Article / Autopsy Case Report
Sigmoid gallstone ileus: a challenging diagnosis
 Renuka Malenie
Renuka Malenie
Sigmoid gallstone ileus: a challenging diagnosis
Autopsy and Case Reports, vol. 9, no. 2, e2019102, 2019
Hospital Universitário da Universidade de São Paulo
Received: 01 March 2019
Accepted: 21 March 2019
Abstract: Gallstone ileus is a rare (1%–4%) complication of gallstone disease. Gallstones entering the gastrointestinal tract by penetration may cause obstruction at any point along their course through the tract; however, they have a predilection to obstruct the smaller-caliber lumen of the small intestine (80.1%) or stomach (14.2%). The condition is seen more commonly in the elderly who often have significant co-morbidities. Gallstone ileus causing large bowel obstruction is rare. We report the case of a 95-year-old woman who presented with a history of abdominal pain without fever, nausea, vomiting, or diarrhea. Computed tomography of the abdomen and pelvis with oral contrast revealed a high-density structure within the lumen of the distal sigmoid colon, initially suspected to be a foreign body. Medical management failed and surgical intervention was not possible. Autopsy revealed peritonitis and a rupture of the sigmoid colon at the site of a cylindrical stone found impacted in an area of fibrotic narrowing with multiple diverticula. A necrotic, thick-walled gallbladder had an irregular stone in its lumen that was a fracture match with the stone in the sigmoid. Adhesions, but no discrete fistula, were identified between the gallbladder and the adjacent transverse colon. The immediate cause of death was peritonitis caused by colonic perforation by the gallstone impacted at an area of diverticular narrowing. To our knowledge, such autopsy findings have not been previously reported.
Keywords: Autopsy, Gallstones, Colon, Sigmoid, Diverticulosis, Intestinal Perforation.
CASE REPORT
The patient was a 95-year-old African American female living in a nursing home who complained of abdominal pain for about 6 days. The patient had a past medical history of hypertension, dementia, chronic obstructive pulmonary disease, chronic kidney disease, and gastroesophageal reflux disease. She had worsening pain and requested to be taken to the hospital, which was unusual for her. She was brought to the local emergency department (ED). A computed tomography (CT) scan done in the ED showed a 3.4 × 3.5 cm curvilinear structure with high-density wall within the lumen of the distal sigmoid colon, suspect foreign body. There was moderate bowel wall thickening proximal to this level compatible with colitis. There were scattered colonic diverticula. Pneumobilia without significant bile duct dilatation. The gall bladder was not clearly delineated.” The CT image is shown in Figure 1 with a stone in the sigmoid colon and a stone in the gallbladder with pneumobilia.
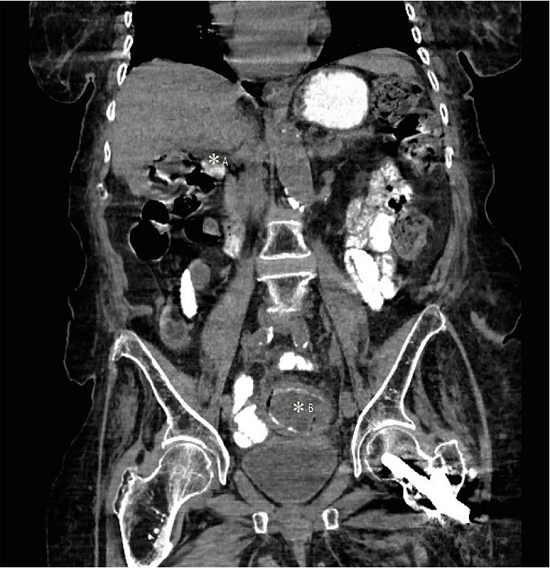
Figure 1
Abdominal computed tomography from the emergency room showing a stone in the gallbladder with pneumobilia – A; and another stone in the sigmoid colon – B.
Aggressive bowel cleansing was initiated in an unsuccessful attempt to pass the foreign body, suspected to be a gallstone. The patient had increased pain after an enema. By the third hospital day, she was hypotensive and septic with increasing abdominal pain. Surgical intervention or colonoscopy was no longer considered possible. The family agreed to comfort care. The patient died on the third hospital day.
AUTOPSY FINDINGS
The patient’s body weighed 68.0 kilograms and measured 157.0 centimeters in length (body mass index 27.68 kg/m2). The autopsy was performed in the conventional manner.
On opening the thoracic cavity, the right and left pleural cavities each contained 50 mL of serous fluid. The pleural surfaces were pale pink at the anterior surface, and red-maroon on the posterior surface with moderate black pigmentation. The lungs were subcrepitant to palpation and soft on section. The cut surfaces were red-maroon and edematous. The distal airways were clear. The pulmonary vessels were unremarkable.
The pericardial cavity contained no significant accumulation of fluid. The heart weighed 370 g (reference range [RR] for height 139–316 g) and was slightly grossly enlarged with mild left ventricular hypertrophy. The coronary arteries had right dominant distribution with 10% atherosclerotic narrowing of the left main artery, the left anterior descending and circumflex arteries, and the right main artery. The fossa ovalis measured 1.8 cm, and the foramen ovale was closed. The myocardium was red-brown with no focal lesions and the free walls measured 0.6 cm and 1.5 cm, right and left, respectively. The interventricular septum measured 1.7 cm. The circumferences of the cardiac valves were: tricuspid 12.4 cm (RR; 12–13 cm), pulmonic 10.1 cm (RR; 8.5–9 cm), mitral 9.8 cm (RR; 10–10.5 cm), and aortic 7.8 cm (RR; 8–8.5 cm) cm. The intimal surface of the aorta was not roughened by atherosclerotic plaque. The remainder of the vascular system was unremarkable.
The peritoneal cavity contained 200–250 mL of brown-gray opaque fluid with yellow fibrin strands. Bowel contents (resembling corn and celery) were identified in the fluid. Dense adhesions were found between the perforated gallbladder and the transverse colon, but no discrete perforation or fistula of the transverse colon was identified. The esophagus had no significant abnormalities. The stomach contained 150 mL of green-yellow liquid. The gastric mucosa and the small bowel mucosa were unremarkable. The sigmoid colon revealed an acute perforation measuring 4.0 × 2.4 cm and a cylindrical stone measuring 4.5 × 2.9 × 2.9 cm in the bowel lumen (Figure 2A).
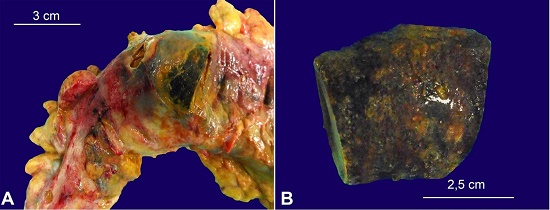
Figure 2
A – Gross view of the impacted stone in the sigmoid colon; B – Cylindrical surface of the stone from the sigmoid colon.
The external surface of the stone was yellow-black and had smooth to slightly irregular circular fractured ends (Figure 2B).
These fractured ends had concentric rings; the outer dark ring measured 0.4 cm, a yellow ring measured 0.7 cm, and a black to yellow center measured 1.7 × 1.5 cm (Figure 3B), which resembled one surface of the stone in the gallbladder. The walls of the sigmoid colon around the perforation were tan and edematous, and multiple diverticula were identified. The appendix was present.
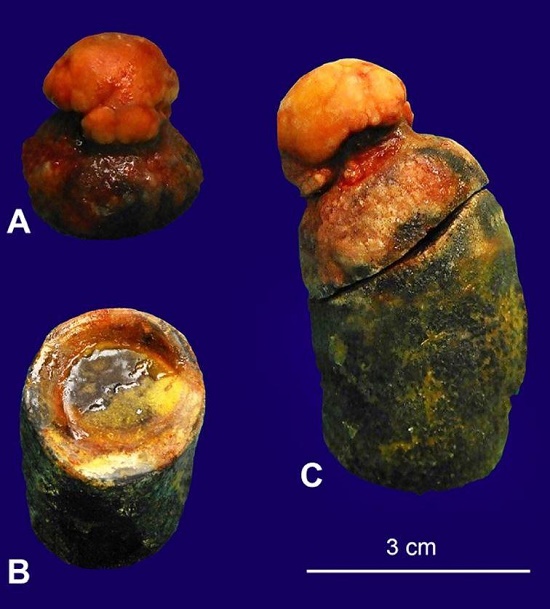
Figure 3
Gross view of the stones. A – Stone from the gallbladder; B – Fracture surface of the stone; C – Entire stone.
The liver weighed 1011 g (RR; 1540- 2030g); the capsule was gray-green, with a firm consistency on palpation and sectioning. The hepatic architecture appeared unremarkable. The gallbladder had a 4.0 × 4.0 cm artifactual perforation through a black and thickened wall. The lumen of the gallbladder contained a black-yellow, irregular 3.6 × 3.1 × 3.0 cm gallstone that appeared to be two stones fused to each other (Figure 3A). One component of the stone was cylindrical and the other was a more irregular oval, pale cap. The cylindrical stone had a fracture surface with concentric rings from an outer dark ring to a yellow ring to a black-to-yellow center. The black-to-yellow center measured 1.7 × 1.5 cm, a yellow ring measured 0.7 cm, and an outer black ring measured 0.4 cm, which corresponds to the dimensions of the stone from the sigmoid. The complete stone is depicted in Figure 3C.
Both kidneys were normal in size and weight. The capsules stripped with moderate difficulty. The kidney surfaces were pink-red, granular, and appeared lobulated. The kidneys were soft on section, and the cortices measured 0.4 cm. The cut surfaces had moderately increased peripelvic fat but were otherwise unremarkable.
The brain weighed 1080 g (RR; 1200–1600 g). The brain—including the proximal-most spinal cord and the dura—was examined after fixation. Grossly, the brain appeared to have moderate cerebral atrophy.
All tissues were fixed in buffered 10% formalin and processed to paraffin blocks in the conventional manner. Tissue sections were made, stained with hematoxylin and eosin and examined microscopically.
Microscopic examination of the gallbladder showed a thickened and fibrotic wall with dense infiltration by chronic inflammatory cells composed of lymphocytes and plasma cells. Sections from the sigmoid colon revealed denuded and autolyzed mucosal lining and features suggestive of acute colitis. No evidence of collagenous colitis was identified. The diverticula in the sigmoid colon, which were identified on gross examination, were confirmed histologically.
Microscopic examination of the heart revealed significant amyloid deposition not found in other postcranial organs. Sections from the lungs revealed centrilobular emphysema, respiratory bronchiolar fibrosis, and fibrointimal thickening in the pulmonary arteries. Congestion and edema were seen in two of the three sections. The third section had marked atelectasis.
The liver was moderately autolyzed with loss of lobular architecture. There was mild portal triaditis. Sections from the kidneys showed some glomeruli to be globally sclerotic but otherwise unremarkable. Moderate arterio- and arteriolosclerosis was present.
Microscopic examination of the brain revealed findings that were diagnostic of Alzheimer disease and were consistent with intermediate to advanced stage disease. Histopathologic findings accounted for clinically discernible dementia, intermediate to severe stage. Only mild amyloid angiopathy was seen in the brain with a moderate number of amyloid plaques in the cerebral cortex and white matter different from the amyloid deposition in the heart. Terminal, global hypoxic-ischemic change was identified. Patchy, less than 10% stenotic atherosclerosis was present. No other degenerative, inflammatory, infectious, or vascular disease processes were identified which would account for the patient’s dementia.
DISCUSSION
Gallstone ileus is a rare complication of gallstone disease. It is more common in patients over 65 (the average age was 72 years).1 Gallstones can erode through the wall of the gallbladder and penetrate the gastrointestinal tract where they may cause obstruction at any point along their course through the tract. They have a predilection to obstruct the smaller-caliber lumen of the small intestine (80.1%) or stomach (14.2%). Gallstones causing large bowel obstruction is rare (4.1%) and even more rarely can cause colonic perforation.2 Obstruction occurs when a single large stone or multiple small stones pass through a cholecystocolonic fistula. When a large stone measuring greater than 2.0 cm in diameter enters the colon through a cholecystocolonic fistula it impacts distally and can cause mechanical obstruction.3 Impaction usually occurs at a site of pathological narrowing, which may be a result of diverticular disease4,5 or pelvic irradiation.6 The presence of neoplasms, or intestinal strictures such as those secondary to Crohn disease, can also decrease the lumen size and may cause the gallstone to impact at the narrowing site. Our patient had a much larger stone and had severe diverticular disease with narrowed sigmoid colon, which predisposed her to impaction. Ischemia may develop at the site of gallstone impaction, due to the pressure generated against the bowel wall causing proximal distention. Necrosis and perforation followed by peritonitis may occur.
Patients typically present with abdominal pain due to acute cholecystitis followed by inflammation that leads to adhesions between the gallbladder and the hepatic flexure. The inflammation can progress to the development of a fistulous connection.3 This was clearly appreciated in our patient during autopsy although only adhesions remained where the fistula that had allowed the stone to penetrate the colon had been. The stone was found more distally in the transverse colon. Symptoms of gallstone ileus can be vague and insidious; therefore, a high index of clinical suspicion is required.
The Rigler triad of pneumobilia, dilated small bowel with paucity of air in the large bowel, and an opacity (gallstone) is seen on plain abdominal x-rays in less than 50% of cases.7 A CT scan is considered to be the gold standard for confirming the clinical diagnosis of gallstone ileus. It has a sensitivity of 93% and a specificity of 100%.8
Gallstone ileus is seen in elderly patients with other co-morbid conditions; therefore, surgery has a high risk of morbidity and mortality. A conservative management strategy can be an acceptable option, which includes colonic lavage/enema/cleansing; this was tried in our patient. Spontaneous passage of the gallstone was awaited as this has been reported in the literature.9-12 Surgery is the treatment of choice but it can be replaced by less invasive techniques, including colonoscopy, which can relieve the obstruction by fragmentation of the stone using lithotripsy.7,13,14 Laparoscopic enterolithotomy also has been used to circumvent surgery.13 These techniques are limited by the availability of local expertise and are dependent on the size and composition of the impacted stone.
In our patient, conservative management was adopted and multiple aggressive bowel cleansing attempts were made with no success in passing the gallstone. The patient experienced increased pain after an enema. By the third hospital day, she was hypotensive and septic with increasing abdominal pain. Surgical intervention or colonoscopy were not considered possible due to her age and other co-morbidities. The family agreed to comfort care and the patient passed away quietly. The immediate cause of death was peritonitis due to the perforated sigmoid colon caused by a large gallstone impacted in the narrowed sigmoid colon, which was the “perfect storm,” resulting from chronic cholecystitis and cholelithiasis, and severe diverticular disease.
A PubMed search yielded very few cases of colonic perforation caused by gallstones. All these cases underwent the Hartmann procedure.2 To the best of our knowledge, no autopsy case of colonic perforation at an impacted gallstone has so far been reported.
CONCLUSION
Gallstone ileus is such a rare complication of gallstone disease that it is not usually considered by the physician. However, delayed or missed diagnosis may have a fatal outcome. Therefore, a high index of clinical suspicion for gallstone ileus should prompt a CT scan to demonstrate a fistulous communication, intraluminal gallstone in the bowel, pneumobilia, and any other co-existing pathology contributing to the impaction and perforation of the gallstone. Gallstone ileus is a condition seen in older populations, usually with other co-morbid conditions; surgical management is associated with a high risk of morbidity and mortality. Non-surgical treatment has been suggested, including endoscopic removal and lithotripsy. In our case, the age and associated medical conditions of the patient helped the family to decide on comfort care and eventually autopsy, which confirmed the diagnosis. Early diagnosis and prompt management can prevent fatal outcomes in elderly patients who present late and have other comorbidities.
ACKNOWLEDGEMENTS
The authors acknowledge the assistance of Brian Kuszyk, MD, Affiliate Professor and Chair of Clinical Radiology, Brody School of Medicine, in obtaining the appropriate CT image and identifying the points of relevance.
References
Reisner RM, Cohen JR. Gallstone ileus: a review of 1001 reported cases. Am Surg. 1994;60(6):441-6. PMid:8198337
Halleran DR, Halleran DR. Colonic perforation by a large gallstone: A rare case report. Int J Surg Case Rep. 2014;5(12):1295-8. http://dx.doi.org/10.1016/j.ijscr.2014.11.058. PMid:25498567
Osman N, Subar D, Loh MY, Goscimski A. Gallstone ileus of the sigmoid colon: An unusual cause of large-bowel obstruction. HPB Surg. 2010;2010:153740. http://dx.doi.org/10.1155/2010/153740. PMid:20585361
Brown C. Colonic obstruction due to a gallstone. Br J Clin Pract. 1972;26(4):175-7. PMid:5036487
Buetow GW, Glaubitz JP, Crampton RS. Recurrent gallstone ileus. Surgery. 1963;54:716-24. PMid:14083576
Ishikura H, Sakata A, Kimura S, et al. Gallstone ileus of the colon. Surgery. 2005;138(3):540-2. http://dx.doi.org/10.1016/j.surg.2004.03.013. PMid:16213911
Athwal TS, Howard N, Belfield J, Gur U. Large bowel obstruction due to impaction of a gallstone. BMJ Case Rep. 2012;2012(feb07 1):bcr1120115100. http://dx.doi.org/10.1136/bcr.11.2011.5100. PMid:22665402
Yu CY, Lin CC, Shyu RY, et al. Value of CT in the diagnosis and management of gallstone ileus. World J Gastroenterol. 2005;11(14):2142-7. http://dx.doi.org/10.3748/wjg.v11.i14.2142. PMid:15810081
Foss HL, Summers JD. Intestinal obstruction from gallstones. Ann Surg. 1942;115(5):721-35. http://dx.doi.org/10.1097/00000658-194205000-00002. PMid:17858013
Tan YM, Wong WK, Ooi LLPJ. A comparison of two surgical strategies for the emergency treatment of gallstone ileus. Singapore Med J. 2004;45(2):69-72. PMid:14985844
Dumonceau JM, Delhaye M, Cremer M. Extracorporeal shock-wave lithotripsy for gallstone ileus. Gastrointest Endosc. 1996;44(6):759. http://dx.doi.org/10.1016/S0016-5107(96)70073-1. PMid:8979079
Salemans PB, Vles GF, Fransen S, Vliegen R, Sosef MN. Gallstone ileus of the colon: Leave no stone unturned. Case Rep Surg. 2013;2013:359871. http://dx.doi.org/10.1155/2013/359871. PMid:23970992
Zielinski MD, Ferreira LE, Baron TH. Successful endoscopic treatment of colonic gallstone ileus using electrohydraulic lithotripsy. World J Gastroenterol. 2010;16(12):1533-6. http://dx.doi.org/10.3748/wjg.v16.i12.1533. PMid:20333797
Bourke MJ, Scheider DM, Haber GB. Electrohydraulic lithotripsy of a gallstone causing gallstone ileus. Gastrointest Endosc. 1997;45(6):521-3. http://dx.doi.org/10.1016/S0016-5107(97)70186-X. PMid:9199914
Notes
Author notes
Correspondence Renuka Malenie East Carolina University Brody School of Medicine - Department of Pathology and Laboratory Medicine 600 Moye Blvd - Greenville/North Carolina – USA Zip Code: 27834-4300 Phone: 252-847-4495 malenier15@ecu.edu
Conflict of interest declaration