Article / Autopsy Case Report
Spontaneous perforation of small intestine followed by rupture of the cystic artery: the natural history of Vascular Ehlers-Danlos Syndrome
Spontaneous perforation of small intestine followed by rupture of the cystic artery: the natural history of Vascular Ehlers-Danlos Syndrome
Autopsy and Case Reports, vol. 9, no. 1, e2018054, 2019
Hospital Universitário da Universidade de São Paulo
Received: 12 September 2018
Accepted: 27 September 2018
ABSTRACT: Vascular Ehlers-Danlos Syndrome (VEDS) is a rare autosomal dominant disorder caused by mutations in the COL3A1 or COL1A1 genes. Its mortality is secondary to sudden and spontaneous rupture of arteries or hollow organs. The genotype influences the distribution of arterial pathology with aneurysms of intra-abdominal visceral arteries being relatively uncommon. We describe the case of a young man with probable VEDS who died of a spontaneous rupture and dissection of the cystic artery. The patient initially presented with abdominal pain due to an unrecognized spontaneous perforation of the small intestine complicated by sepsis. We postulate that inflammatory mediators may have triggered the arterial rupture due to remodeling and weakening of vessel walls. The phenotype of the patient’s vascular damage included bilateral spontaneous carotid-cavernous sinus fistulae and dissection with pseudoaneurysm formation of large- and medium-sized arteries, predominantly the abdominal aorta and its branches. The autopsy uncovered a long history of vascular events that may have been asymptomatic. These findings along with a positive family history supported the VEDS diagnosis. Loeys-Dietz, Marfan, and familial thoracic aortic aneurysm and dissection syndromes were ruled out based on the absence of arterial tortuosity, eye abnormalities, bone overgrowth, and the distribution of vascular damage among other features. Interestingly, microscopic examination of the hippocampus revealed a focus of neuronal heterotopia, commonly associated with epilepsy; however, the patient had no history of seizures. The natural course of VEDS involves the rupture and dissection of arteries that, if unrecognized, can lead to a rapid death after bleeding into free spaces.
Keywords: Aneurysm, Aneurysm, False, Ehlers-Danlos Syndrome, Intestinal Perforation, Aneurysm, Dissecting.
CASE REPORT
A 30-year-old man complained of left lower abdominal pain associated with nausea and vomiting. The medical history included aneurysms of the abdominal aorta and some of its branches, a surgically repaired pseudoaneurysm of the left subclavian artery, a coil embolization of the superior ophthalmic vein, right and left cavernous sinuses and recent coil embolization of an aneurysm of the splenic artery. His father had also developed multiple aneurysms. Physical examination revealed tenderness with guarding of the lower abdomen. Laboratory results on admission were relevant for normal hemoglobin (15.1 g/dL, reference range [RR]; 12,16 g/dL) and a white blood cell count of 8,800 cells/mm3 (RR; 4,800-10,800/mm3) with 84.2% neutrophils. An abdominal CT scan revealed ascites and changes consistent with prior aneurysms. In a repeat CT, there was a right pleural effusion and nonspecific enteritis involving small bowel loops in the left abdomen and descending colon. The clinical diagnosis was an intestinal obstruction, which improved after the placement of a nasogastric tube.
On hospitalization day 7, the patient remained in stable condition with normal hematologic and clinical chemistry parameters; however, an abdominal X-ray still showed persistent dilation of small bowel loops. General and vascular surgery recommended medical management. On hospitalization day 11, he developed fever and leukocytosis associated with a sudden drop in hemoglobin to 6.5 g/dL. Right thoracentesis collected hazy pleural fluid. Later that night, the patient developed respiratory distress and increased abdominal pain, and expired.
AUTOPSY PRESENTATION
The postmortem period was 24 hours. On external examination, the skin was pale and elastic. There were widened atrophic scars in the left paratracheal and supraclavicular regions from prior surgical procedures. There were no apparent deformities of the axial or appendicular skeleton. On internal examination, there were bilateral serous pleural effusions (right, 150 mL; left, 50 mL). The visceral pleura exhibited numerous fibrous adhesions to the chest wall and pericardium, bilaterally. The pericardial sac was dry. There was hemoperitoneum, 900 mL of blood and 910 mL of clots. Fibrous and fibrinous adhesions between loops of small intestine and abdominal wall were present in the lower abdominal cavity associated with a 5-cm area of serosal purulent exudate. There was a perforation of the small intestine (Figure 1).
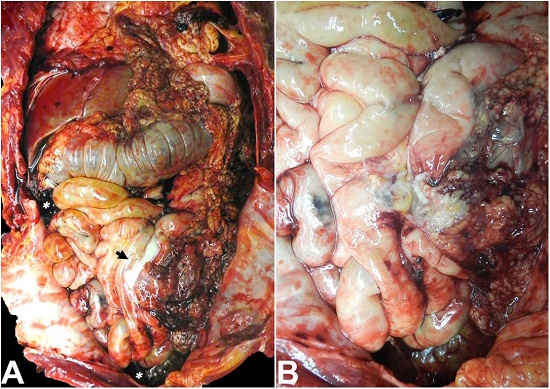
Figure 1
Abdominal cavity, after lifting up the greater omentum, with evidence of intestinal perforation. A - Purulent exudate in small intestinal loops (black arrow) with adhesions, and hemoperitoneum (white asterisks); B - Extensive small bowel edema, purulent exudate, and focal hemorrhage of mesenteric fat.
The remainder of the small and large intestines exhibited thin and translucent walls with loss of mucosal folds and reduced circumference. An area of fresh soft tissue hemorrhage tracked down to the gallbladder neck and hepatic hilum. Careful dissection and microscopic examination of the gallbladder neck revealed rupture and dissection of the cystic artery (Figure 2, 3 and 4).

Figure 2
Rupture and dissection of the cystic artery. Note the soft tissue hemorrhage around the gallbladder neck (arrow). Bar: 1 cm.
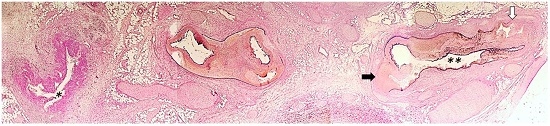
Figure 3
Photomicrograph of the cystic duct (one asterisk), and cystic artery (two asterisks) showing dilatation, rupture (black arrow), and a dissecting track with double lumen formation (white arrow), (Verhoeff’s stain, 25x).
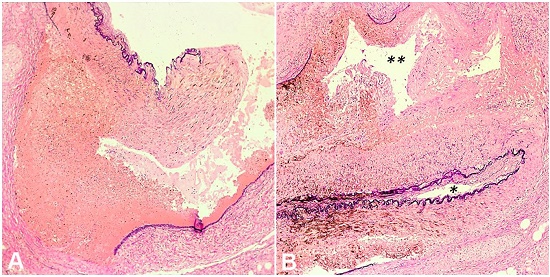
Figure 4
Photomicrographs of the cystic artery. A - Disruption of the elastic lamina of the cystic artery at point of rupture with blood extravasation, (Verhoeff’s stain, 200x); B - Dissecting track between the arterial adventitia and media with double lumen formation. True lumen demarcated by the inner elastic lamina (one asterisk). False lumen located between the inner and outer elastic laminae (two asterisks) (Verhoeff’s stain, 200x).
The pancreaticobiliary tree was unremarkable. The liver weighed 1010 g (RR; 1500-1800 g) and showed hepatocellular cholestasis, mild steatosis, and scattered glycogenated nuclei. There was also mild portal inflammation and mild siderosis on iron stains.
The heart weighed 240 g (RR; 270-360 g) and showed thin atrial walls and a 2.5-centimeter subendocardial hemorrhage within the septal wall of the left ventricle consistent with resuscitation efforts. The coronary arteries displayed normal courses and no evidence of atherosclerosis or thrombosis. The infrarenal segment of the abdominal aorta exhibited a 4-cm pseudoaneurysm associated with a 2.3-cm intraluminal endothelialized band (Figure 5). The right common iliac artery was dilated, dissected and focally calcified, measuring 2.6 cm in diameter. There were pseudoaneurysms of the left common and internal iliac arteries containing old thrombi, each measuring 2.3 cm in diameter. The left external iliac artery exhibited a 1.8 cm calcified pseudoaneurysm. A 1.1 cm coiled pseudoaneurysm was present in the splenic artery. Microscopic examination revealed evidence of prior dissection of the aorta and its distal terminal branches by elastin stains (Figure 5).
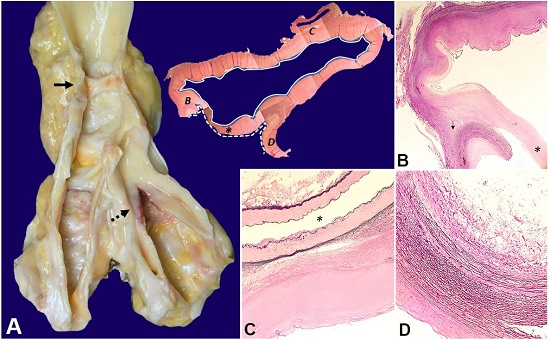
Figure 5
Pathology of the abdominal aorta and iliac arteries. A - Posteriorly opened abdominal aorta with aneurysm and an endothelialized intraluminal band (solid arrow), and dissection and dilation of the iliac arteries with calcifications and hemorrhage (dashed arrow). Composite H&E images of cross-section at the level of endothelialized intraluminal band (asterisk) showing a false lumen or dissecting track (continuous line), and a true lumen (discontinuous line), on the top right; B - Point of cleavage between the adventitia and media (arrow) adjacent to the endothelialized intraluminal band (asterisk) (Verhoeff’s stain, 50x); C - False lumen lined by fibrin and fibrous tissue devoid of elastin fibers, which are conserved in the inferior mesenteric artery (asterisk) (Verhoeff’s stain, 100x); D - Vascular wall delimiting the true lumen with preservation of elastic fibers of the medial layer and intimal thickening (Verhoeff’s stain, 100x).
The thoracic aorta was unremarkable. The renal arteries exhibited intimal fibrosis and mild myxoid changes. The right renal artery measured approximately three times the size of the left renal artery.
The right lung weighed 415 g (RR; 360-570 g) and showed atelectasis and congestion in the upper lobe. Microscopically, the right pleura appeared markedly thickened with granulation tissue, fibrosis, fibrin deposition, and focal acute inflammation. The left lung weighed 275 g (RR; 325-480 g) and appeared shrunken with atelectasis and congestion in the lower lobe. There was no evidence of pulmonary thromboemboli. The brain weighed 1530 g (RR; 1100-1700 g) and showed signs of mild hypoxic-ischemic damage as well as a focus of neuronal heterotopia in the hippocampus (Figure 6).
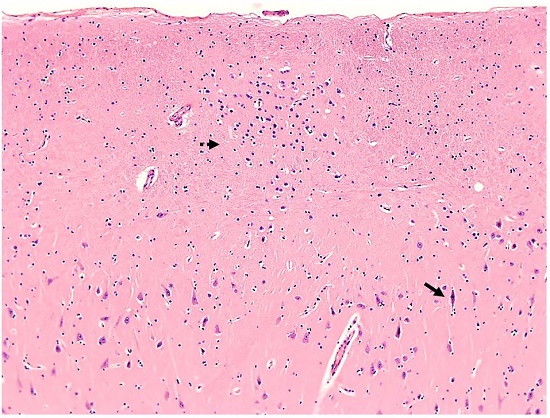
Figure 6
Photomicrograph of the hippocampus. Cornu Ammonis-1 (CA1) showing a focus of neuronal heterotopia in the stratum moleculare (dashed arrow) and red neurons in the hippocampal pyramidal layer (solid arrow) (H&E, 100x).
Metallic coils were present in the cavernous sinuses, bilaterally. There was congestive splenomegaly (230 g (RR; 150-200 g)). The bone marrow was normocellular with trilineage hematopoiesis. The adrenal glands were lipid-depleted consistent with an acute stress reaction. The kidneys and other genitourinary organs were grossly and microscopically unremarkable. Postmortem cultures of the serosal intestinal exudate were positive for Escherichia coli and Enterococcus species. Lung and blood cultures were negative. No toxicology tests were performed.
CLINICAL DISCUSSION
The differential diagnosis of conditions causing pseudoaneurysms is complex. An aneurysm is defined as a localized permanent pathologic dilation of a vessel with a diameter at least 50% larger than the expected normal diameter of the vessel in question. While in a true aneurysm all vascular layers are present, a pseudoaneurysm (false aneurysm) is delineated by only adventitia, periadventitial connective tissue or healed fibrous tissue. Interestingly, pseudoaneurysms may form after rupturing of true aneurysms and even replace them.1 Elastin stains help differentiate both types by demonstrating elastic fibers in the medial layer, and outer and inner elastic laminae in arteries. The distinction is relevant for accurate pathologic diagnosis. Hypertension, atherosclerosis, and inflammatory aortitis are the leading etiologies of aortic aneurysms.2 In these conditions, pressure or ischemia-related injury and destruction of the vasa vasorum causes degenerative changes of components of the vascular wall leading to progressive dilation and increased risk of rupture. On the other hand, a spontaneous rupture with dissection is the most common mechanism for pseudoaneurysm formation. Hypertension accounts for approximately 90% of aortic dissections, especially in older men, while inherited or acquired connective tissue disorders are more common in younger patients.2
In the case described herein, a young adult man presented with spontaneous perforation of the small intestine that was followed by fatal dissection and rupture of the cystic artery. The phenotype of his vascular disease included bilateral spontaneous carotid-cavernous sinus fistulae and dissection with pseudoaneurysm formation of large- and medium-sized arteries, predominantly the abdominal aorta and its branches. Because of his age, family history and the absence of conventional cardiovascular risk factors, an inherited disease is the most plausible explanation for his clinical presentation. Hereditary diseases involving dissecting pseudoaneurysms of the aorta include abnormalities in extracellular matrix proteins such as Marfan syndrome and Ehlers-Danlos syndrome (EDS), smooth muscle cytoskeleton proteins, components of the transforming growth factor (TGF)-beta(β) signaling pathway, and metabolic disorders such as Fabry disease, polycystic kidney disease among others. Craniofacial developmental malformations and some immunological derangements such as allergies and inflammatory bowel disease have also been associated with an increased risk of aortic dissection.3
The autopsy findings along with the family history are consistent with the natural history of vascular type EDS (VEDS) although no confirmatory genetic testing was performed. VEDS is caused by mutations in the COL3A1 gene and more rarely in COL1A1, which are inherited in an autosomal dominant pattern. According to the Ehlers-Danlos Society, the most recent 2017 international diagnostic criteria includes: 1) family history of VEDS with documented causative mutation in COL3A1; 2) arterial rupture at a young age; 3) spontaneous intestinal perforation in the absence of other bowel pathology; 4) uterine rupture in the absence of previous C-section; and 5) carotid-cavernous sinus fistula formation in the absence of trauma.4 We identified four major criteria sufficient to diagnose VEDS. Minor criteria including thin translucent skin, characteristic facial appearance (thin face, large appearing eyes, thin lips, thin nose), acrogeria, hypermobility of small joints, tendon and muscle rupture, talipes equinovarus, early onset varicosities, and gingival recession are subjective and difficult to evaluate post-mortem. Because some forms of Loeys-Dietz syndrome, Marfan syndrome, and familial arterial aneurysm and dissection syndromes exhibit overlapping features with VEDS, a definitive diagnosis may require confirmation by gene sequencing, deletion/ duplication testing, or analysis of type III procollagen in cultures of fibroblasts.4 Loeys-Dietz syndrome is caused by mutations in TGF-β pathway genes and is characterized by arterial tortuosity and aneurysms, hypertelorism, and bifid uvula. The primary features of the Marfan syndrome are eye abnormalities including dislocated lenses, bone overgrowth and laxity, and aortic enlargement. These defects were all absent in our patient. Moreover, the vascular damage observed in Marfan, as well as familial thoracic aortic aneurysm and dissection syndromes, are limited to heart and large vessels.5
Individuals with VEDS have significantly shortened life spans with a median survival of 48 years (range, 6 to 73 years) due to the spontaneous rupture of blood vessels and visceral organs.4 These complications are uncommon during childhood. The most common first and second complication is an arterial rupture, even after a first gastrointestinal complication. The lethality after rupture of any artery tends to be higher if there is bleeding into a free space in comparison to bleeding into a confined space that may be sealed because of tamponade. Aneurysms of intra-abdominal visceral arteries are relatively uncommon in VEDS.6 There are reports of spontaneous rupture of the splenic, hepatic, superior mesenteric, pancreaticoduodenal, and renal arteries.7 To our knowledge, this is the first report of spontaneous rupture of the cystic artery in VEDS. The genotype influences the distribution of arterial pathology.8,9 Missense and in-frame shift mutations lead to the production of a minimal amount of normal collagen (10-15%), while nonsense and frameshift mutations cause haploinsufficiency leading to a mild to moderate reduction of normal collagen (50%). In a cohort study, 68 individuals were classified into two groups based on the type of COL3A1 mutations and their effect on the amount of normal collagen.8 Patients with higher production of normal collagen presented with more aortic involvement and late onset of disease compared to patients with a severe decrease (56% vs. 21%). On the other hand, visceral arterial involvement and early onset of disease were more common in patients with a severe decrease in the production of normal collagen.9
Perforation, spontaneous or iatrogenic, of intraabdominal viscera, is the second most common complication in VEDS. The most frequent anatomical location is the sigmoid colon.4 However, perforation of small intestine often occurs secondary to diverticula. Intramural vascular rupture with hematoma formation increases the risk of necrosis of the intestinal wall, which also may lead to perforation.10 Of note, perforation of the small intestine in our patient preceded the rupture of the cystic artery. Formation and expansion of aneurysms have been associated with inflammation and tissue degradation.11-13 It is possible that chronic or acute inflammatory events increase the risk of vessel rupture in VEDS; although, this needs to be confirmed.
Unexpectedly, a focus of neuronal heterotopia was identified during routine microscopic examination of the hippocampus in association with neurons depicting hypoxic/ ischemic damage (i.e. “red dead neurons”) as shown in Figure 6. Of interest, central nervous system disorders and epilepsy can accompany EDS.14,15 Structural abnormalities of the central nervous system appear to be the cause of seizures. It has been suggested that seizures may originate in areas of heterotopic neurons. Abnormal neuronal positioning in VEDS can be related to defects in extracellular matrix and disruption in cellular adhesion affecting neuronal migration.14 There is no apparent correlation between the extent and severity of the neuronal heterotopia and frequency of seizures. Despite the presence of neuronal heterotopia, our patient did not have a history of epilepsy or seizures. Therefore, the significance of this finding is unknown and requires further investigation.
CONCLUSION
In conclusion, we describe the case of a man with VEDS presenting with intestinal perforation followed by a lethal and spontaneous rupture of the cystic artery. Spontaneous rupture of vessels, mainly large- and medium-sized arteries, and internal organs are responsible for the high mortality seen in young people with VEDS. Patients with this rare collagen disorder may survive several vascular events that might be asymptomatic, leading to progressive destruction of vessel walls, aneurysm formation, rupture, and dissection. In many instances, the triggering factor for the vessel rupture is unknown, but herein we found that an intestinal perforation preceded it. This sequence of events can be explained by the inflammatory effects of sepsis leading to remodeling and weakening of vessel walls. The natural course of VEDS involves the rupture and dissection of arteries that can lead to immediate death if there is bleeding into free spaces.
REFERENCES
Nomura M, Mori K, Tamase A, et al. Pseudoaneurysm formation due to rupture of intracranial aneurysms: case series and literature review. Neuroradiol J. 2017;30(2):129-37. http://dx.doi.org/10.1177/1971400916684667. PMid:28059632
Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. J Am Coll Cardiol. 2010;55(14):e27-129. http://dx.doi.org/10.1016/j.jacc.2010.02.015. PMid:20359588
Bradley TJ, Bowdin SC, Morel CF, Pyeritz RE. The expanding clinical spectrum of extracardiovascular and cardiovascular manifestations of heritable thoracic aortic aneurysm and dissection. Can J Cardiol. 2016;32(1):86-99. http://dx.doi.org/10.1016/j.cjca.2015.11.007. PMid:26724513
Byers PH, Belmont J, Black J, et al. Diagnosis, natural history, and management in vascular Ehlers-Danlos syndrome. Am J Med Genet C Semin Med Genet. 2017;175(1):40-7. http://dx.doi.org/10.1002/ajmg.c.31553. PMid:28306228
Meester JAN, Verstraeten A, Schepers D, Alaerts M, Van Laer L, Loeys BL. Differences in manifestations of Marfan syndrome, Ehlers-Danlos syndrome, and Loeys-Dietz syndrome. Ann Cardiothorac Surg. 2017;6(6):582-94. http://dx.doi.org/10.21037/acs.2017.11.03. PMid:29270370
Parfitt J, Chalmers RT, Wolfe JH. Visceral aneurysms in Ehlers-Danlos syndrome: case report and review of the literature. J Vasc Surg. 2000;31(6):1248-51. http://dx.doi.org/10.1067/mva.2000.105667. PMid:10842163
Chadha M, Ahuja C. Visceral artery aneurysms: diagnosis and percutaneous management. Semin Intervent Radiol. 2009;26(3):196-206. http://dx.doi.org/10.1055/s-0029-1225670. PMid:21326564
Shalhub S, Black JH 3rd, Cecchi AC, et al. Molecular diagnosis in vascular Ehlers-Danlos syndrome predicts pattern of arterial involvement and outcomes. J Vasc Surg. 2014;60(1):160-9. http://dx.doi.org/10.1016/j.jvs.2014.01.070. PMid:24650746
Frank M, Albuisson J, Ranque B, et al. The type of variants at the COL3A1 gene associates with the phenotype and severity of vascular Ehlers-Danlos syndrome. Eur J Hum Genet. 2015;23(12):1657-64. http://dx.doi.org/10.1038/ejhg.2015.32. PMid:25758994
Burcharth J, Rosenberg J. Gastrointestinal surgery and related complications in patients with Ehlers-Danlos syndrome: a systematic review. Dig Surg. 2012;29(4):349-57. http://dx.doi.org/10.1159/000343738. PMid:23095510
Torra R, Cases A, Trilla A, Ordi J, López J, Revert L. Fatal rupture of a mycotic aneurysm of the subclavian artery: an unusual complication of methicillin-resistant Staphylococcus-aureus-related sepsis. Nephrol Dial Transplant. 1994;9(1):114-5. PMid:8177470
Morissette R, Schoenhoff F, Xu Z, et al. Transforming growth factor-β and inflammation in vascular (type IV) Ehlers-Danlos syndrome. Circ Cardiovasc Genet. 2014;7(1):80-8. http://dx.doi.org/10.1161/CIRCGENETICS.113.000280. PMid:24399159
Newby D, Forsythe R, McBride O, et al. Aortic wall inflammation predicts abdominal aortic aneurysm expansion, rupture, and need for surgical repair. Circulation. 2017;136(9):787-97. http://dx.doi.org/10.1161/CIRCULATIONAHA.117.028433. PMid:28720724
Verrotti A, Monacelli D, Castagnino M, Villa MP, Parisi P. Ehlers-Danlos syndrome: a cause of epilepsy and periventricular heterotopia. Seizure. 2014;23(10):819-24. http://dx.doi.org/10.1016/j.seizure.2014.07.014. PMid:25131162
Cortini F, Villa C. Ehlers-Danlos syndromes and epilepsy: an updated review. Seizure. 2018;57:1-4. http://dx.doi.org/10.1016/j.seizure.2018.02.013. PMid:29499446
Notes
Author notes
Correspondence Christopher Antonio Febres-Aldana AM Rywlin M.D. Department of Pathology and Laboratory Medicine - Mount Sinai Medical Center 4300 Alton Rd, 33140 - Miami Beach/FL - United States of America Phone: +1 (305) 674-2277 christopher.febres@msmc.com
Conflict of interest declaration