Image in Focus
Pseudoxanthoma elasticum
Pseudoxanthoma elasticum
Autopsy and Case Reports, vol. 7, no. 4, pp. 18-21, 2017
Hospital Universitário da Universidade de São Paulo
Keywords: Pseudoxanthoma Elasticum, Elastic Tissue, Vascular Calcification
Pseudoxanthoma elasticum (PXE) is an autosomal recessive disease of the connective tissue, which is characterized by mutations in the ABCC6 gene complex, located in chromosome 16p13. The precise prevalence is unknown, although it is estimated at 1/50,000 people. Diagnosing this condition is a challenge for physicians as the typical clinical features develop later in life, with cutaneous disorders being the earliest manifestation.1-3
Women are more often affected than men, in a ratio of 2:1. At birth, clinical manifestations are generally absent and the skin lesions start to develop in the first or second decade. As mentioned above, the cutaneous findings are frequently the first symptom of PXE. The most common areas affected are the lateral and posterior regions of the neck, the flexural areas (axillae, inguinal region, antecubital, and popliteal fossae), and the periumbilical area. The clinical feature is expressed by asymptomatic small papules (1-5 mm), yellowish or skin-tone, which blend together into large reticular plaques.4
Within the disease course, the patient starts presenting numerous cardiovascular manifestations, which include reduced peripheral pulse, hypertension, angina pectoris, and intermittent claudication. Since PXE patients may have premature atherosclerosis (caused by the mineralization and fragmentation of the elastic fibers of the medium-sized arteries and the aorta) they can also have early acute myocardial infarcts and cerebrovascular accidents. Furthermore, they have a higher cardiovascular risk as a result of alterations in lipoprotein composition and hypertriglyceridemia.4
The most important histological feature of PXE is elastorrhexis, a pattern at the middle dermis, which shows progressive mineralization and disintegration of the elastic fibers. Using light microscopy and relevant specific stains—such as Verhoeff-Van Gieson, and for calcium (Von Kossa or Alizarin Red)—fragmented elastic fibers and mid-dermal calcification will be shown, respectively, which are essential for the diagnosis of PXE. This deterioration of the elastic fibers results in dermatologic, ophthalmologic, and vascular dysfunction.3,4
In 2010, Plomp et al.5 proposed new criteria (Table 1) for the diagnosis of PXE. Their requirements are listed below, but it is also necessary to exclude causes of PXE-like disease, such as sickle cell anemia, beta-thalassemia, and PXE-like phenotype with cutis laxa and multiple coagulation factor deficiency (when mutational analysis of ABCC6 is negative or not available).
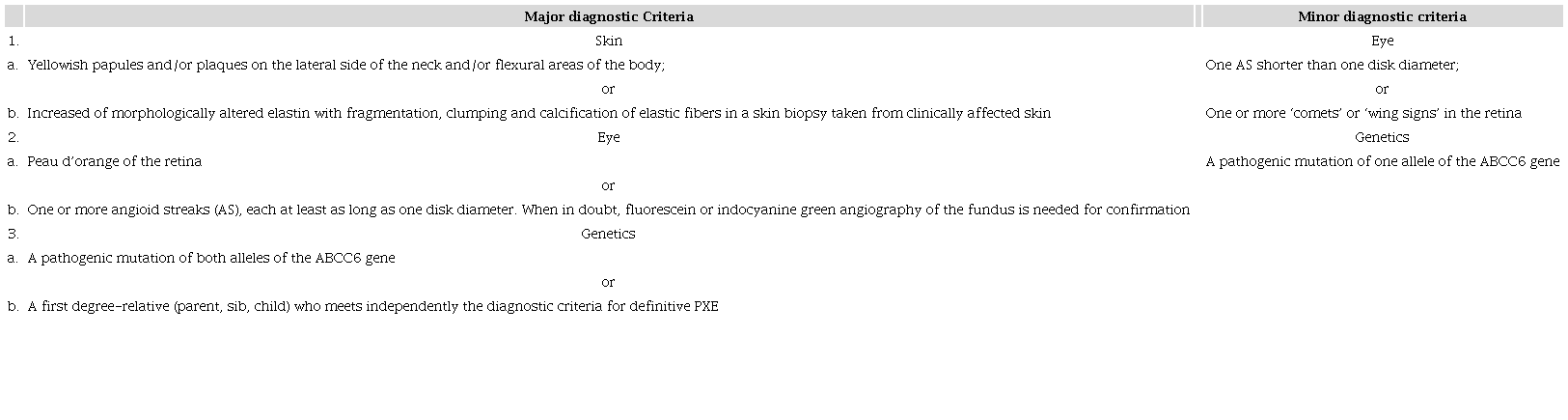
Table reproduced with the consent and acknowledgment of Jong PT5
Criteria for the diagnosis of PXE are:
-
Definitive diagnosis: The presence of two (or more) major criteria not belonging to the same category (skin, eye, genetics);
-
Probable diagnosis: The presence of two major eye or two major skin criteria, or the presence of one major criterion and one or more minor criteria not belonging to the same category as the major criterion;
-
Possible diagnosis: The presence of a single major criterion, or the presence of one or more minor criteria.
Despite the genetic progress in understanding this syndrome, no specific treatment is available. Some authors believe that a dietary supplementation with magnesium and a phosphate binder could have benefits in these patients, but this is still a controversial topic. Another study by Guo and colleagues6, utilizing Abcc6-/- mice, showed that starting a statin (atorvastatin) at age 4 weeks reduced lipid values and ameliorated vascular calcification (particularly at the higher dose)6. Some authors claim that statin is useful; however, further studies are needed.7
Nevertheless, the only fully accepted treatment is ocular manifestation, with the use of agents derived from the humanized monoclonal antibody to the vascular endothelial growth factor, which have shown effectiveness in choroidal manifestation.3
The above images refer to a 27-year-old woman who sought the dermatological clinic with a 15-year history of asymptomatic cervical and axillary cutaneous lesions. Her medical history included visual impairment, a former abortion after 12 weeks’ gestation, and a previous pregnancy with severe pre-eclampsia. On physical examination, the cervical and axillary regions presented a parchment-like elastic skin with yellowish papules clustered together forming plaques (Figure 1A and B). She also had loss of peripheral pulses and fundoscopy with bilateral angioid streaks. As suspected, the histopathological examination revealed grouped, fragmented, and twisted material in the middle dermis, which is consistent with calcified elastic fibers (Weirgt von Gieson [Figure 1C] and Von Kossa [Figure 1D]), and resulted in the diagnosis of PXE. However, we also excluded sickle cell anemia beta-thalassemia and coagulation factor deficiency.
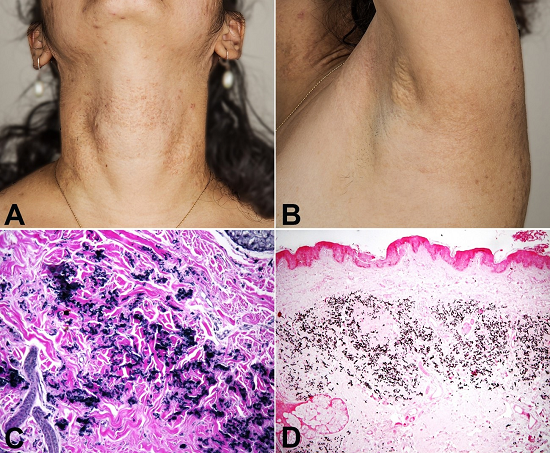
Figure 1
A - Skin-toned papules coalescing together into large plaques situated at the anterior and lateral sections of the neck. Also, the skin became flaccid; B - Yellowish, small papules grouped together in the flexural area (axillar) ; C - Weigert van Gieson stain by light microscopy shows material in the middle dermis grouped, fragmented, and twisted, which is consistent with elastic fibers; D - Von Kossa stain examined by light microscopy demonstrates that this material in the middle dermis blends in black, which represents calcium deposition. Therefore, as noticed in sequence, it shows calcified elastic fibers.
References
1 Germain DP. Pseudoxanthoma elasticum. Orphanet J Rare Dis. 2017;12(1):85. 28486967 http://dx.doi.org/10.1186/s13023-017-0639-8
2 Moitra K, Garcia S, Jaldin M, et al. ABCC6 and pseudoxanthoma elasticum: the face of a rare disease from genetics to advocacy. Int J Mol Sci. 2017;18(7):1488. 28696355 http://dx.doi.org/10.3390/ijms18071488
3 Uitto J, Jiang Q, Vàradi A, Bercovitch LG, Terry SF. Pseudoxanthoma elasticum: diagnostic features, classification, and treatment options. Expert Opin Orphan Drugs. 2014;2(6):567-77. 25383264 http://dx.doi.org/10.1517/21678707.2014.908702
4 Marconi B, Bobyr I, Campanati A, et al. Pseudoxanthoma elasticum and skin: Clinical manifestations, histopathology, pathomechanism, perspectives of treatment. Intractable Rare Dis Res. 2015;4(3):113-22. 26361562 http://dx.doi.org/10.5582/irdr.2015.01014
5 Plomp AS, Toonstra J, Bergen AA, van Dijk MR, de Jong PT. Proposal for updating the pseudoxanthoma elasticum classification system and a review of the clinical findings. Am J Med Genet A. 2010;152A(4):1049-58. 20358627 http://dx.doi.org/10.1002/ajmg.a.33329
6 Guo H, Li Q, Chou DW, Uitto J. Atorvastatin counteracts aberrant soft tissue mineralization in a mouse model of pseudoxanthoma elasticum (Abcc6−/−). J Mol Med (Berl). 2013;91(10):1177-84. 23807484 http://dx.doi.org/10.1007/s00109-013-1066-5
7 Luft FC. Pseudoxanthoma elasticum and statin prophylaxis. J Mol Med (Berl). 2013;91(10):1129-30. 24026849 http://dx.doi.org/10.1007/s00109-013-1082-5
Notes
Author notes
Correspondence Bruna Morassi Sasso Rua Tessália Vieira de Camargo, 126 - Cidade Universitária Zeferino Vaz - Campinas/SP - Brazil CEP: 13083-887 Phone: +55 (19) 3521-7541 bruna.derma@gmail.com
Conflict of interest declaration