Article / Clinical Case Report
Received: 11 April 2017
Accepted: 21 August 2017
DOI: https://doi.org/10.4322/acr.2018.009
Abstract: Odontomas are odontogenic tumors composed of a mixture of dental tissues. They are very common hamartomas of the jaws. However, their peripheral or gingival counterparts are extremely uncommon. The objective of this article is to report a rare case of gingival complex odontoma in an 11-year-old patient, and also to review all published cases of this type of lesion.
Keywords: Diagnosis, Oral, Odontogenic Tumors, Gingival, Odontoma.
INTRODUCTION
Odontomas are odontogenic tumors/hamartomas composed of dental tissue in a variable proportion. They are classically divided into compound or complex types, and are much more common in children and young adults. In most cases, odontomas are intraosseous and disturb the eruption of both permanent and deciduous teeth.1 In a few cases, they may erupt in the oral cavity.2 However, such lesions rarely develop completely within tooth-bearing soft tissues, but, in this case, they may be called gingival or peripheral odontomas.3
Gingival odontoma is almost never diagnosed as such when making a differential diagnosis of peripheral lesions. Given its rare occurrence, we thought it important to report the case of a gingival complex odontoma, and also considered it pertinent to review all published cases since the first report of this type of odontoma in 1989.
CASE REPORT
An 11-year-old white female patient was referred to the Stomatology clinic of the University of São Paulo, because of a painless nodular lesion on the palatal gingiva close to the incisive papilla. The nodule was sessile, smooth-surfaced, covered with normal colored mucosa, firm upon palpation and measured approximately 1.5 cm (Figure 1).

Figure 1
Clinical presentation showing a nodular lesion on the palatal aspect between maxillary left permanent central and lateral incisors.
The patient reported that the lesion had grown slowly over 2 years. The clinical hypothesis included peripheral ossifying fibroma and peripheral giant cell granuloma, and the patient was submitted to an excisional biopsy. The absence of bone erosion was confirmed through radiographic examination and during surgery.
In the course of gross examination, a hard consistency was noticed and the specimen was sent to be decalcified. The microscopic analysis revealed the presence of a rounded lesion within the lamina propria composed of randomly arranged dental tissues (Figure 2A). The tissues were mostly young, and composed of tubular dentin, cementum-like material and loosely arranged mesenchymal cells resembling dental papilla. The mass contained odontoblast-like cells adjacent to the dentin, small islands of odontogenic epithelium and few basophilic areas interpreted as enamel matrix. Foci of ghost cells were also observed (Figure 2B). The final diagnosis was peripheral complex odontoma.
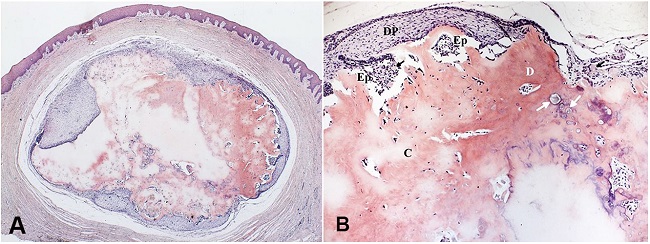
Figure 2
Photomicrograph of the excisional biopsy showing in A - a tumor composed of dental tissues within the lamina propria (H&E, 25X), and in B - mesenchymal cells loosely arranged resembling dental papilla (DP), odontogenic epithelium (Ep), cementum-like material (C), tubular dentin (D), enamel matrix (white arrows), and ghost cells (black arrows) (H&E, 100X).
The surgery site healed uneventfully, and the patient remains lesion-free after one year.
DISCUSSION
Odontogenic tumors make up a large group of neoplastic and developmental lesions originating from the odontogenic epithelium, the ectomesenchyme or both. Because tooth formation takes place within the jaw bones, it is reasonable to expect that the tumors developing there will be only intraosseous. Nevertheless, occasionally rests of dental lamina (rests of Serres) entrapped within gingival tissues may give rise to peripheral odontogenic tumors.4 There is still no consensus regarding what stimuli could activate the rests of dental lamina and initiate formation of a gingival odontoma.5 As the intraosseous counterpart of peripheral odontogenic tumors, gingival odontomas are also divided into compound or complex types, based upon their histopathological features.6-11 Some authors prefer to classify them as peripheral developing odontomas instead,12-14 a misused term since the lesion is hamartomatous by definition.
Microscopic analysis of our case revealed different amounts of dental tissue within the palatal gingiva, without any connection to underlying bone or overlying epithelium. Some pathologists may not feel very comfortable in distinguishing an epithelium-rich odontoma from an ameloblastic fibro-odontoma, due to their histological similarities. Indeed, most authors believe these lesions are different parts of the same spectrum that comprises a hamartomatous variant and a truly neoplastic ameloblastic fibroma.15 In this case, the dental tissues appeared well circumscribed and ball-shaped, closely resembling an intraosseous tumor. This arrangement served as strong evidence to establish the diagnosis as that of a peripheral odontoma, and not an ameloblastic fibro-odontoma.16 Moreover, our case failed to demonstrate enamel organ-like islands typically seen in fibro-odontoma.
Some authors also consider a supernumerary tooth as a different expression of the same pathological process that leads to odontoma.14,17 This histological appearance of a disorganized developing dental germ observed in both lesions could support such a hypothesis. However, even though this idea may be applicable to some situations, supernumeraries do not cause a slow growing mass, as was observed in this case report.
Gingival odontoma may also erupt in the oral cavity if left untreated.18 It is unclear if eruption is a trend for all cases, but it may be related to tumor growth over time or to local bone resorption.18 The absence of resorption noted during the surgery, and the distance between the tumor in relation to the surface epithelium strongly suggests that eruption would hardly come about in this patient.
Table 1 presents all the previously published diagnosed cases of this tumor. The research included the terms “peripheral odontoma”, “gingival odontoma” and “soft tissue odontoma” as key words in PUBMED, MEDLINE, COCHRANE and GOOGLE SCHOLAR databases, and resulted in 15 papers dating from 1989 to 2014. Four of them were available only at the public library of the University of São Paulo.6-9 We excluded one article from the list because its authors were unable to decide whether the tumor was a peripheral ameloblastic fibro-odontoma or an odontoma, even though they did present some evidence pointing to the latter.16 This article reflected how hard is to distinguish between these lesions, as discussed earlier.
Data from previously reported and present cases of gingival odontoma arranged by age
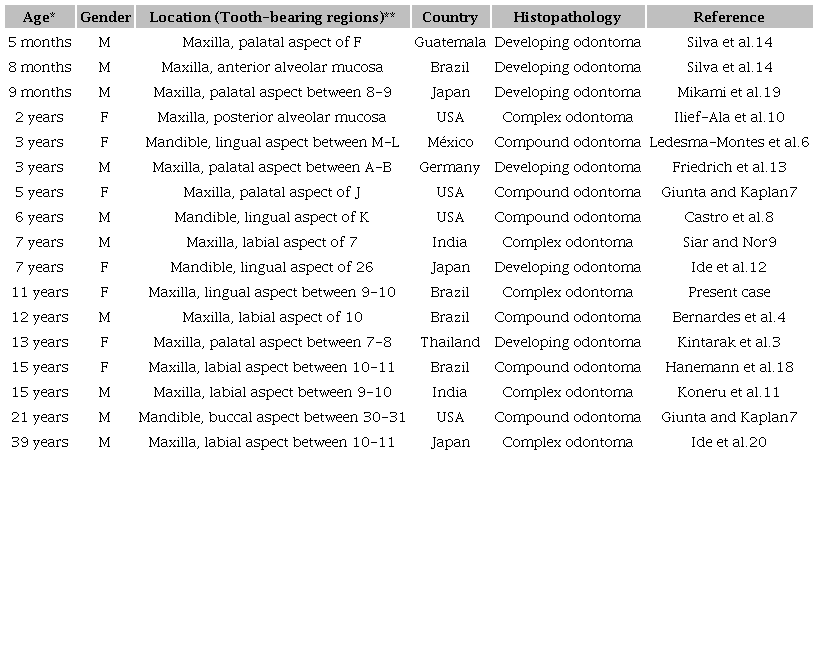
* Age at the first dental visit; ** Tooth identification number follows the Universal Numbering System.
Similar to the descriptions of most reports, the present case was asymptomatic and showed no recurrence after surgical removal. The patient’s age at the time of diagnosis was approximately two years older than the average age for gingival odontoma. Some of the listed tumors showed unusual characteristics, such as ghost cells seen during histopathological examination,4 adult involvement and association with a congenital teratomatous tumor.19,20 Foci of ghost cells were detected in these cases but their origin remains uncertain since these cells may appear in a variety of odontogenic tumors.
This is the fourth case reported in a Brazilian patient and the seventeenth case worldwide. We considered it relevant to report the present case, because it was an extremely rare odontogenic tumor, and enabled us to broaden our understanding of the clinicopathological features of this tumor.
INFORMED CONSENT
The informed consent was signed by the patient’s guardian.
REFERENCES
1 Cohen DM, Bhattacharyya I. Ameloblastic fibroma, ameloblastic fibro-odontoma, and odontoma. Oral Maxillofac Surg Clin North Am. 2004;16(3):375-84. 18088738 http://dx.doi.org/10.1016/j.coms.2004.03.005
2 Raval N, Mehta D, Vachhrajani K, Nimavat A. Erupted odontoma: a case report. J Clin Diagn Res. 2014;8(7):10-1. PMid:25177649
3 Kintarak S, Kumplanont P, Kietthubthew S, Chungpanich S. A nodular mass of the anterior palatal gingiva. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102(1):3-6. 16831665 http://dx.doi.org/10.1016/j.tripleo.2006.01.018
4 Bernardes VF, Cota LOM, Costa FO, Mesquita RA, Gomez RS. Gingival peripheral odontoma in a child: case report of an uncommon lesion. Brazilian J Oral Sci. 2008;7(26):1624-6.
5 Ide F, Obara K, Mishima K, et al. Peripheral odontogenic tumor: a clinicopathologic study of 30 cases: general features and hamartomatous lesions. J Oral Pathol Med. 2005;34(9):552-7. 16138894 http://dx.doi.org/10.1111/j.1600-0714.2005.00355.x.
6 Ledesma-Montes C, Perez-Bache A, Garcés-Ortíz M. Gingival compound odontoma. Int J Oral Maxillofac Surg. 1996;25(4):296-7. 8910117 http://dx.doi.org/10.1016/S0901-5027(06)80061-5.
7 Giunta JL, Kaplan MA. Peripheral, soft tissue odontomas: two case reports. Oral Surg Oral Med Oral Pathol. 1990;69(3):406-11. 2314871 http://dx.doi.org/10.1016/0030-4220(90)90312-G.
8 Castro GW, Houston G, Weyrauch C. Peripheral odontoma: report of case and review of literature. ASDC J Dent Child. 1994;61(3):209-13. PMid:8089351
9 Siar CH, Nor GM. Peripheral complex odontome with ghost cell epithelium: a case report. Ann Dent. 1989;48(2):6-7. PMid:2604374
10 Ilief-Ala MA, Eisenberg E, Mathieu G. Peripheral complex odontoma in a pediatric dental patient: a case report. J Mass Dent Soc. 2008;56(4):24-6. PMid:18459673
11 Koneru A, Surekha R, Vanishree M, Hamsini A, Hunasgi S. Rare gingival odontoma: report of a case and review of literature. J Dr NTR Univ Heal Sci. 2014;3(2):133-5. http://dx.doi.org/10.4103/2277-8632.134889
12 Ide F, Mishima K, Saito I, Kusama K. Rare peripheral odontogenic tumors: report of 5 cases and comprehensive review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106(4):e22-8. 18718792 http://dx.doi.org/10.1016/j.tripleo.2008.05.064
13 Friedrich RE, Fuhrmann A, Scheuer HA, Zustin J. Small peripheral developing odontoma of the maxilla in a 3-year-old patient depicted on cone-beam tomograms. In Vivo. 2010;24(6):895-8. PMid:21164051
14 Silva AR, Carlos-Bregni R, Vargas PA, Almeida OP, Lopes MA. Peripheral developing odontoma in newborn: report of two cases and literature review. Med Oral Patol Oral Cir Bucal. 2009;14(11):e612-5. 19680201 http://dx.doi.org/10.4317/medoral.14.e612
15 Buchner A, Vered M. Ameloblastic fibroma: a stage in the development of a hamartomatous odontoma or a true neoplasm? Critical analysis of 162 previously reported cases plus 10 new cases. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;116(5):598-606. 24055148 http://dx.doi.org/10.1016/j.oooo.2013.06.039
16 Reibel J, Grønbaek AB, Poulsen S. Peripheral ameloblastic fibro-odontoma or peripheral developing complex odontoma: report of a case. Int J Paediatr Dent. 2011;21(6):468-70. 21689175 http://dx.doi.org/10.1111/j.1365-263X.2011.01144.x.
17 Pippi R. Odontomas and supernumerary teeth: is there a common origin? Int J Med Sci. 2014;11(12):1282-97. 25419174 http://dx.doi.org/10.7150/ijms.10501
18 Hanemann JAC, Oliveira DT, Garcia NG, Santos MRG, Pereira AAC. Peripheral compound odontoma erupting in the gingiva. Head Face Med. 2013;9(1):15. 23758697 http://dx.doi.org/10.1186/1746-160X-9-15
19 Mikami T, Yagi M, Mizuki H, Takeda Y. Congenital peripheral developing odontoma accompanied by congenital teratomatous fibroma in a 9-month-old boy: a case report. J Oral Sci. 2013;55(1):89-91. 23485607 http://dx.doi.org/10.2334/josnusd.55.89
20 Ide F, Shimoyama T, Horie N. Gingival peripheral odontoma in an adult: case report. J Periodontol. 2000;71(5):830-2. 10872967 http://dx.doi.org/10.1902/jop.2000.71.5.830
Notes
Author notes
Correspondence Marcos Custódio Department of Oral and Maxillofacial Pathology - School of Dentistry - University of São Paulo (USP) Av. Prof. Lineu Prestes, 2227 - São Paulo/SP - Brazil CEP: 05508-000 Phone: +55 (11) 3091-7902 marcosjcustodio@usp.br
Conflict of interest declaration
