16:1<97::AID-EAT2260160112>3.0.CO;2-N.
21 Mehler PS, Howe SE. Serous fat atrophy with leukopenia in severe anorexia nervosa. Am J Hematol. 1995;49(2):171-2. 7771474 http://dx.doi.org/10.1002/ajh.2830490219
22 Yakoub-Agha I, Galland S, Colmar-Montiel C, Poilane B, Morice P. Gelatinous transformation of the bone marrow in anorexia nervosa. Ann Med Interne. 1995;146(3):203-4. PMid:7653930
23 Bachmeyer C, Lamotte I, Dhote R, et al. Pancytopenia and gelatinous transformation of the bone marrow in anorexia nervosa. Ann Med Interne. 1995;146(2):129-30. PMid:7598339
24 Feugier P, Guerci A, Boman F, Stockemer V, Lederlin P. Gelatinous transformation of the bone marrow. Apropos of 3 cases. Rev Med Interne. 1995;16(1):15-9. 7871266 http://dx.doi.org/10.1016/0248-8663(96)80660-6.
25 Arranz R, Gil-Fernandez JJ, Acevedo A, Tomas JF, Alegre A, Fernandez-Rañada JM. Gelatinous degeneration presenting as a preleukaemic syndrome. J Clin Pathol. 1996;49(6):512-4. 8763271 http://dx.doi.org/10.1136/jcp.49.6.512
26 Basu S, Mitra S, Marwaha RK, Garewal G. Gelatinous transformation of bone marrow. Indian J Pathol Microbiol. 1997;40(3):383-4. PMid:9354013
27 Nonaka D, Tanaka M, Takaki K, Umeno M, Okamura T, Taketa H. Gelatinous bone marrow transformation complicated by self-induced malnutrition. Acta Haematol. 1998;100(2):88-90. 9792939 http://dx.doi.org/10.1159/000040872
28 Shultz A, Yam LT. Gelatinous transformation of bone marrow. J Ky Med Assoc. 1998;96(1):10-2. PMid:9470310
29 Marie I, Levesque H, Heron F, Courtois H, Callat MP. Gelatinous transformation of the bone marrow: an uncommon manifestation of intestinal lymphangiectasia (Waldmann’s disease). Am J Med. 1999;107(1):99-100. PMid:10403358
30 Sasaki Y, Yamagishi F, Yagi T, Mizutani F. A case of pulmonary tuberculosis case with pancytopenia accompanied to bone marrow gelatinous transformation. Kekkaku. 1999;74(4):361-4. PMid:10355222
31 Böhm J, Schmitt-Graff A. Gelatinous bone marrow transformation in a case of idiopathic myelofibrosis: a morphological paradox. Pathol Res Pract. 2000;196(11):775-9. 11186174 http://dx.doi.org/10.1016/S0344-0338(00)80111-9.
32 Chim CS, Wat NM, Ma SK. The irreplaceable image: Serous degeneration of the bone marrow. Haematologica. 2001;86(5):558. PMid:11410430
33 Mathew M, Mathews I, Manohar C, Rao S. Gelatinous transformation of bone marrow following chemotherapy for myeloma. Indian J Pathol Microbiol. 2001;44(1):53-4. PMid:12561997
34 Tieulie N, Sudaka I, Kaphan R, et al. Gelatinous transformation of bone marrow: 4 cases. Presse Medicale (Paris, France: 1983). 2001;30(24 Pt1):1209-10.
35 Singh H, Singh S, Gupta MS, et al. Gelatinous transformation of the bone marrow complicated by self induced starvation. J Assoc Physicians India. 2002;11(2):98.
36 Abella E, Feliu E, Granada I, et al. Bone marrow changes in anorexia nervosa are correlated with the amount of weight loss and not with other clinical findings. Am J Clin Pathol. 2002;118(4):582-8. 12375646 http://dx.doi.org/10.1309/2Y7X-YDXK-006B-XLT2
37 Sen R, Singh S, Singh H, Gupta A, Sen J. Clinical profile in gelatinous bone marrow transformation. J Assoc Physicians India. 2003;51:585-8. PMid:15266925
38 Wang C, Amato D, Fernandes B. Gelatinous transformation of bone marrow from a starch-free diet. Am J Hematol. 2001;68(1):58-9. 11559938 http://dx.doi.org/10.1002/ajh.1149
39 Orlandi E, Boselli P, Covezzi R, Bonaccorsi G, Guaraldi GP. Reversal of bone marrow hypoplasia in anorexia nervosa: Case report. Int J Eat Disord. 2000;27(4):480-2. 10744856 http://dx.doi.org/10.1002/(SICI)1098-108X(200005)27:4<480::AID-EAT14>3.0.CO;2-3.
40 Nishio S, Yamada H, Yamada K, et al. Severe neutropenia with gelatinous bone marrow transformation in anorexia nervosa: a case report. Int J Eat Disord. 2003;33(3):360-3. 12655634 http://dx.doi.org/10.1002/eat.10143
41 Chen SH, Hung IJ, Jaing TH, Sun CF. Gelatinous degeneration of the bone marrow in anorexia nervosa. Chang Gung Med J. 2004;27(11):845-9. PMid:15796262
42 Stroup JS, Stephens JR, Baker DL. Gelatinous bone marrow in an HIV-positive patient. Proc Bayl Univ Med Cent. 2007;20(3):254-6. PMid:17637880
43 Boullu-Ciocca S, Darmon P, Sebahoun G, Silaghi A, Dutour-Meyer A. Gelatinous bone marrow transformation in anorexia nervosa. Ann Endocrinol. 2005;66(1):7-11. 15798582 http://dx.doi.org/10.1016/S0003-4266(05)81680-4.
44 Murugan P, Chandrakumar S, Basu D, Hamide A. Gelatinous transformation of bone marrow in acquired immunodeficiency syndrome. Pathology. 2007;39(2):287-8. 17454770 http://dx.doi.org/10.1080/00313020701230989
45 Niscola P, Maurillo L, Palombi M, et al. Gelatinous degeneration of the bone marrow: two case reports showing different hematological features and clinical outcomes. Acta Haematol. 2007;118(3):165-6. 17890850 http://dx.doi.org/10.1159/000108766
46 Thiel A, Heits F, Amthor M. Severe leukopenia and bone marrow hypoplasia with gelatinous transformation in anorexia nervosa. Deutsche Medizinische Wochenschrift. 2007;132(43):2256-8.
47 Ram R, Gafter-Gvili A, Okon E, Pazgal I, Shpilberg O, Raanani P. Gelatinous transformation of bone marrow in chronic myeloid leukemia during treatment with imatinib mesylate: a disease or a drug effect? Acta Haematol. 2008;119(2):104-7. 18367829 http://dx.doi.org/10.1159/000121825
48 Munfus DL, Menke DM. Case of severe serous fat atrophy. Mayo Clin Proc. 2009;84(7):570. 19567708 http://dx.doi.org/10.1016/S0025-6196(11)60743-X.
49 Yamamoto M, Belmont HM, Utsunomiya M, Hidaka Y, Kishimoto M. Gelatinous transformation of the bone marrow in systemic lupus erythematosus. Lupus. 2009;18(12):1108-11. 19762388 http://dx.doi.org/10.1177/0961203309106344
50 Hong FS, Mitchell CA, Zantomio D. Gelatinous transformation of the bone marrow as a late morphological change in imatinib mesylate treated chronic myeloid leukaemia. Pathology. 2010;42(1):84-5. 20025487 http://dx.doi.org/10.3109/00313020903434686
51 Charania RS, Kern WF, Charkrabarty S, Holter J. Successful management of gelatinous transformation of the bone marrow in anorexia nervosa with hematopoietic growth factors. Int J Eat Disord. 2011;44(5):469-72. 20593416 http://dx.doi.org/10.1002/eat.20833
52 Rivière E, Pillot J, Saghi T, et al. Gelatinous transformation of the bone marrow and acute hepatitis in a woman suffering from anorexia nervosa. Rev Med Interne. 2012;33(7):38-40. PMid:22265096
53 Brennan CM, Atkins KA, Druzgal CH, Gaskin CM. Magnetic resonance imaging appearance of scurvy with gelatinous bone marrow transformation. Skeletal Radiol. 2012;41(3):357-60. 22223127 http://dx.doi.org/10.1007/s00256-011-1350-9
54 Cotta CV. Gelatinous transformation. Blood. 2012;120(11):2166. 23136659 http://dx.doi.org/10.1182/blood-2012-02-408815
55 Agrawal P, Sharma P, Narang V, Varma N, Malhotra P, Varma S. Gelatinous marrow transformation in an imatinib-treated CML patient with pancytopenia following severe sepsis. Indian J Hematol Blood Transfus. 2014;30(1):72-4. 24554832 http://dx.doi.org/10.1007/s12288-012-0188-1
56 Thakral B, Higa B, Venkataraman G, Velankar MM. Bone marrow with gelatinous transformation associated with residual disease in imatinib mesylate-treated chronic myelogenous leukaemia (CML). Pathology. 2012;44(1):59. 22157697 http://dx.doi.org/10.1097/PAT.0b013e32834e42df
57 Niscola P, Palombi M, Fratoni S, et al. Long-term survival of a patient with bone marrow gelatinous degeneration of idiopathic origin. Korean J Hematol. 2012;47(4):309-10. 23320013 http://dx.doi.org/10.5045/kjh.2012.47.4.309
58 Morii K, Yamamoto T, Kishida H, Okushin H. Gelatinous transformation of bone marrow in patients with anorexia nervosa. Intern Med. 2013;52(17):2005-6. 23995005 http://dx.doi.org/10.2169/internalmedicine.52.0912
59 Nakanishi R, Ishida M, Hodohara K, et al. Prominent gelatinous bone marrow transformation presenting prior to myelodysplastic syndrome: a case report with review of the literature. Int J Clin Exp Pathol. 2013;6(8):1677-82. PMid:23923088
60 Rafiullah F, Islam R, Mahmood R, Sitwala KV. Gelatinous bone marrow transformation secondary to unusual eating habits and drastic weight loss. BMJ Case Rep. 2013;2013:bcr2013200243. 23861277. http://dx.doi.org/10.1136/bcr-2013-200243
61 Sharma SK, Choudhary D, Handoo A, et al. Gelatinous transformation of bone marrow following the use of dasatinib in a patient with philadelphia chromosome-positive acute lymphoblastic leukemia. Leuk Res Rep. 2013;2(1):7-8. 24371767 http://dx.doi.org/10.1016/j.lrr.2012.11.004
62 Osgood E, Muddassir S, Jaju M, Moser R, Farid F, Mewada N. Starvation marrow - gelatinous transformation of bone marrow. J Community Hosp Intern Med Perspect. 2014;4(4):24811. 25317270 http://dx.doi.org/10.3402/jchimp.v4.24811
63 Das S, Mishra P, Kar R, Basu D. Gelatinous marrow transformation: a series of 11 cases from a tertiary care centre in South India. Turk J Haematol. 2014;31(2):175-9. 25035676 http://dx.doi.org/10.4274/Tjh.2012.0151
64 Chang J, Park CJ. Gelatinous transformation of the bone marrow in hepatocellular carcinoma. Blood Res. 2015;50(2):71. 26157774 http://dx.doi.org/10.5045/br.2015.50.2.71
65 Dikondwar AR, Gupta AP, Kawthalkar SM, et al. Gelatinous transformation of bone marrow: a rare cause of pancytopenia. Annals Pathol Lab Med. 2015;2(2):138-41.
66 Singh S, Gupta M, Singh G, et al. Gelatinous transformation of bone marrow: a prospective tertiary center study, indicating varying trends in epidemiology and pathogenesis. Indian J Hematol Blood Transfus. 2016;32(Suppl 1):358-60. 27408437 http://dx.doi.org/10.1007/s12288-015-0514-5
67 Villate A, Iquel S, Legac E. Gelatinous transformation of the bone marrow: a retrospective monocentric case series of 12 patients. Rev Med Interne. 2016;37(7):448-52. 26632481 http://dx.doi.org/10.1016/j.revmed.2015.10.349
68 Schafernak KT. Gelatinous transformation of the bone marrow from anorexia nervosa. Blood. 2016;127(10):1374. 28092875 http://dx.doi.org/10.1182/blood-2015-11-683946
69 Barbin FF, Oliveira CC. Gelatinous transformation of bone marrow. A&CR. 2017;7(2):5-8.
70 Goyal M, Gupta A, Yarlagadda S, Handoo A. Fatty but starving marrow! Gelatinous transformation of bone marrow secondary to plasma cell disorder and all-trans-retinoic acid therapy: a report of two cases. South Asian J Cancer. 2017;6(1):40-1. 28413801 http://dx.doi.org/10.4103/2278-330X.202563
71 Sung CW, Hsieh KL, Lin YH, et al. Serous degeneration of bone marrow mimics spinal tumor. Eur Spine J. 2017;26(Suppl 1):80-4. 27652677 http://dx.doi.org/10.1007/s00586-016-4778-8
72 Chang E, Rivero G, Jiang B, et al. Gelatinous marrow transformation associated with imatinib: case report and literature review. Case Rep Hematol. 2017;2017:1950724.
73 Mohamed M, Khalafallah A. Gelatinous transformation of bone marrow in a patient with severe anorexia nervosa. Int J Hematol. 2013;97(2):157-8. 23271414 http://dx.doi.org/10.1007/s12185-012-1255-y
74 Obata Y, Tamba S, Yamada Y, et al. Resolution of gelatinous bone marrow transformation following hormone replacement therapy in a patient with primary insufficiency of the adrenal and thyroid glands. Intern Med. 2013;52(17):1931-6. 23994986 http://dx.doi.org/10.2169/internalmedicine.52.0081
75 Boutin RD, White LM, Laor T, et al. MRI findings of serous atrophy of bone marrow and associated complications. Eur Radiol. 2015;25(9):2771-8. 25773942 http://dx.doi.org/10.1007/s00330-015-3692-5
76 Khanna R, Verma S, Singh VK, Belurkar S. Serous atrophy of bone marrow: a rare cause of paediatric cytopenia. Int J Pharma Bio Sci. 2017;8(3):849-53. http://dx.doi.org/10.22376/ijpbs.2017.8.3.b849-853.
77 Akhtar K, Rizvi W, Sherwani RK. Gelatinous transformation of the bone marrow: a rare presentation. Int J Pharmaceut Chem Sci. 2017;6(2):30-3.
78 Chari BM, Somal PK, Belurkar S, et al. Serous atrophy of the marrow in anorexia nervosa - a case report. Int J Med Sci Clin Invent. 2014;1(9):489-92.
79 Roper E, Jackett L. An example of gelatinousbone marrow transformation. Pathology. 2017;49(2):S85-6. http://dx.doi.org/10.1016/j.pathol.2016.12.235
80 Sims K. Musculoskeletal MRI. J Canadian Chiropractic Assoc. 2010;54(2):134.
81 Mant MJ, Faragher BS. The haematology of anorexia nervosa. Br J Haematol. 1972;23(6):737-49. 4265027 http://dx.doi.org/10.1111/j.1365-2141.1972.tb03488.x.
Notes
Author notes
Correspondence Khushdeep Kaur Shergill Department of Pathology, Armed Forces Medical College (AFMC) Pune - Maharashtra - India - 411040 Phone: 070303991112 shergillkhushdeep@gmail.com
Conflict of interest declaration