Article / Autopsy Case Report
Sudden onset acute liver failure in a patient with clinically occult small cell lung carcinoma: autopsy report and review of the medical literature
 Massimiliano Guerriero
Arnaldo Carbone
Massimiliano Guerriero
Arnaldo Carbone
Sudden onset acute liver failure in a patient with clinically occult small cell lung carcinoma: autopsy report and review of the medical literature
Autopsy and Case Reports, vol. 9, no. 2, e2019089, 2019
Hospital Universitário da Universidade de São Paulo
Received: 05 May 2019
Accepted: 23 May 2019
Abstract: Liver metastases are commonly found in advanced cancer patients; however, acute liver failure secondary to diffuse liver infiltration is rare. Small cell lung carcinoma accounts for 15% of lung carcinomas. We describe the ninth case of small cell lung carcinoma massively metastatic to the liver, reported in the scientific literature, with sudden clinical onset and death after a few days. An autopsy was performed to understand the cause of death.
Keywords: Small Cell Lung Carcinoma, Hepatomegaly, Acute Liver Failure, Liver Metastasis.
INTRODUCTION
Small cell lung carcinoma (SCLC) is an aggressive neuroendocrine neoplasia, which is strongly related to smoking attitude, characterized by rapid growth and very poor overall survival, usually diagnosed as a central tumor.1 It accounts for 13-15% of all lung cancers and represents the sixth most common cause of death for malignant tumours.2
Histological evaluation is mandatory. According to the World Health Organization (WHO), morphology and immunohistochemistry should be performed for the final diagnosis.3
The lack of specific symptoms at early tumor stages and the lack of screening methods continue to be the main obstacles for the early detection of this disease. Most patients are diagnosed with advanced disease—often with a metastatic dissemination (extensive stage [ES]).4 Because of the highly progressed disease states, clinical courses are usually too short to identify the causes, resulting in multi-organ failure.
We describe the unusual case of an occult SCLC with clinical onset for jaundice and fulminant progression up to death within a few days. The particularities of the case are also its incidental diagnosis at autopsy, clinical onset with non-obstructive jaundice liver disease, and the rapid progression towards death.
To date 35 cases (in 25 papers) of SCLCs with diffuse liver metastases and fulminant liver failure have been described in the medical literature, but in 9 cases the clinical onset was sudden and without warning, followed by a quick death.
We will carry out a critical review of all published cases.
CASE REPORT
A 78-year-old male, who was a heavy smoker, presented at the Emergency Department with recently appeared jaundice (sclera and skin) and lower limbs edema. Past medical history included chronic obstructive pulmonary disease and hypertensive heart disease. He had no history of hepatitis, alcohol abuse, or drug allergy. On admission, the physical examination revealed a globose abdomen with marked hepatomegaly, respiratory examination was consistent with chronic bronchitis with mild dyspnea and shortness of breath.
An abdominal and thoracic computed tomography was performed and showed a lesion in the lower lobe of the right lung highly suspicious of malignancy, and marked hepatomegaly not otherwise specified.
Due to severe renal, cardiac, and hepatic conditions, the patient was hospitalized in intensive care. The patient developed hepatic encephalopathy and later went into a coma. He died with acute liver failure (ALF) and multi-organ failure only 7 days after admission.
AUTOPSY PRESENTATION
The Autopsy Revealed Unexpected Findings
The liver (Figure 1) extended from the right to the left hipochondrium.
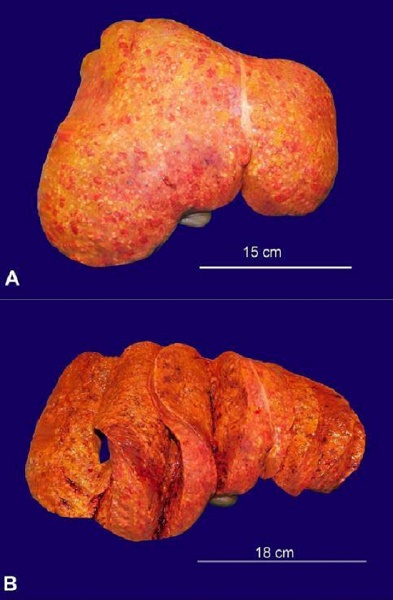
Figure 1
Gross view the liver. A – the outer surface is completely covered by small nodular lesions; B – multiple cross-sections showing the hepatic parenchyma completely occupied by yellowish-white nodules, with an average diameter of 3-4 mm.
The liver’s dimensions had increased so much that it could be measured from the costal arch of 14 cm on the right and 6 cm on the left. The liver weighed 4.25 kg (Reference range [RR]; 1.5 kg) and the cut surface was entirely occupied by small yellowish-white nodules of varying sizes (average size of 0.3-0.4 cm). Moderate ascitic fluid (approx. 400 mL) was present. There was evidence of bilateral pulmonary edema, and lower limbs edema. In the right lower pulmonary lobe (Figure 2) there was a yellowish-white nodule of 5.5 cm, which involved bronchial branches. There were bilateral lymphadenopathies; the ipsilateral major lymph node measured 1.9 cm. The left ventricle hypertrophy (wall thickness of the left ventricle of 2.3 cm) was compatible with hypertensive heart disease. No brain lesions were identified and the other organs did not show remarkable changes.
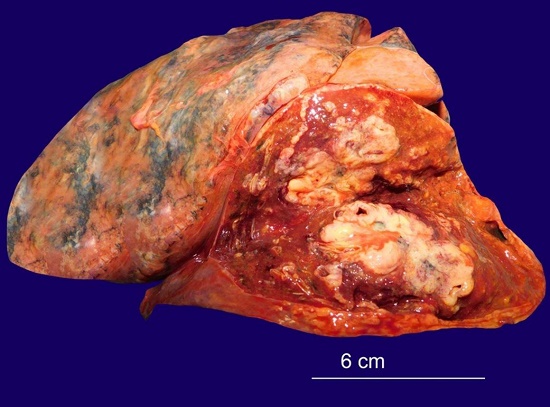
Figure 2
Gross view of lung tumor. A whitish 5.5 cm nodule was found in the right lower lobe, with peribronchial growth.
The Tissues Were Fixed in 10% Neutral Formalin and Embedded in Paraffin
The pulmonary lesion (Figure 3) was an undifferentiated lymphocytic-like neoplasm, mainly of small cells, with nuclear characteristics (salt and pepper chromatin), which allowed the diagnosis of small cell carcinoma. The immunohistochemical findings confirmed a small cell carcinoma; in fact, these tumor cells were strongly and diffusely positive for cytokeratin cocktail MNF116, CD56, and TTF-1, and faintly positive for synaptophysin and chromogranin A.
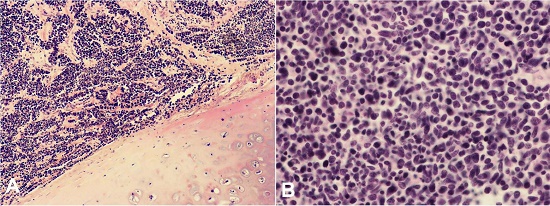
Figure 3
Photomicrographs of the lung neoplasm (A – H&E, 40X; B – H&E, 200X). The lesion histology consisted of small, rounded to oval, tumor cells, diffusely overlapped with diffused growth, with granular chromatin, nucleolus absent.
Three Ipsilateral Peribronchial Lymph Nodes Revealed SLCL Metastases
The liver was enlarged due to massive SLCL infiltration, which was also responsible by the cholestasis (Figures 4 and 5).
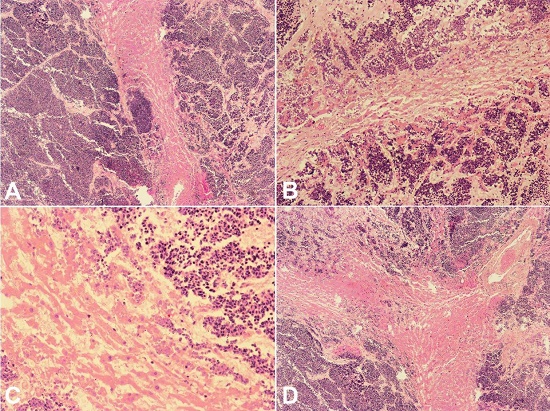
Figure 4
Photomicrographs of liver infiltrated by small cell lungs carcinoma (A – H&E, 40X; B – H&E, 100X; C – H&E, 200X; D – H&E, 40X). The liver was massively infiltrated by the lung neoplasm; only thin cords of hepatocytes remained.
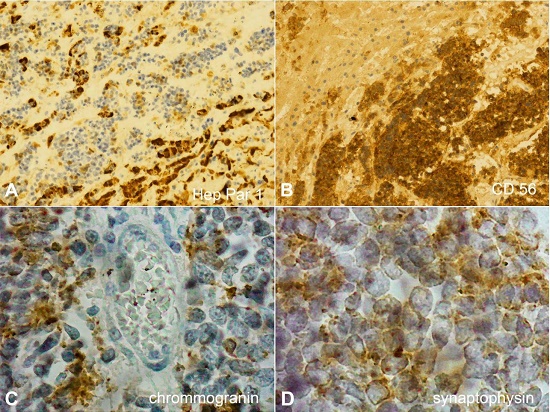
Figure 5
Photomicrographs of liver infiltrated by small cell lung carcinoma. A – the rare waves of residual hepatocytes are evident (Hep Par 1 immunohistochemical stain, 200X); B – the extensive aggregates of neoplastic cells that destroy the hepatic structure are evident (CD56 immunohistochemical stain 200X); C – faint positivitity for Chromogranin (200X); D – faint positivitity for Synaptophysin (400X).
No signs of portal hypertension was found. The spleen was small (weighed 70g, mean RR; 112g), and was histologically normal.
The Remaining Organs Were Free of Neoplastic Infiltration
Based on the gross and microscopic features and the clinical picture, the cause of the patient’s death might therefore be placed as: “ALF and multi-organic damage associated with the hepato-renal syndrome in SCLC with massive hepatic infiltration.”
DISCUSSION
Most studies regarding fulminant hepatic failure in metastatic liver SCLC have been published as case reports. To our knowledge, in 25 scientific papers a total of 35 cases of hepatic failure due to metastatic SCLC were reported (see Table 1).
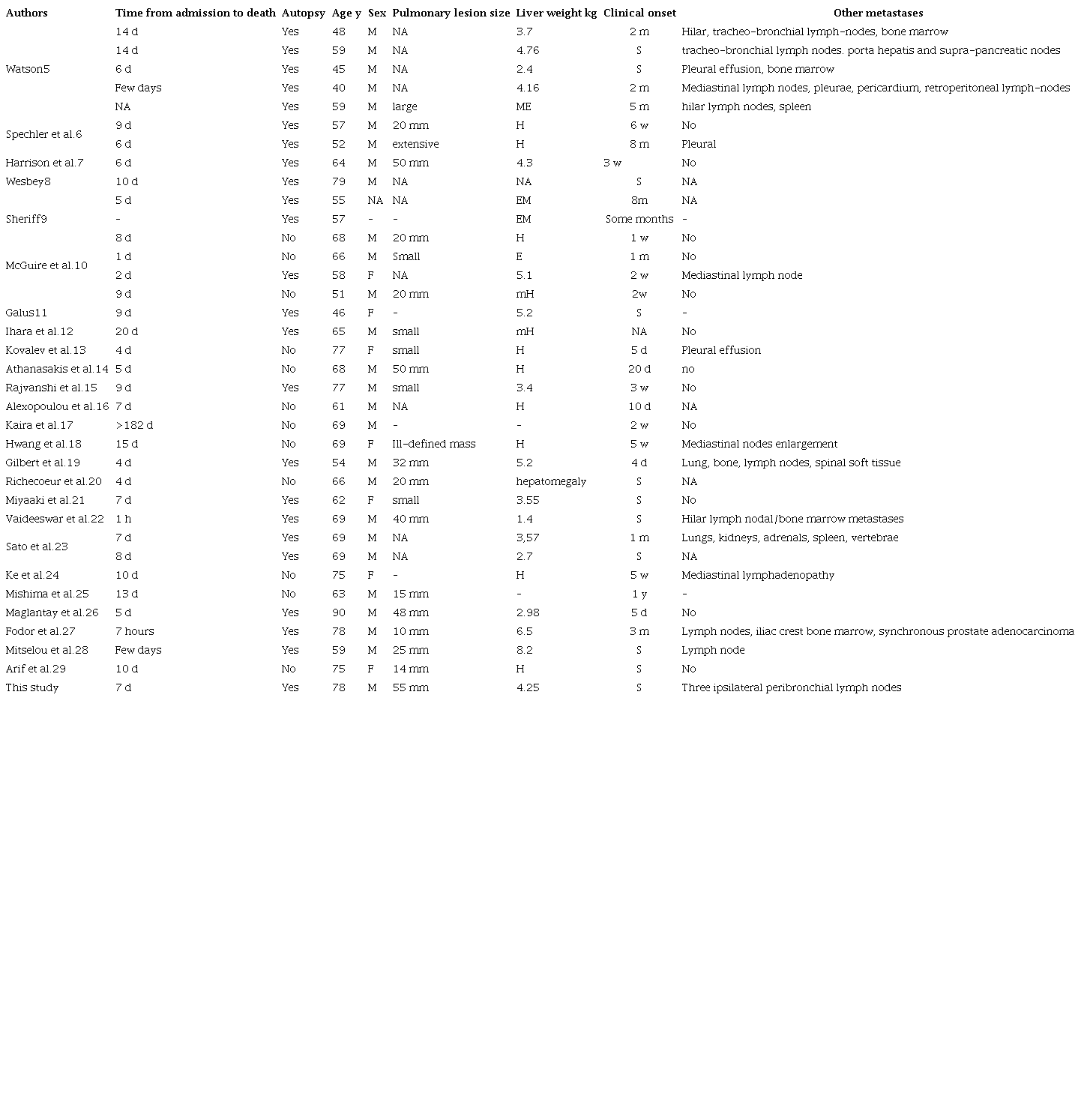
D = days; E = enlarged; EM = extensive metastases; F = female; H = hepatomegaly; M = male; ME = moderately enlarged; NA = not available; S = sudden; SCLC = small cell lung carcinoma; y = year.
An autopsy was performed in 24 of the 35 published cases.5-29
Apart from our case, only 10 others have been described with sudden onset and death within a few days. In 8 of these 10 cases, an autopsy was performed. In this type of case, performing an autopsy is of paramount importance to understand the causes of death. Let us consider these eight cases and compare them with ours.
The lung tumors (when measured) in these cases were large, from a minimum of 14 mm29 to a maximum of 48 mm;26 in our case it measured 55 mm and was the largest ever described, yet it remained clinically silent.
In the other 35 reported cases, the liver weight ranged between 1.4 and 8.2 kg;21,27 in our case, the liver weighed 4.25 kg.
In the other cases, death occurred after a minimum of 1 hour22 from the time of arrival in the hospital to a maximum of 14 days5 (average of 7.1 days); in our case death occurred 7 days after hospitalization.
The liver is the most common site for metastatic tumor deposits with evidence of hepatic metastases reported in 36% of all patients who died from cancer.30 Despite this, liver dysfunction may not be evident. Fulminant hepatic failure (FHF; also known as ALF) secondary to a metastatic tumor is rare. In some cases, tumors may replace up to 90% of the liver without any manifestation of jaundice. However drowsiness and abdominal pain have been reported.
Small cell lung cancer is so highly invasive that hepatic metastasis is common, but a rapid progression to ALF is extremely rare. In most patients with ALF secondary to malignant infiltration of the liver, the prognosis is terrible.
In cases of very rapid progression from the time of clinical onset, the cause of hepatomegaly may be unknown at the time of the patient’s death.
CONCLUSION
Each case of ALF of undetermined etiology must be evaluated with a high index of suspicion. The aggressiveness of SCLC is well documented and, in many cases, metastatic lesions are diagnosed prior to the discovery of the primary tumor. In hepatomegaly, imaging is often non-diagnostic. In order to suggest which therapies to follow, liver biopsy must be considered in indeterminate cases.
Diffuse liver metastasis must be considered when imaging modalities show hepatomegaly in patients with FHF, especially when viral hepatitis and drug reactions are excluded. It is therefore of paramount importance for the clinician to take hepatomegaly into consideration in the investigation of distant metastases of unknown primary origin.
The role of the autopsy in this type of case is fundamental.
REFERENCES
Früh M, De Ruysscher D, Popat S, Crinò L, Peters S, Felip E. Small-cell lung cancer (SCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24(Suppl 6):vi99-105. http://dx.doi.org/10.1093/annonc/mdt178. PMid:23813929
Howlader N, Noone AM, Krapcho M, et al. SEER cancer statistics review, 1975-2010. Bethesda: National Cancer Institute; 2013.
Travis WD, Brambilla E, Nicholson AG, et al. The 2015 World Health Organization classification of lung tumors: impact of genetic, clinical and radiologic advances since the 2004 classification. J Thorac Oncol. 2015;10(9):1243-60. http://dx.doi.org/10.1097/JTO.0000000000000630. PMid:26291008
Dearing MP, Steinberg SM, Phelps R, et al. Outcome of patients with small-cell lung cancer: effect of changes in staging procedures and imaging technology on prognostic factors over 14 years. J Clin Oncol. 1990;8(6):1042-9. http://dx.doi.org/10.1200/JCO.1990.8.6.1042. PMid:2161447
Watson AJ. Diffuse intra-sinusoidal metastatic carcinoma of the liver. J Pathol Bacteriol. 1955;69(1-2):207-17. http://dx.doi.org/10.1002/path.1700690128. PMid:13243188
Spechler SJ, Esposito AL, Koff RS, Hong WK. Lactic acidosis in oat cell carcinoma with extensive hepatic metastases. Arch Intern Med. 1978;138(11):1663-4. http://dx.doi.org/10.1001/archinte.1978.03630360045020. PMid:214048
Harrison HB, Middleton HM 3rd, Crosby JH, Dasher MN Jr. Fulminant hepatic failure: an unusual presentation of metastatic liver disease. Gastroenterology. 1981;80(4):820-5. http://dx.doi.org/10.1016/0016-5085(81)90147-5. PMid:7202952
Wesbey G. Lactic acidosis in oat cell carcinoma with extensive hepatic metastases. Arch Intern Med. 1981;141(6):816-7. http://dx.doi.org/10.1001/archinte.1981.00340060124034. PMid:6263203
Sheriff DS. Lactic acidosis and small cell carcinoma of the lung. Postgrad Med J. 1986;62(726):297-8. http://dx.doi.org/10.1136/pgmj.62.726.297. PMid:3012499
McGuire BM, Cherwitz DL, Rabe KM, Ho SB. Small-cell carcinoma of the lung manifesting as acute hepatic failure. Mayo Clin Proc. 1997;72(2):133-9. http://dx.doi.org/10.4065/72.2.133. PMid:9033546
Galus M. Liver failure due to metastatic small-cell carcinoma of the lung. Mayo Clin Proc. 1997;72(8):791. http://dx.doi.org/10.1016/S0025-6196(11)63603-3. PMid:9276611
Ihara N, Yashiro N, Kinoshita T, et al. Diffuse intrasinusoidal liver metastasis of small cell lung cancer causing fulminant hepatic failure: CT findings-a case report. Radiat Med. 2001;19(5):275-7. PMid:11724260
Kovalev Y, Lurie M, Naschitz JE, Yeshurun D, Zuckerman E. Metastatic small cell carcinoma presenting as acute hepatic failure. Am J Gastroenterol. 2001;96(12):3471-3. http://dx.doi.org/10.1111/j.1572-0241.2001.05366.x. PMid:11774994
Athanasakis E, Mouloudi E, Prinianakis G, Kostaki M, Tzardi M, Georgopoulos D. Metastatic liver disease and fulminant hepatic failure: presentation of a case and review of the literature. Eur J Gastroenterol Hepatol. 2003;15(11):1235-40. http://dx.doi.org/10.1097/00042737-200311000-00014. PMid:14560159
Rajvanshi P, Kowdley KV, Hirota WK, Meyers JB, Keeffe EB. Fulminant hepatic failure secondary to neoplastic infiltration of the liver. J Clin Gastroenterol. 2005;39(4):339-43. http://dx.doi.org/10.1097/01.mcg.0000155123.97418.06. PMid:15758630
Alexopoulou A, Koskinas J, Deutsch M, Delladetsima J, Kountouras D, Dourakis SP. Acute liver failure as the initial manifestation of hepatic infiltration by a solid tumor: report of 5 cases and review of the literature. Tumori. 2006;92(4):354-7. http://dx.doi.org/10.1177/030089160609200417. PMid:17036530
Kaira K, Takise A, Watanabe R, Mori M. Fulminant hepatic failure resulting from small-cell lung cancer and dramatic response of chemotherapy. World J Gastroenterol. 2006;12(15):2466-8. http://dx.doi.org/10.3748/wjg.v12.i15.2466. PMid:16688847
Hwang YT, Shin JW, Lee JH, et al. A case of fulminant hepatic failure secondary to hepatic metastasis of small cell lung carcinoma. Korean J Hepatol. 2007;13(4):565-70. http://dx.doi.org/10.3350/kjhep.2007.13.4.565. PMid:18159155
Gilbert J, Rutledge H, Koch A. Diffuse malignant infiltration of the liver manifesting as a case of acute liver failure. Nat Clin Pract Gastroenterol Hepatol. 2008;5(7):405-8. http://dx.doi.org/10.1038/ncpgasthep1154. PMid:18521114
Richecoeur M, Massoure M-P, Le Coadou G, Lipovac AS, Bronstein J-A, Delluc C. Acute hepatic failure as the presenting manifestation of a metastatic lung carcinoma to liver. Rev Med Interne. 2009;30(10):911-3. http://dx.doi.org/10.1016/j.revmed.2009.01.016. PMid:19328604
Miyaaki H, Ichikawa T, Taura N, et al. Diffuse liver metastasis of small cell lung cancer causing marked hepatomegaly and fulminant hepatic failure. Intern Med. 2010;49(14):1383-6. http://dx.doi.org/10.2169/internalmedicine.49.3296. PMid:20647652
Vaideeswar P, Munot S, Rojekar A, Deodhar K. Hepatic diffuse intra-sinusoidal metastases of pulmonary small-cell carcinoma. J Postgrad Med. 2012;58(3):230-1. http://dx.doi.org/10.4103/0022-3859.101654. PMid:23023366
Sato K, Takeyama Y, Tanaka T, Fukui Y, Gonda H, Suzuki R. Fulminant hepatic failure and hepatomegaly caused by diffuse liver metastases from small cell lung carcinoma: 2 autopsy cases. Respir Investig. 2013;51(2):98-102. http://dx.doi.org/10.1016/j.resinv.2012.12.004. PMid:23790738
Ke E, Gomez JD, Tang K, Sriram KB. Metastatic small-cell lung cancer presenting as fulminant hepatic failure. BMJ Case Rep. 2013;2013(1):bcr2012007865. http://dx.doi.org/10.1136/bcr-2012-007865. PMid:23616311
Mishima S, Nozaki Y, Mikami S, et al. Diffuse liver metastasis of small-cell lung cancer presenting as acute liver failure and diagnosed by transjugular liver biopsy: a rare case in whom nodular lesions were detected by enhanced CT examination. Case Rep Gastroenterol. 2015;9(1):81-7. http://dx.doi.org/10.1159/000381140. PMid:25969674
Maglantay R, Qin J, Lanjewar S, et al. Metastatic small cell carcinoma of the lung: an unusual cause of acute fulminant hepatic failure. Fed Pract. 2016;33(Suppl 5):30S-4S. PMid:30766221
Fodor D, Gurzu S, Contac AO, Jung I. Giant hepatic metastasis in a patient with coin-like small cell lung carcinoma incidentally diagnosed at autopsy: a case report. Medicine. 2017;96(11):e6366. http://dx.doi.org/10.1097/MD.0000000000006366. PMid:28296775
Mitselou A, Papadatos SS, Tsoultsidou S, et al. Giant metastatic liver tumor of unknown primary origin: thoracic autopsy solves the mystery. Acta Med. 2017;60(4):163-6. http://dx.doi.org/10.14712/18059694.2018.14. PMid:29716684
Arif H, Suchniak-Mussari K, Beg M, Morrissey S. Unusual acute liver failure from small cell carcinoma of the lung. Clin Exp Hepatol. 2018;4(4):275-7. http://dx.doi.org/10.5114/ceh.2018.80130. PMid:30603677
Rowbotham D, Wendon J, Williams R. Acute liver failure secondary to hepatic infiltration: a single centre experience of 18 cases. Gut. 1998;42(4):576-80. http://dx.doi.org/10.1136/gut.42.4.576. PMid:9616324
Notes
Author notes
Correspondence Massimiliano Guerriero Department of Pathology - Regional Health Authority of Molise (ASReM) - Antonio Cardelli Regional Hospital Contrada Tappino s.n.c. Campobasso/CB – Italy 86100 Phone: +39 (0874) 409-205 ilguerrierochecorre@gmail.com
Conflict of interest declaration