Article / Clinical Case Report
Tracheal stenosis due to endotracheal tube cuff hyperinflation: a preventable complication
 Márcio Teodoro da Costa Gaspar
Márcio Teodoro da Costa Gaspar
Tracheal stenosis due to endotracheal tube cuff hyperinflation: a preventable complication
Autopsy and Case Reports, vol. 9, no. 1, e2018072, 2019
Hospital Universitário da Universidade de São Paulo
Received: 06 April 2018
Accepted: 08 October 2018
ABSTRACT: Endotracheal intubation injuries are rare, but may be devastating—mostly among the pediatric patients or when these occur in the distal trachea. Such complications typify a therapeutic challenge, which, besides requiring intellectual and technical resources, takes a long time to reach a resolution. The authors present the case of a 15-year-old girl admitted with an abnormal state of consciousness due to diabetic ketoacidosis. She was submitted to endotracheal intubation with hyperinflation of the tube cuff, which rendered tracheal necrosis and detachment of the tracheal mucosa, and consequent obstruction. Later, she developed scarring retraction and stenosis. The patient was successfully treated with an endotracheal prosthesis insertion. The aim of this report is to illustrate a preventable complication.
Keywords: Tracheal Stenosis, Intubation, Endotracheal, Prosthesis Implantation.
INTRODUCTION
Tracheal stenoses due to endotracheal intubation are rare and usually present a benign course. However, their treatment is complex and requires specialized evaluation. Endotracheal intubation is a procedure frequently necessary among severely ill patients, and may be performed by less-experienced physicians. In this setting, particularities of the procedure should be observed to avoid injuries while attempting to maintain the capillary pressure of the tracheal mucosa at around 20-40 mmHg. Exceeding tracheal cuff pressures will result in ischemic necrosis, which leads to confluent mucosal ulceration, deep stromal necrosis, and perichondritis within 96 hours, and the chondritis will subsequently favor cartilage necrosis. The healing process of the extensive ulcers will cause stenosis due to fibrous tissue.1,2
The mechanisms of the airway injury associated with endotracheal intubation are (i) high pressure of the intubation tube cuff; (ii) tube support in the posterior commissure of the larynx; (iii) repetitive movement of the endotracheal tube causing mucosal injury; and (iv) repeated tracheal intubation. The tracheal tube (nasally or orally inserted) will always push the posterior larynx, which is where major mucosal injuries occur.3
CASE REPORT
A 15-year-old girl was brought to the emergence care unit (ECU) because of acidosis and a decreased level of consciousness. She was diagnosed with type 1 diabetes with poor treatment adherence. She was referred to the intensive care unit (ICU) and was submitted to endotracheal intubation for 5 days. After 3 days of extubation, the patient showed respiratory distress due to stenosis of the trachea at the fourth tracheal ring, which was diagnosed by a nasofibroscopy. The cervical computed tomography (CT) study showed a segmental parietal concentric thickening of the trachea with 2 cm of craniocaudal extension associated with a marked luminal reduction at the T1 level directly below the thyroid gland (Figure 1A and 1B).
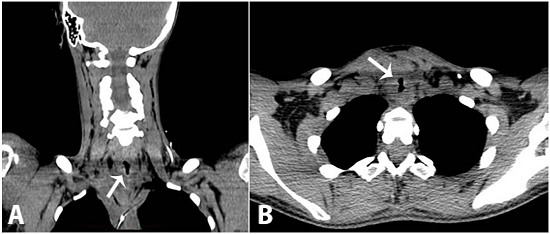
Figure 1
A - Cervical computed tomography (CT) - coronal plane; B - Thoracic CT - axial plane showing concentric stenosis of the trachea (arrows).
The suspension videolaringoscopy evidenced ulcers in the lateral and posterior walls of the trachea, and necrosis of the mucosa at the fifth tracheal ring (Figure 2A). A complete resection of the necrotic tissue that measured 2 cm was undertaken. At the end of the procedure, the trachea resumed an almost normal caliber (Figure 2B). The histopathological examination of the surgical specimen was represented by tracheal necrosis (Figure 3).
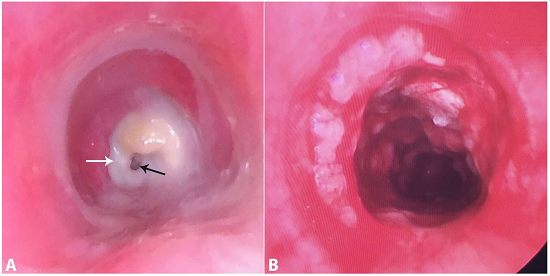
Figure 2
Endoscopic view. A - Tracheal stenosis (white arrow) at the fourth tracheal ring and a narrow remaining lumen (black arrow); B - Post-resection of the necrotic tissue. Note the enlargement of the tracheal lumen.
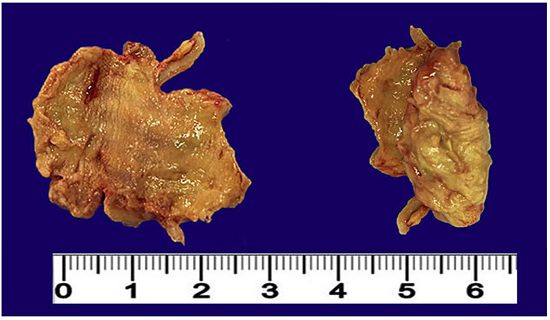
Figure 3
Gross appearance of the surgical specimen represented by tracheal necrosis.
The patient was discharged 3 days after the endoscopic necrosis resection. However, she returned to the ECU after 9 days, presenting severe respiratory distress due to upper airway obstruction, which required urgent fiberoptic bronchoscope-guided orotracheal intubation. A new rigid and eccentric stenosis was diagnosed (Figure 4A). In attempting the tracheal dilation with the bronchoscope, and with the intubation tube insertion, a rupture and laceration of the posterior pars membranacea of the trachea in its proximal stenotic portion occurred, with consequent pneumomediastinum, which was drained with a pigtail coupled to a Heimlich valve. The patient remained intubated for 24 hours and another suspended videolaringoscopy found a false path in the posterior tracheal wall measuring 4 cm, which extended 5 cm from the cricoid cartilage and 4 cm from the carina (Figure 4B). The lesion was better observed during positive pressure ventilation.
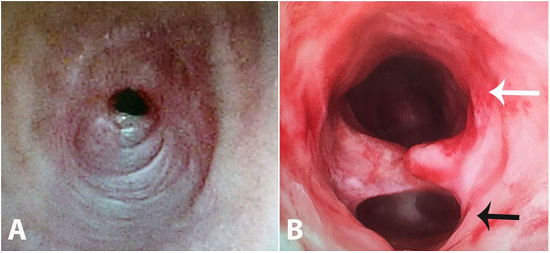
Figure 4
Endoscopic view. A - Scarring fibrotic stenosis 9 days after the exeresis of the necrotic tissue; B - Iatrogenic injury of the trachea with a false path (black arrow).
An endoprosthesis (silicone Stening®) (Figure 5) was inserted along the whole extension of the tracheal injury fixed with polypropylene 3-0.
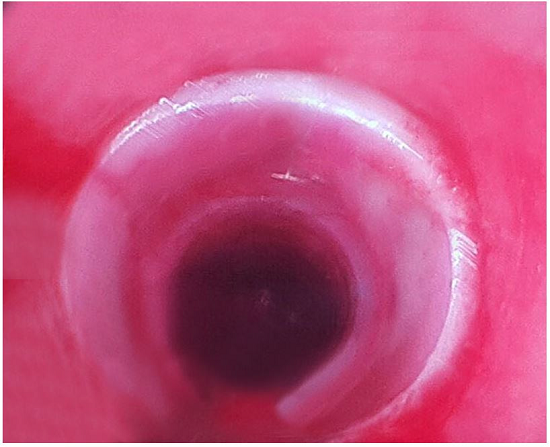
Figure 5
Endoscopic view of the silicon endoprosthesis placed along the entire tracheal lesion.
Additionally, an upper digestive endoscopy was performed, which showed a Los Angeles-A esophagitis and biliary reflux. A control thoracic CT showed pneumomediastinum, a pneumothorax, extensive cervical subcutaneous emphysema, and a prosthesis surrounded by gas in the thoracocervical transition (Figure 6).
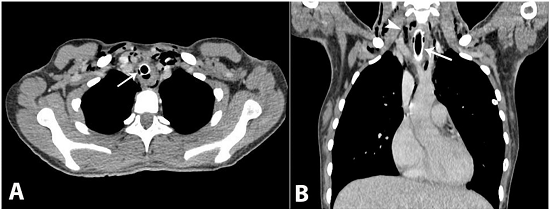
Figure 6
Thoracic computed tomography. A - Axial plane showing the endoprosthesis inserted in the trachea, and a posterior airspace corresponding to the traumatic false path (white arrow); B - Coronal plane showing the endoprosthesis placed in the middle third of the trachea (white arrow) surrounded by pneumomediastinum (arrowhead).
A Nissen-type anti-reflux valve was performed by laparoscopy 40 days after the last endoscopic procedure, due to the marked biliary reflux. The patient was discharged and has been kept on an outpatient clinic follow-up over the last year, with good control of the diabetes and with normal respiratory function. Surgery has been scheduled for the final tracheal injury correction.
DISCUSSION
The case presented herein illustrates a preventable complication of endotracheal intubation followed by a complex and troublesome treatment undertaken in a secondary hospital. This sort of complication is the result of the invasive airway maneuvers developed in the 20th century and the survival of patients treated in ICUs.3
Several tutorials and programs have been developed to guide a safe endotracheal intubation for health professionals.4,5 However, despite all the care, we still face such complications, mainly in pediatrics,6,7 A recent study8 evaluated the endotracheal intubation skill of 85 physicians from three different services: ICU, ECU, and pulmonology. This study concluded that the skill level was unsatisfactory, and that improvement in training was necessary to prevent complications.
The diagnosis of laryngotracheal stenosis is suspected in the presence of (i) barking cough; (ii) hoarseness; (iii) inspiratory stridor; (iv) varying grades of respiratory dysfunction; (v) tachypnea; (vi) intercostal and suprasternal indrawing; (vii) shortness of breath; and (viii) agitation and imminent death sensation. Diagnosis is confirmed by imaging (CT, magnetic resonance imaging) and endoscopic examination. Although these methods are complementary, the latter could be performed when imaging methods are unavailable.9 Endoscopy should be avoided because the procedure, by itself, may worsen the original injury. Therefore, endoscopy should be reserved for therapeutic purposes.
The treatment of choice for laryngotracheal stenosis is surgical; the reconstruction of the airway should be undertaken in centers with extensive experience. Nevertheless, it is associated with high rates of relapse.10 Alternative endoscopic treatments are being developed to treat surgical complications, to replace large operations, and to treat patients with high morbidity.11
Concerning endoscopic treatment, the use of tracheal prosthesis has been more used in specialized centers. Other options, such as endoscopic dilation, argon plasma coagulation, and laser therapy, are also available in some advanced centers. Since the number of patients with such endotracheal complications is increasing, other non-surgical therapeutic options are being developed. In this setting, spray cryotherapy has been used in a series of 26 patients with tracheal stenosis of diverse etiology with partial relief of symptoms, and without any substantial intraoperative or postoperative complications. It seems a safe adjunct therapy.12
We performed the treatment with suspension laryngoscopy; this was represented by the exeresis of the necrotic tissue followed by the insertion of the silicon prosthesis. Stents have been used since 1960s, and silicone ones have good efficacy and tolerance, with low costs and infrequent complications.13 Recent studies have confirmed its effectiveness.14
Technological development in the field of radiology enables new therapeutic aids for the treatment of tracheal stenosis. For example, Kuo et al.15 used CT images before 3D reconstruction to calculate the cross-sectional area and volume of the trachea to assist the physicians with the diagnosis and scheduling the treatment.
In another approach, a group of Russian researchers suggest the use of biotechnology for the treatment and prevention of the stenoses with tissue auto transplant and tissue engineering (tissue culture), with promising short-term results.16,17
Our center has been following patients with tracheal stenosis for more than 20 years. During this period, our patients have been submitted to a suspension laryngoscopy to evaluate (i) the level and the grade of the stenosis; (ii) the need to insert a template to maintain steadiness during endoscopic dilation; and (iii) the need to perform a laryngofissure (cartilage graft with laryngeal molding). The patient with laryngeal stenosis often requires several interventions.
We have also observed a frequent presence of biliary or acid reflux during the operative procedure. Even in the absence of dyspeptic symptoms, or the presence of an eventual interpretation of physiologic reflux,18 we consider the possibility of reflux, which perpetuates the inflammatory process in the laryngotracheal region and postpones the possibility of tracheal decannulation.
Therefore, many of our patients are submitted to impedanciometry and/or pH monitoring before a laryngoscopy is performed. If there is evidence of gastroesophageal reflux, it is treated surgically earlier. The incidence of recurrence of stenosis has been lower in the last 10 years, with successful decannulations.
Much is said about the techniques to treat benign tracheal injuries. However, it seems that relieving this problem is much more difficult than preventing it. Therefore, we suggest that the entire health provider team involved with critical or potentially critical patients, maintains constant updating on airway management.
REFERENCES
Chagas AA Fo, Machado FS, Janiszewski M. Long-term post intubation tracheal stenosis. RBTI. 2005;17(1):40-3.
Sehgal IS, Dhooria S, Bal A, Aggarwal AN, Behera D, Agarwal R. Obstructive fibrinous tracheal pseudomembrane after endotracheal intubation. Respir Care. 2016;61(9):1260-6. http://dx.doi.org/10.4187/respcare.04662. PMid:27247431.
Minamoto H, Terra RM, Cardoso PFG. Estenoses benignas da via aérea: tratamento endoscópico. Pulmão RJ. 2011;20(2):48-53.
Tucori LP. Traumas externos da laringe. In: Anais do 3º Congresso de Otorrinolaringologia da Universidade de São Paulo; 2002; São Paulo, Brazil. São Paulo: Fundação Otorrinolaringologia; 2002.
Tallo FS, Guimarães HP, Lopes RD, et al. Orotracheal intubation and rapid sequence technique: a review for the internist. Rev Bras Clin Med. 2011;9(3):211-7.
Sittel C. Pathologies of the larynx and trachea in childhood. GMS Curr Top Otorhinolaryngol Head Neck Surg. 2014;13:1-15. PMid:25587369.
Jefferson ND, Cohen AP, Rutter MJ. Subglottic stenosis. Semin Pediatr Surg. 2016;25(3):138-43. http://dx.doi.org/10.1053/j.sempedsurg.2016.02.006. PMid:27301599.
Yamanaka CS, Góis AFT, Vieira PCB, et al. Orotracheal intubation: physicians knowledge assessment and clinical practices in intensive care units. Rev Bras Ter Intensiva. 2010;22(2):103-11. http://dx.doi.org/10.1590/S0103-507X2010000200002. PMid:25303750.
Parshin VD, Koroleva IM, Mishchenko MA. Evolution of diagnostic methods for cicatrical tracheal stenosis and tracheomalacia. Khirurgiia (Mosk). 2016;(5):17-25. http://dx.doi.org/10.17116/hirurgia2016517-25. PMid:27271715.
Karapantzos I, Karapantzou C, Zarogoulidis P, Tsakiridis K, Charalampidis C. Benign tracheal stenosis a case report and up to date management. Ann Transl Med. 2016;4(22):451. http://dx.doi.org/10.21037/atm.2016.11.18. PMid:27999785.
Amantéa SL, Silva APP. Clinical management of upper airway obstruction: epiglottitis and laryngotracheobronchitis. J Pediatr (Rio J). 1999;75(Suppl. 2):S177-84. http://dx.doi.org/10.2223/JPED.387. PMid:14685464.
Bhora FY, Ayub A, Forleiter CM, et al. Treatment of benign tracheal stenosis using endoluminal spray cryotherapy. JAMA Otolaryngol Head Neck Surg. 2016;142(11):1082-7. http://dx.doi.org/10.1001/jamaoto.2016.2018. PMid:27532803.
Ayub A, Al-Ayoubi AM, Bhora FY. Stents for airway strictures: selection and results. J Thorac Dis. 2017;9(Suppl 2):S116-21. http://dx.doi.org/10.21037/jtd.2017.01.56. PMid:28446974.
Terra RM, Bibas BJ, Minamoto H, et al. Decannulation in tracheal stenosis deemed inoperable is possible after long-term airway stenting. Ann Thorac Surg. 2013;95(2):440-4. http://dx.doi.org/10.1016/j.athoracsur.2012.09.037. PMid:23201102.
Kuo CF, Leu YS, Kuo R, et al. Three-dimensional reconstruction of trachea using computed tomography imaging as therapy for tracheal stenosis in infants. Comput Methods Programs Biomed. 2016;132:177-87. http://dx.doi.org/10.1016/j.cmpb.2016.04.027. PMid:27282237.
Kurgansky IS, Makhutov VN, Lepekhova SA. The methods for the treatment and prevention of cicatrix stenosis of trachea. Vestn Otorinolaringol 2016;81(1):66-71. PMid:27166482.
Jakobsen KK, Grønhøj C, Jensen DH, Fischer-Nielsen A, Hjuler T, von Buchwald C. Mesenchymal stem cell therapy for laryngotracheal stenosis: a systematic review of preclinical studies. PLoS One. 2017;12(9):3-10. http://dx.doi.org/10.1371/journal.pone.0185283. PMid:28934345.
Guedes CC. Manifestações atípicas da doença do refluxo gastroesofágico [Internet]. [cited 2018 Nov 24]. Available from: http://abran.org.br/wp/wp-content/uploads/2015/02/MANIFESTA%C3%87%C3%95ES-AT%C3%8DPICAS-DA-DOEN%C3%87A-DO-REFLUXO-GASTROESOF%C3%81GICO.pdf
Notes
Author notes
Correspondence Márcio Teodoro da Costa Gaspar Clinica Multiperfil Rua Morro Bento, s/n - Samba / Luanda - Angola Phone: +244 923680961 marcio85gaspar@gmail.com
Conflict of interest declaration