Clinical Case Report
Rare association between giant-cell aortitis and giant-cell aortic valvulitis
 Georgina del Cisne Jadán Luzuriaga geojadan@gmail.com
Ricardo Ribeiro Dias
Vagner Madrini
Walther Yoshiharu Ishikawa
Fabio Fernandes
Vera Demarchi Aiello
Georgina del Cisne Jadán Luzuriaga geojadan@gmail.com
Ricardo Ribeiro Dias
Vagner Madrini
Walther Yoshiharu Ishikawa
Fabio Fernandes
Vera Demarchi Aiello
Rare association between giant-cell aortitis and giant-cell aortic valvulitis
Autopsy and Case Reports, vol. 13, e2023449, 2023
Hospital Universitário da Universidade de São Paulo
Received: 18 May 2023
Accepted: 24 August 2023
ABSTRACT: Giant cell arteritis (GCA) is a type of chronic vasculitis that affects medium and large-caliber arteries, frequently related to aortic involvement and, consequently, to aneurysm formation. However, associated valvulitis with giant cells is uncommon. We describe the case of a 50-year-old female patient with aortic aneurysm and valvular insufficiency, whose anatomopathological examination revealed giant-cell aortic valvulitis associated with giant cell aortitis.
Keywords: Aorta, Thoracic, Aortic Diseases, Aortic Aneurysm, Aortic Valve, Aortic Valve Insufficiency.
INTRODUCTION
Giant cell arteritis (GCA) is a vasculitis involving medium and large-caliber arteries.1 It is a rare disease, affecting women over 50 years of age more often.2,3
Approximately 22% of patients with GCA have aortic involvement (aneurysm/dilation).4 In this condition, complications are associated with aortic valvar insufficiency secondary to aortic root dilation, aneurysm and/or aortic dissection, leading to heart failure and death in 20% of cases.5
We describe a case of a female patient with aortic aneurysm and valvular insufficiency, whose anatomopathological examination revealed giant-cell aortic valvulitis associated with giant-cell aortitis.
CASE REPORT
A 50-year-old Caucasian female with no personal or family history of pathological conditions presented with dyspnea on moderate and minor efforts, dizziness, and palpitations. On physical examination, there was an aspiration murmur in the aortic focus (2+/6+), with irradiation to the mitral and accessory aortic foci. Blood count, C-reactive protein, blood sedimentation speed, rheumatoid factor, anti-neutrophil cytoplasmic antibody, and renal function were normal. Serologies for hepatitis B, C, HIV, and syphilis were negative.
The electrocardiogram showed premature ventricular complexes. Chest radiography revealed dilation of the thoracic aorta. The echocardiogram revealed a left atrium of 42 mm, a left ventricle of 64 x 42 mm, and an ejection fraction of 62%, with significant aortic regurgitation and dilation of the ascending aorta.
On angiotomography, the aortic root measured 50 mm (Figure 1), the ascending segment 45 mm, the aortic arch 32 mm, the descending segment 22 mm, and the abdominal segment 17 mm. Surgery for aortic aneurysm correction was indicated. A coronary angiography was requested in the preoperative evaluation, excluding coronary obstructions.
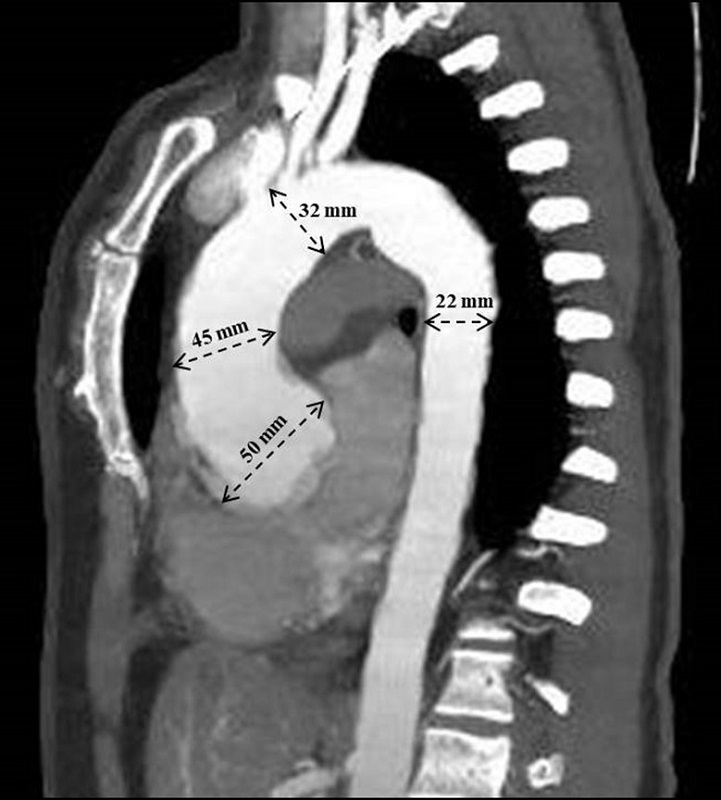
Figure 1
Contrast-enhanced chest CT angiography showing dilatation of the aortic root with a diameter greater than 50 mm in the ascending segment, the ascending segment 45 mm, the aortic arch 32 mm and the descending segment 22 mm.
Surgical intervention was performed with aortic root reconstruction and replacement of the ascending aorta (Bentall-De Bono procedure) using a valved tube with a mechanical aortic prosthesis.
The valve and the aortic aneurysmal segment were sent for anatomopathological analysis. The gross inspection of the aortic valve showed mild fibrous thickening at the free edge of the leaflets. Histological examination of the semilunar leaflets revealed a lymphohistiocytic infiltrate with giant cells, besides focal fibrinoid necrosis. Inflammatory cells were concentrated mainly at the ventricular aspect of the leaflets and spared their free edge. The diagnosis was giant-cell valvulitis with fibrinoid necrosis (Figure 2).
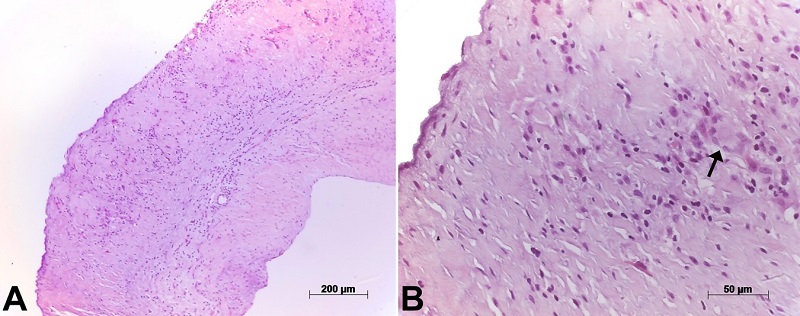
Figure 2
Photomicrographs of an aortic leaflet. In the panel A - with diffuse thickening and chronic inflammatory infiltrate; in the panel B - the arrows point to a Langerhans-type giant cell within the inflammatory infiltrate. Hematoxylin-eosin staining, objective magnifications 10x and 40x, respectively.
The aortic wall showed segmental destruction of elastic fibers of the medial layer and diffuse fibrointimal thickening, besides chronic inflammatory infiltrates with Langerhan-type giant cells, which concentrated at the external half of the wall, near the adventitial layer (Figures 3 and 4).
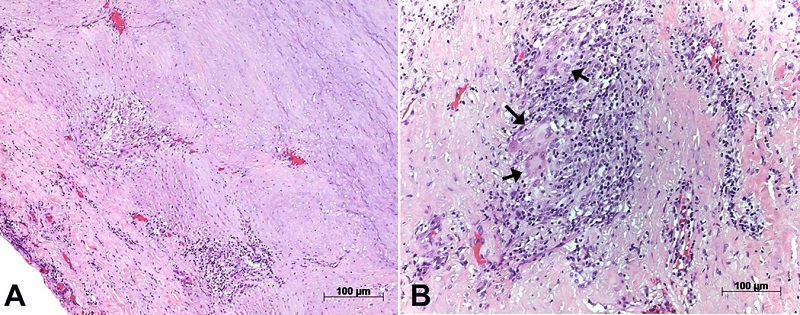
Figure 3
Photomicrographs of the aortic wall showing in panel A - the diffuse involvement of the layers by chronic inflammatory infiltrate; in panel B - a close-up view shows a giant cell within the inflammatory infiltrate. Hematoxylin-eosin staining, objective magnifications 5x and 40x respectively.
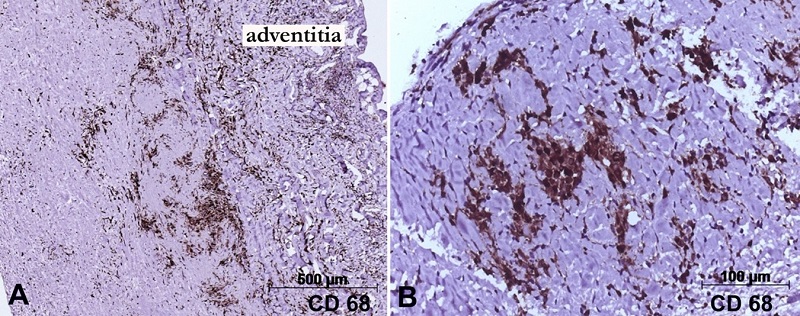
Figure 4
Photomicrographs of the aortic and valvar tissue submitted to immunohistochemical reactions for macrophages (CD68 antigen). In A - the positive cells are concentrated in the external half of the aortic wall, near the adventitia; Panel B - depicts positive macrophages in one aortic leaflet. Objective magnifications are respectively A - 5x; and B - 20x. Mouse monoclonal antibody CD68 (clone KP1), counter-staining with Harry’s Hematoxylin.
However, well-formed granulomas were not found, in the aortic wall and valvar tissue. Investigations for bacteria, acid-resistant bacilli, and fungi were negative in the valvar leaflets and the aortic wall (Brown-Hopps, Ziehl-Neelsen, and Grocott stains, respectively). CD68 immunostaining was strongly positive in the inflammatory foci in the aorta and valvar leaflets. Postoperative analysis of inflammatory markers showed no significant changes.
DISCUSSION
The present case describes the uncommon presentation of valvulitis associated with giant cells aortitis observed in the anatomopathological analysis.
When chronic aortitis leads to aortic root dilation, aortic valvar insufficiency usually occurs secondarily.6 In a previous review of 386 cases with thoracic aortic aneurysm and aortic insufficiency, only 2,6% were due to GCA, confirmed histopathologically.7 Likewise, in another series, from 7551 patients who underwent surgery for ascending or aortic arch disease, only 2% showed GCA on histologic examination.8
Involvement of the aortic valve by the same process as the one present in the aortic wall in GCA is sporadic and was first described by Niclauss et al.9 and Terré et al.10 from Paris also published inflammatory involvement of the aortic valve in GCA, however, in the form of non-infectious endocarditis, with mixed inflammatory infiltrate and absence of giant cells.
It is noteworthy that GCA does not affect the heart valves more frequently, even being a disease of the autoimmune rheumatologic group. However, such impairment may be more significant than reported in the literature since valve replacement is not always performed during GCA surgery.
A prospective study of biopsy or autopsy material in confirmed GCA cases could assess the prevalence of this type of associated inflammatory valvar involvement.
According to the Consensus Statement on Surgical Pathology of the Aorta, this form of aortitis was limited to GCA disease because there were no well-formed granulomas in the anatomopathological analysis, as in other types of arteritis. Likewise, no other clinical manifestations or laboratory or imaging results are suggestive of different forms of vascular disease.11
CONCLUSION
The involvement of the valve and the aortic arterial wall by GCA is an unusual association, and the diagnosis can be determined through the anatomopathological analysis of the specimens. Despite being infrequent, this combination also requires consideration in the differential diagnosis of disorders involving the aorta and aortic valve because its prevalence could be higher in patients who have not yet undergone surgical intervention and that could evolve into aortic syndromes and be life-threatening.
REFERENCES
Ciofalo A, Gulotta G, Iannella G, et al. Giant cell arteritis: pathogenesis, clinical aspects and treatment approaches. Curr Rheumatol Rev. 2019;15(4):259-68. http://dx.doi.org/10.2174/1573397115666190227194014. PMid:30827250.
Sehra ST, Setty A. Giant cell arteritis - a series of cases and review of literature. Curr Rheumatol Rev. 2013;9(2):138-43. http://dx.doi.org/10.2174/1573397111309020009. PMid:25409672.
Souza AWS, Okamoto KYK, Abrantes F, Schau B, Bacchiega ABS, Shinjo SK. Giant cell arteritis: a multicenter observational study in Brazil. Clinics. 2013;68(3):317-22. http://dx.doi.org/10.6061/clinics/2013(03)OA06. PMid:23644850.
García-Martínez A, Arguis P, Prieto-González S, et al. Prospective long term follow-up of a cohort of patients with giant cell arteritis screened for aortic structural damage (aneurysm or dilation). Ann Rheum Dis. 2014;73(10):1826-32. http://dx.doi.org/10.1136/annrheumdis-2013-203322. PMid:23873881.
Evans JM, Bowles CA, Bjornsson J, Mullany CJ, Hunder GG. Thoracic aortic aneurysm and rupture in giant cell arteritis. A descriptive study of 41 cases. Arthritis Rheum. 1994;37(10):1539-47. http://dx.doi.org/10.1002/art.1780371020. PMid:7864947.
Spence RK, Estella F, Gisser S, Schiffman R, Camishion RC. Thoracic aortic aneurysm secondary to giant cell arteritis: a reappraisal of etiology, treatment and possible prevention. J Cardiovasc Surg. 1985;26(5):492-5. PMid:4030882.
Gelsomino S, Romagnoli S, Gori F, et al. Annuloaortic ectasia and giant cell arteritis. Ann Thorac Surg. 2005;80(1):101-5. http://dx.doi.org/10.1016/j.athoracsur.2005.01.063. PMid:15975349.
Svensson LG, Arafat A, Roselli EE, et al. Inflammatory disease of the aorta: patterns and classification of giant cell aortitis, Takayasu arteritis, and nonsyndromic aortitis. J Thorac Cardiovasc Surg. 2015;149(2, Suppl):S170-5. http://dx.doi.org/10.1016/j.jtcvs.2014.08.003. PMid:25218529.
Niclauss L, Letovanec I, Chassot PG, Gersbach PA, von Segesser LK. Acute aortic valve insufficiency and cardiogenic shock due to an isolated giant cell inflammation of the aortic valve leaflets: case report and review of the literature. J Heart Valve Dis. 2008;17(3):343-7. PMid:18592933.
Terré A, Lidove O, Georges O, Mesnildrey P, Chennebault H, Ziza JM. Non-infective endocarditis: expanding the phenotype of giant cell arteritis. Joint Bone Spine. 2019;86(1):115-6. http://dx.doi.org/10.1016/j.jbspin.2018.04.002. PMid:29709695.
Stone JR, Bruneval P, Angelini A, et al. Consensus statement on surgical pathology of the aorta from the Society for Cardiovascular Pathology and the Association for European Cardiovascular Pathology: I. Inflammatory diseases. Cardiovasc Pathol. 2015;24(5):267-78. http://dx.doi.org/10.1016/j.carpath.2015.05.001. PMid:26051917.
Notes
Ethics statement: The authors retain informed consent signed by the patient authorizing the data publication.
Author notes
CorrespondenceGeorgina del Cisne Jadán Luzuriaga Universidade de São Paulo, Faculdade de Medicina, Instituto do Coração (InCor), Departamento de Miocardiopatias e Doenças da Aorta Av. Dr. Enéas Carvalho de Aguiar, 44, CEP 05403-000, São Paulo, SP, Brasil Phone: +55 (11) 2661-5000geojadan@gmail.com
Conflict of interest declaration