Article / Clinical Case Report
Primary colonic liposarcomatosis: report of a case with review of literature
Primary colonic liposarcomatosis: report of a case with review of literature
Autopsy and Case Reports, vol. 9, no. 1, e2018056, 2019
Hospital Universitário da Universidade de São Paulo
Received: 12 August 2018
Accepted: 18 September 2018
ABSTRACT: The colon is a rare site of occurrence of liposarcoma, as either the primary site or by secondary involvement from a retroperitoneal liposarcoma. Liposarcomatosis denotes simultaneous occurrence of multiple liposarcomas. There are only 17 cases of primary colonic liposarcoma reported in the English literature—one of which was primary colonic liposarcomatosis. We depict the second case of primary colonic liposarcomatosis in a 57-year-old female who presented with abdominal swelling and pain. On exploratory laparotomy, two large masses were seen arising from the wall of the right colon along with multiple smaller masses attached to the colon. Right hemicolectomy with en bloc excision of the masses was performed along with hysterectomy and pelvic floor repair. Macroscopically, multiple exophytic masses and one endophytic mass were identified. The exophytic masses were of variable size and were found to hang from the colon by a thin pedicle simulating variable-sized appendices epiploicae. Histopathologically, the lesions showed the morphology of well-differentiated liposarcoma. This appears to be a case of primary colonic liposarcomatosis. There is only one other similar case reported in the English literature, to the best of our knowledge.
Keywords: Liposarcoma, Colonic Neoplasms, Proto-Oncogene Proteins c-mdm2.
INTRODUCTION
Liposarcoma is generally a slow growing, heterogeneous, locally aggressive tumor, which usually becomes symptomatic when the size of the tumor increases to a large extent. Histologically, liposarcoma is subdivided into well-differentiated, dedifferentiated, myxoid/round cell, or pleomorphic types.1 Rarely, the well-differentiated/dedifferentiated morphology can coexist with myxoid/round cell type or pleomorphic type.2 Liposarcomatosis is characterized by the synchronous presence of multiple liposarcomas. Liposarcoma generally occurs in the axial skeleton, limbs, retroperitoneum (RP), and spermatic cord. Searching on PubMed and using the uniterms “primary colonic liposarcomatosis,” “primary colonic liposarcoma,” “colonic liposarcoma,” and “colon, liposarcoma,” we found 17 cases of primary colonic liposarcoma reported in the English literature. Most of the previously reported cases of primary colonic liposarcoma presented as solitary endoluminal masses arising from the submucosal adipocytes. However, only a few cases showed single large pedunculated exophytic masses.3 Primary colonic liposarcomatosis is even rarer than liposarcoma, and only one case of primary colonic/mesenteric liposarcomatosis is described in the English literature.4 We describe a case of primary colonic liposarcomatosis where both endoluminal and exophytic growths were noted. Grossly and histomorpholgically, the exophytic growths appeared to arise from the appendices epiploicae with a spectrum of liposarcomatous transformation. Individual liposarcoma was well differentiated. We believe that this is the second case of primary colonic liposarcomatosis.
CASE REPORT
A 57-year-old female presented with an abdominal swelling over the last 6 months, and pain during the last 2 months. She also had a prolapsed uterus, which was diagnosed 3 months ago. She had no co-morbidities. A history of radiation exposure or any previous surgery was absent. On examination, a large abdominopelvic lump was palpable, measuring about 25 cm in diameter. The lower border of the mass could not be felt. Routine investigations were within normal limits. The contrast-enhanced computed tomography (CECT) of the abdomen and pelvis scan showed a large abdominopelvic mass with homogeneous density and enhancement, predominantly on the right side, displacing the small bowel and urinary bladder to the left. The abdominal and pelvic CECT scan showed a large abdominopelvic mass with homogeneous density and enhancement after contrast injection, predominantly on the right side, displacing the small bowel and the urinary bladder to the left. The CECT also showed multiple small lesions in the abdomen, with a large right iliac mass abutting the right iliac vessels (Figures 1A and 1B). There was no bowel or any other visceral infiltration. The imaging findings were consistent with the diagnosis of a retroperitoneal liposarcoma.
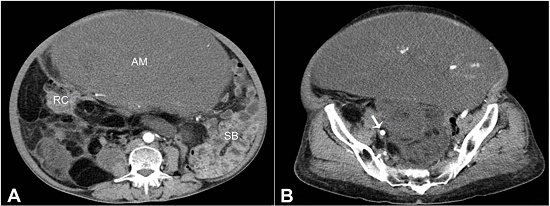
Figure 1
Abdominal computed tomography (CT) (axial plane). A - An abdominopelvic mass (AM) occupying almost whole of the abdominal cavity. The small bowel (SB) is displaced to the left, while the right colon (RC) is abutted against the paracolic gutter; B - Pelvic CT (axial plane) showing right iliac vessels (arrow) adherent to the soft tissue mass.
On exploratory laparotomy, there was minimal free fluid in the abdominal cavity. A multilobulated soft tissue tumor measuring approximately 20 × 15 cm was seen arising probably from the mesentery or from the bowel wall of the right colon. Another mass measuring 8 × 6 cm was seen in the right iliac fossa abutting the iliac vessels (Figure 2). Multiple nodules of up to 3 cm were seen in the entire abdomen, and they appeared to be attached to the colon.
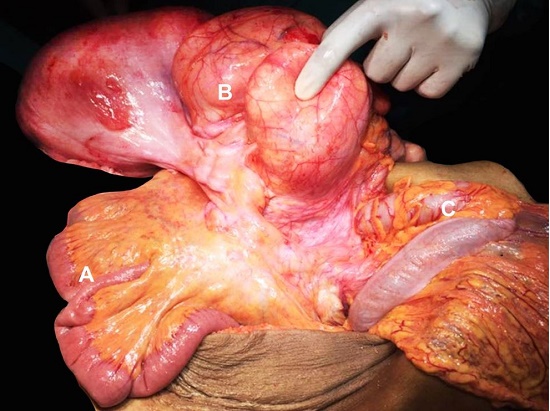
Figure 2
Intraoperatively view of the mass possibly arising from the right colon mesentery or the bowel wall of the right colon. A - Distal ileum; B - Multilobulated soft tissue tumor; C - Transverse colon.
The patient underwent a right hemicolectomy with en bloc excision of the mass, excision of right iliac fossa mass with hysterectomy and pelvic floor repair. The postoperative period was uneventful. The patient is currently doing well (3 months post-surgery) and is on regular follow-up. The excised mass was sent for histopathology.
The right hemicolectomy specimen included part of the terminal ileum, the cecum, the appendix, the ascending colon, and the proximal part of the transverse colon. The respective lengths of the parts of bowel were 13.5 cm (terminal ileum), 5 cm (cecum), 8.5 cm (appendix) and 14 cm (rest of the colon). The same container contained the en bloc mass along with multiple separately lying nodules. The en bloc resected specimen showed multiple nodules and exophytic masses attached to and hanging from the colon. Most of the masses were found to hang by a tiny pedicle, simulating appendices epiploicae of variable size, while only a few appeared not to have any stalk. These nodules and masses ranged in size from 1 cm to 22.5 × 16.5 x 10 cm in its largest dimension. The cut surfaces of the smaller nodules were fatty and yellow with thin strands of fibrous septa dividing these nodules into fatty lobules. The thickness of the septa was greater in the larger nodules, and the even larger ones showed a grayish white and dominantly fibrous cut surface with only a few interspersed fat lobules. In places, the larger masses showed indentation/cleavage, and these areas appeared to be the zone of fusion of two or more adjacent exophytic masses, and the cut surfaces of such masses showed the same (Figure 3).

Figure 3
Gross view of the specimen after formalin fixation with multiple fatty to solid gray pedunculated masses some of which appeared to arise from the coalescence of the smaller nodules (black arrowhead). Note the variable sizes of these pedunculated (exophytic masses) (white arrowheads); one mass was endophytic (black arrow) projecting within the cecal lumen. The white arrow highlights the ileocecal valve; the black star highlights the external aspect of the largest exophytic mass.
It appeared to be the coalescence of multiple adjacent appendices. The largest nodules showed central myxoid areas and scattered calcific specks. All these masses appeared to arise from the appendices on gross morphology. In addition, the cecum showed a bulge measuring 2.4 × 0.8 × 0.6 cm, and on cutting open showed a mass with a fibrofatty cut surface protruding into the cecum. No mucosal pathology was noted.
The specimen was extensively sampled to demonstrate the pathology, and a spectrum of pathological changes was documented. The smallest nodules (both attached and freely floating) showed multiple lobules of mature adipocytes with thin fibrous septa. The larger the masses, the more the thickness, complexity, number of septa, and number of septal and atypical adipocytic cells and lipoblasts increased (Figures 4A-4C and 5). The large nodules showed only a few lobules of mature fat and dominantly fibrocollagenous areas, giving rise to a sclerosing pattern (Figure 5). The largest nodule showed well-differentiated morphology with central areas of myxoid degeneration and atypical spindle cells in a myxoid matrix (Figure 6).
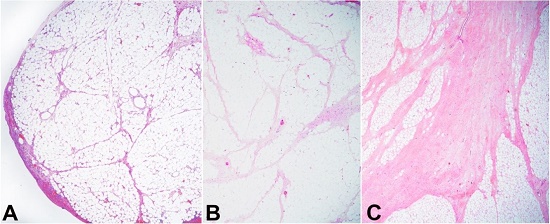
Figure 4
Photomicrographs of the appendices epiploicae of different size from smallest to the largest with gradual increase in the septal thickness and complexity (A-C), with the smallest one showing essentially normal morphology (A) and the larger one displaying thick septa (C).
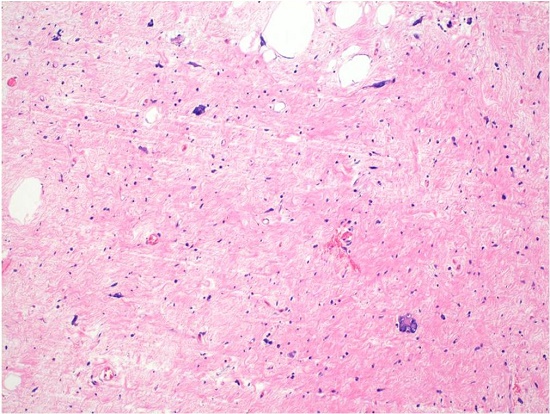
Figure 5
The largest of the appendices showed a sclerosing phenotype with occasional lobules of fat (H&E, 100X). The hyperchromatic atypical stromal cells are evident.
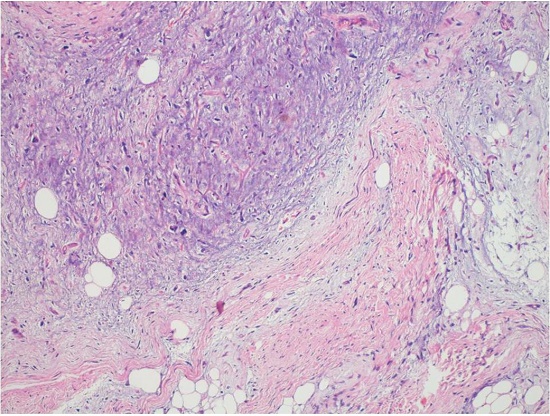
Figure 6
The largest mass showed extensive myxoid stroma (H&E, 200X).
The septal cells were moderate to highly pleomorphic, singly scattered, spindle-shaped with hyperchromatic nuclei, and inconspicuous to occasional prominent nucleoli and wispy eosinophilic cytoplasm (Figure 7A). Many of these cells displayed bizarre morphology, and giant cells and floret-like cells were also noted (Figure 7B). The larger nodules also showed atypical adipocytes with hyperchromatic nuclei and many scattered univacuolated and multivacuolated lipoblasts (Figure 7C). Mitotic figures were occasional (2-4/10 high-power field); necrosis was absent. Immunohistochemistry for MDM2 (Figure 7D) and S100 showed nuclear positivity in the atypical septal cells, lipoblasts, and many of the mature-looking adipocytes.
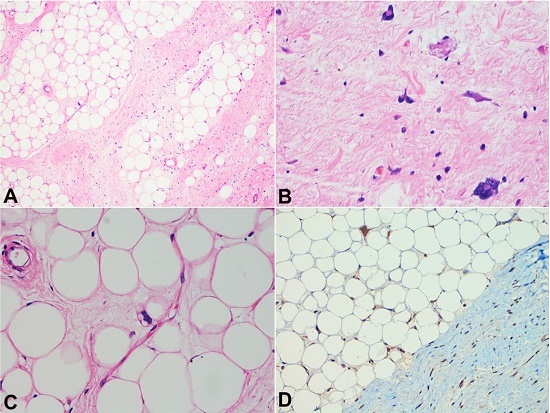
Figure 7
Photomicrographs of the nodular mass. A and B - Thick septa separating the lobules of adipocytes. Note the septa with spindle-shaped singly scattered atypical stromal cells with hyperchromatic nuclei (H&E, 40X and 400X, respectively). C - Multivacuolated lipoblast (H&E, 400X). D - MDM2 immunohistochemistry showing strong nuclear positivity in the stromal cells as well as in the adipocytes (100X).
CD34, Desmin, SMA, and βcatenin were negative in the tumor cells. The cecal bulge showed an endoluminal liposarcoma arising within the submucosa and stretching the overlying mucosa. The remaining ileum, ileocecal valve, and the colon did not reveal any mucosal pathology. The diagnosis of well-differentiated liposarcoma, adipocytic and sclerosing subtypes was rendered with the suspicion that the exophytic masses appeared to arise from the appendices epiploicae, which was consistent with the diagnosis of liposarcomatosis. The spectrum of changes was mostly corroborated by the size of the mass with the larger mass showing thicker septa, fewer number of adipocytes, and an abundance of atypical septal cells, atypical-looking adipocytes, and lipoblasts. Only few of the smaller nodules showed a morphological pattern similar to large nodules in terms of septal thickness and complexity.
DISCUSSION
Liposarcoma is a malignancy of fat cells. It commonly occurs in trunk, limbs, and RP. In fact, the most common variant of soft tissue sarcoma (STS) in the RP is the liposarcoma and accounts for 20% of all STS, and over 50% of RP sarcomas.5 In contrast, primary colonic liposarcoma is a rare entity with only 17 cases reported in the English literature. Liposarcomatosis denotes the simultaneous presence of multiple liposarcomas, and there is only one case of primary colonic liposarcomatosis in the English literature.4 In contrast, multiple peritoneal implants following the removal of the primary tumor have been described by Turkoglu et al.6
The symptomatology of primary colonic liposarcomas depends on the location of the mass. Most of the previously described colonic liposarcomas were solitary. The endoluminal masses may present with features of obstruction (constipation), intussusception, or hematochezia.4,7,8 In contrast, abdominal pain and/or a lump in the abdomen are the usual presentations for exophytic masses similar to the index case.1,6 Dumbbell-shaped masses can also occur.8 The abdomen and the RP are deep, expandable spaces; therefore, slow-growing tumors usually reveal signs and symptoms after a large extent of growth. The majority of these tumors present late after attaining a huge size and causing an increase in the abdominal girth, a palpable lump, or symptoms due to visceral compression. Anemia, diarrhea, and weight loss are the other clinical symptoms, and the former may be associated with sudden rupture and hemorrhage within the lesion, or mucosal ulceration.2,9 The only other previous case4 with liposarcomatosis presented with pain, constipation, and weight loss, and this case had a dominant endoluminal mass; this is in contrast to our case, which presented with pain and swelling due to dominant exophytic masses. Most of the patients were middle-aged or older similar to the index case. However, Rudnicki et al.10 and Fernandes et al.7 have described two cases occurring in young individuals. Importantly, both these cases showed evidence of a predisposing/co-morbid condition in the form of metabolic syndrome and Crohn disease under medication (azathioprine).7,10 However, the case of Crohn disease did not show any disease activity at the time of surgery.7 Most of the colonic liposarcomas were reported to occur in the cecum or ascending colon similar to the index case, although both the descending colon and sigmoid also can be affected (see Table 1).
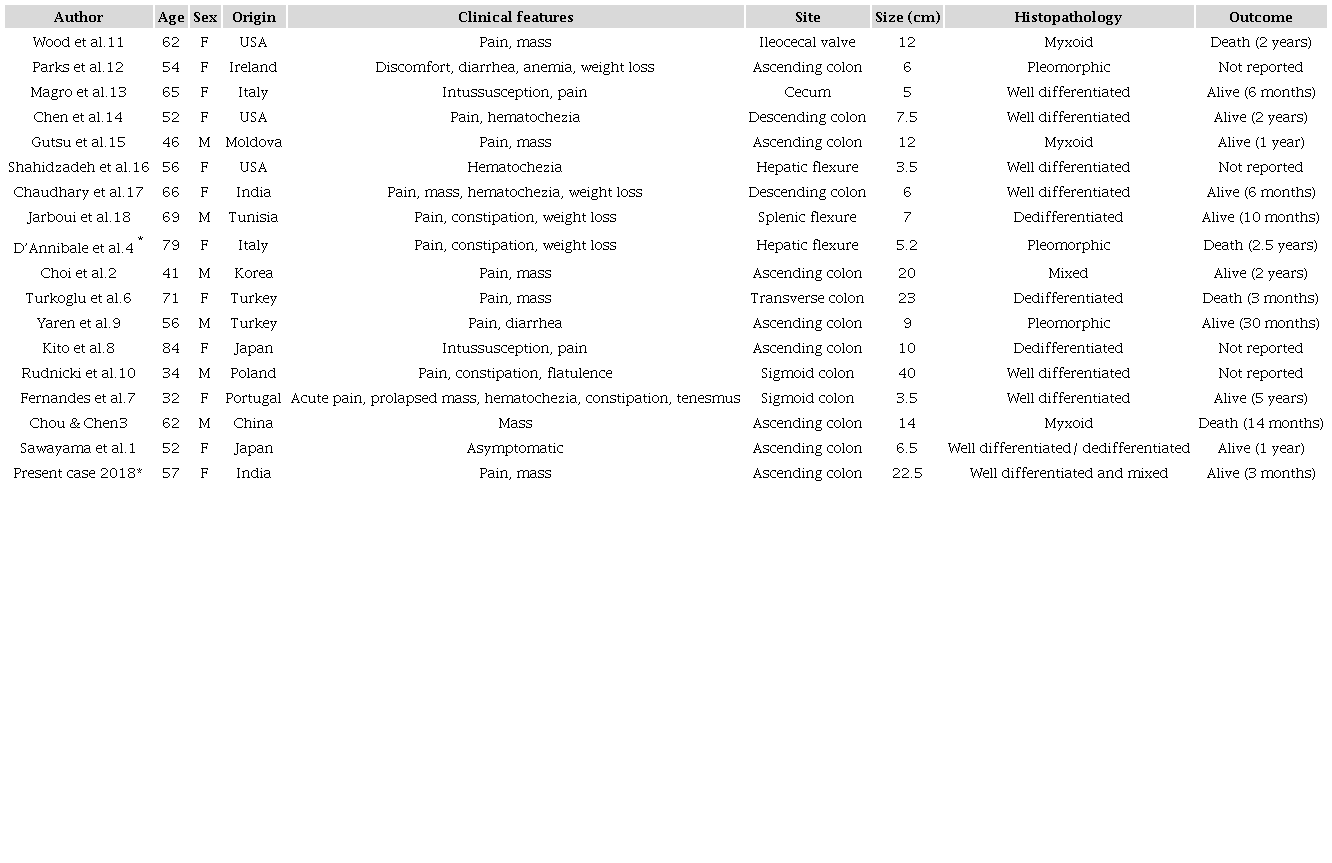
* Cases with liposarcomatosis.
Histologically, liposarcoma can be subdivided into well-differentiated, dedifferentiated, myxoid/round cell, and pleomorphic subtypes. The well-differentiated liposarcoma/atypical lipomatous tumor can be further subdivided into adipocytic, sclerosing/spindle cell, and inflammatory subtypes. Choi et al.2 had described a rare case of primary colonic liposarcoma with mixed histomorphology with a combination of well-differentiated and myxoid features.2 The previous case of liposarcomatosis was histologically categorized as pleomorphic liposarcoma.4 The index case was unique to show the presence of well-differentiated morphology in a case of liposarcomatosis.
Our case showed numerous pedunculated exophytic masses attached to the colon, simulating variable-sized appendices epiploicae. Indeed, all such masses showed liposarcomatous changes on histopathology. The larger masses showed planes of cleavage between them with nodular cut surfaces, which prompted us to think that these masses could have arisen from the coalescence of the appendices. Moreover, our case showed the histomorphological spectrum of changes in these masses with the larger mass showing the increased thickness of the septa, fewer numerous adipocytes, and an abundance of atypical cells in the septa and the lipoblasts. We could not find any mention of such a phenomenon in the literature. This is possibly because we demonstrate only the second case of primary colonic liposarcomatosis. Our case represents multiple exophytic and single endophytic liposarcomas of the colon, and we are tempted to think that the exophytic masses had possibly arisen from the appendices epiploicae, based on their gross and histomorphological features.
The natural behavior and outcome of STS are dependent on the age of the patient, anatomical site and depth, size, and resectability of the tumor, as well as histology, grade, nodal disease, and distant metastasis.19 Management of these tumors mandates a multidisciplinary approach ideally carried out at referral centers treating a high number of patients. The diagnostic investigation of choice is CECT scanning or magnetic resonance imaging (MRI) of the abdomen and pelvis.20,21 Imaging helps to identify the anatomical location of the tumor; its size and origin; the relationship to adjacent visceral and neurovascular structures; possible compression or invasion; and the presence of liver or lung metastases.21,22 Liposarcomas have a characteristic appearance on CT and MRI with a predominantly fatty component.
Surgery is the mainstay of the treatment for primary colonic liposarcoma. Usually, an en bloc resection of the tumor is carried out with macroscopically negative margins. In most patients, location, density, and displacement, rather than the invasion of the adjacent organs, is diagnostic of the tumor and precludes the pre-treatment biopsy. However, in some patients, radiology may point towards different entities, such as lymphoma, neuroendocrine tumor, or gastrointestinal stromal tumor, which may necessitate a pre-treatment biopsy. In contrast to limb sarcomas, removal of the entire tumor in colonic liposarcoma/liposarcomatosis may not be achieved. As a consequence, disease recurrence and death may ensue. Adjuvant radiation therapy may constitute a valuable treatment option in order to improve local control, specifically with the involved margins or high-grade tumors. Chemosensitivity is determined by histological type and grade. Jones et al.23 investigated the response to chemotherapy in 88 patients with liposarcoma (43% located in the RP). They found a significantly higher response rate in myxoid liposarcoma compared to all other liposarcomas (48% vs. 18%, p = 0.012). The response rate was 25% in dedifferentiated liposarcomas, while none of the well-differentiated liposarcomas responded. Targeting MDM2 or CDK4 in well-differentiated liposarcoma and dedifferentiated liposarcoma has been of interest for several years.15 This may be a very promising approach, especially for advanced or unresectable well-differentiated and dedifferentiated liposarcomas.
CONCLUSION
We describe a case of primary colonic liposarcomatosis. This appears to be the second such case in English literature. We also believe that this case is unique as most of the exophytic masses in the index case possibly arose from the appendices epiploicae. The extreme rarity of primary colonic liposarcoma/liposarcomatosis precludes the establishment of a standard management protocol in such cases. Further longitudinal studies are required in this regard.
ACKNOWLEDGEMENTS
We acknowledge both Dr. Kartik and Dr. Rasheeda, junior residents in the Department of Pathology for their help during the grossing of the specimen.
REFERENCES
Sawayama H, Yoshida N, Miyamoto Y, et al. Primary colonic well-differentiated/dedifferentiated liposarcoma of the ascending colon: a case report. Surg Case Rep. 2017;3(1):96. http://dx.doi.org/10.1186/s40792-017-0373-4. PMid:28856628
Choi YY, Kim YJ, Jin SY. Primary liposarcoma of the ascending colon: a rare case of mixed type presenting as hemoperitoneum combined with other type of retroperitoneal liposarcoma. BMC Cancer. 2010;10(1):239. http://dx.doi.org/10.1186/1471-2407-10-239. PMid:20507577
Chou CK, Chen ST. Computed tomography identification of an exophytic colonic liposarcoma. Radiol Case Rep. 2016;11(3):161-4. http://dx.doi.org/10.1016/j.radcr.2016.06.005. PMid:27594941
D’Annibale M, Cosimelli M, Covello R, Stasi E. Liposarcoma of the colon presenting as an endoluminal mass. World J Surg Oncol. 2009;7(1):78. http://dx.doi.org/10.1186/1477-7819-7-78. PMid:19852822
Dalal KM, Kattan MW, Antonescu CR, Brennan MF, Singer S. Subtype specific prognostic nomogram for patients with primary liposarcoma of the retroperitoneum, extremity, or trunk. Ann Surg. 2006;244(3):381-91. PMid:16926564
Türkoğlu MA, Elpek GO, Dogru V, Calış H, Uçar A, Arıcı C. An unusual case of primary colonic dedifferentiated liposarcoma. Int J Surg Case Rep. 2014;5(1):8-11. http://dx.doi.org/10.1016/j.ijscr.2013.10.013. PMid:24394854
Fernandes SR, Rita Goncalves A, Lopes J, et al. Primary liposarcoma of the sigmoid presenting as colonic intussusception - A case report. Rev Esp Enferm Dig. 2016;108(9):591-4. PMid:26785977
Kito Y, Fujii T, Nishiyama T, et al. Peduncular liposarcoma of the colon: a case report and literature review. J Gastrointest Cancer. 2014;45(Suppl. 1):248-51. http://dx.doi.org/10.1007/s12029-014-9647-2. PMid:25216753
Yaren A, Degirmencioglu S, Calli Demirkan N, Gokcen Demiray A, Taskoylu B, Gokoz Dogu G. Primary mesenchymal tumors of the colon: a report of three cases. Turk J Gastroenterol. 2014;25(3):314-8. http://dx.doi.org/10.5152/tjg.2014.4010. PMid:25141322
Rudnicki C, Romanowski M, Medrek-Socha M, Stec-Michalska K. The diagnosis of sigmoid liposarcoma in a young male with metabolic syndrome. J Clin Diagn Res. 2015;9(12):OD01-03. PMid:26816934
Wood DL, Morgenstern L. Liposarcoma of the ileocecal valve: a case report. Mt Sinai J Med. 1989;56(1):62-4. PMid:2784186
Parks RW, Mullan FJ, Kamel HM, Walsh MY, McKelvey ST. Liposarcoma of the colon. Ulster Med J. 1994;63(1):111-3. PMid:8658985
Magro G, Gurrera A, Di Cataldo A, Licata A, Vasquez E. Well-differentiated lipoma-like liposarcoma of the caecum. Histopathology. 2000;36(4):378-80. http://dx.doi.org/10.1046/j.1365-2559.2000.0855d.x. PMid:10841651
Chen KT. Liposarcoma of the colon: a case report. Int J Surg Pathol. 2004;12(3):281-5. http://dx.doi.org/10.1177/106689690401200312. PMid:15306943
Gutsu E, Ghidirim G, Gagauz I, Mishin I, Iakovleva I. Liposarcoma of the colon: a case report and review of literature. J Gastrointest Surg. 2006;10(5):652-6. http://dx.doi.org/10.1016/j.gassur.2005.09.014. PMid:16773759
Shahidzadeh R, Ponce CR, Lee JR, Chamberlain SM. Liposarcoma in a colonic polyp: case report and review of the literature. Dig Dis Sci. 2007;52(12):3377-80. http://dx.doi.org/10.1007/s10620-007-9806-4. PMid:17393311
Chaudhary A, Arora R, Sharma A, Aggarwal S, Safaya R, Sharma S. Primary colonic liposarcoma causing colo-colic intusussception: a case report and review of literature. J Gastrointest Cancer. 2007;38(2-4):160-3. http://dx.doi.org/10.1007/s12029-008-9031-1. PMid:18972225
Jarboui S, Moussi A, Jarraya H, et al. Primary dedifferentiated liposarcoma of the colon: a case report. Gastroenterol Clin Biol. 2009;33(10-11):1016-8. http://dx.doi.org/10.1016/j.gcb.2008.11.014. PMid:19272723
Lewis JJ, Leung D, Woodruff JM, Brennan MF. Retroperitoneal soft-tissue sarcoma: analysis of 500 patients treated and followed at a single institution. Ann Surg. 1998;228(3):355-65. http://dx.doi.org/10.1097/00000658-199809000-00008. PMid:9742918
Thomas JM. Retroperitoneal sarcoma. Br J Surg. 2007;94(9):1057-8. http://dx.doi.org/10.1002/bjs.5967. PMid:17701955
Hughes TM, Spillane AJ. Imaging of soft tissue tumours. Br J Surg. 2000;87(3):259-60. http://dx.doi.org/10.1046/j.1365-2168.2000.01412.x. PMid:10718790
Hoffman A, Lazar AJ, Pollock RE, Lev D. New frontiers in the treatment of liposarcoma, a therapeutically resistant malignant cohort. Drug Resist Updat. 2011;14(1):52-66. http://dx.doi.org/10.1016/j.drup.2010.11.001. PMid:21169051
Jones RL, Fisher C, Al-Muderis O, Judson IR. Differential sensitivity of liposarcoma subtypes to chemotherapy. Eur J Cancer. 2005;41(18):2853-60. http://dx.doi.org/10.1016/j.ejca.2005.07.023. PMid:16289617
Notes
Author notes
Correspondence Dr. Suvradeep Mitra Department of Pathology and Lab Medicine Academic Block, 2nd Floor - AIIMS - Bhubaneswar/Orissa - Índia PIN: 751019 Phone: +919855663999 / Fax: +916742472215 sugreebm@gmail.com
Conflict of interest declaration