Image in Focus
Received: 13 January 2018
Accepted: 21 February 2018
DOI: https://doi.org/10.4322/acr.2018.014
Keywords: Nail Diseases, Breast Neoplasms, Antineoplastic Agents, Hypoalbuminemia
Muehrcke’s lines (ML)—a rare presentation of apparent leukonychia1—were firstly described by Dr. Robert Muehrcke2 in 1956 in a subset of patients with hypoalbuminemia due to nephrotic syndrome and other causes. They are usually associated with periods of metabolic stress and hypoalbuminemia, such as those secondary to infections, severe malnutrition, chronic diseases (e.g. liver diseases, renal insufficiency, or pellagra) and chemotherapy drugs (most frequently doxorubicin and cyclophosphamide).1,3,4 Other causes not influenced by hypoalbuminemia have been proposed, such as ML induced by altitude in Mount Everest expeditions.5 ML typically fade with digital compression and are expected to disappear as long as the serum albumin levels increase.1
Leukonychia can be classified as true (an injury in the nail matrix leads to white bands that move with nail growth) or apparent (static white discoloration bands secondary to nail bed pathology).1 Mees’ lines are an example of true leukonychia, most notably secondary to arsenic trioxide poisoning, but also carbon monoxide, thallium, and chronic fluoride poisoning (fluorosis), infections (leprosy, tuberculosis, malaria, herpes zoster), Hodgkin lymphoma, acute myeloid leukemia, and chemotherapy.6-10 Unlike ML, Mees’ lines do not fade with digital compression, and they are expected to move along the nail growth. Besides ML, other examples of apparent leukonychia are Lindsay nails (also known as “half-and-half nails”) in uremic renal failure patients (normal proximal half and a brownish, discolored distal half-nail)9-12 and Terry nails in patients with congestive heart failure, cirrhosis, and adult-onset diabetes mellitus (white-colored proximal half and normal distal half).9,12 Beau’s lines can be described as white depressions parallel to the lunula as a result of direct damage to the nail matrix keratinocytes.1 This disruption can be caused by antimitotic drugs (most often taxanes),12 but also it can be related to any severe systemic illness.9 Interestingly, the width of the lines are strictly related to the severity and the temporal evolution of the underlying disease.10
The pictures above (Figure 1) refer to a 66-year-old woman with stage IV sarcoidosis who was diagnosed with locally advanced breast carcinoma, luminal B Her-2 negative subtype. She started neoadjuvant chemotherapy with doxorubicin and cyclophosphamide, but was unable to proceed with the treatment after the third cycle due to subsequent hospital admissions (the first one due to febrile neutropenia and the following two due to hospital-acquired pneumonia) with unfavorable evolution with chronic hypoxemic respiratory failure and prolonged hypoalbuminemia (<25 g/L; normal range 38-51 g/L). Chemotherapy was canceled; the patient was started on anastrozole and was proposed for mastectomy. Examining the patient’s fingernails during the third admission, we documented three non-palpable white bands parallel to the lunula separated by the natural pink nail. These findings are consistent with ML. Since the lines were not present before the cancer diagnosis and treatment, we believe chemotherapy played a major role in the pathophysiology, enhancing the effect of the tumor-induced hypoalbuminemia. In this clinical setting, sarcoidosis can be considered a relevant chronic comorbidity that is probably less related to ML, since there are no clear data in the literature supporting this connection.
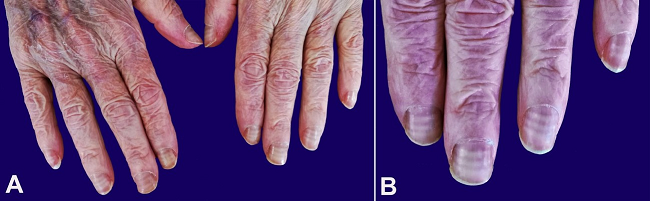
Figure 1
A- Muehrcke’s lines shown in the fingernails of both hands; B- Muehrcke’s lines in detail.
This manuscript was approved by the institution’s Ethics Committee after the patient signed an informed consent.
REFERENCES
1 Robert C, Sibaud V, Mateus C, et al. Nail toxicities induced by systemic anticancer treatments. Lancet Oncol. 2015;16(4):e181-9. http://dx.doi.org/10.1016/S1470-2045(14)71133-7. PMid:25846098
2 Muehrcke RC. The finger-nails in chronic hypoalbuminemia: a new physical sign. BMJ. 1956;1(4979):1327-8. http://dx.doi.org/10.1136/bmj.1.4979.1327. PMid:13316143
3 Brownson WC. An unusual condition of the nails in pellagra. South Med J. 1915;8(8):672-5. http://dx.doi.org/10.1097/00007611-191508000-00004
4 Morrison-Bryant M, Gradon JD. Images in clinical medicine: Muehrcke’s lines. N Engl J Med. 2007;357(9):917. http://dx.doi.org/10.1056/NEJMicm065055. PMid:17761595
5 Windsor JS, Hart N, Rodway GE. Muehrcke’s lines on Mt. Everest. High Alt Med Biol. 2009;10(1):87-8. http://dx.doi.org/10.1089/ham.2008.1079. PMid:19278357
6 Sharma S, Gupta A, Deshmukh A, Puri V. Arsenic poisoning and Mees’ lines. QJM. 2016;109(8):565-6. http://dx.doi.org/10.1093/qjmed/hcw068. PMid:27256460
7 Chauhan S, D’Cruz S, Singh R, Sachdev A. Mees’ lines. Lancet. 2008;372(9647):1410. http://dx.doi.org/10.1016/S0140-6736(08)61587-1. PMid:18940464
8 Anoun S, Qachouh M, Lamchahab M, Quessar A, Benchekroun S. Mees’ lines in an acute myeloyd leukemia patient. Turk J Haematol. 2013;30(3):340. http://dx.doi.org/10.4274/Tjh.2013.0048. PMid:24385821
9 Fawcett RS, Linford S, Stulberg DL. Nail abnormalities: clues to systemic disease. Am Fam Physician. 2004;69(6):1417-24. PMid:15053406
10 Singal A, Arora R. Nail as a window of systemic diseases. Indian Dermatol Online J. 2015;6(2):67-74. http://dx.doi.org/10.4103/2229-5178.153002. PMid:25821724
11 Yang CS, Robinson-Bostom L. Images in clinical medicine: Lindsay’s nails in chronic kidney disease. N Engl J Med. 2015;372(18):1748. http://dx.doi.org/10.1056/NEJMicm1406572. PMid:25923554
12 Minisini AM, Tosti A, Sobrero AF, et al. Taxane-induced nail changes: incidence, clinical presentation and outcome. Ann Oncol. 2003;14(2):333-7. http://dx.doi.org/10.1093/annonc/mdg050. PMid:12562663
Notes
Author notes
Correspondence Nuno Teixeira Tavares Serviço de Oncologia Médica - Centro Hospitalar de São João Alameda Prof. Hernâni Monteiro - Porto - Portugal CEP: 4200-319 Phone: +351 (22) 551 2100 nunoteixeiratavares@hotmail.com
Conflict of interest declaration
