International Series: Adherence
Adherence: a review of education, research, practice and policy in Australia
Adherence: a review of education, research, practice and policy in Australia
Pharmacy Practice, vol. 7, no. 1, pp. 1-10, 2009
Centro de Investigaciones y Publicaciones Farmaceuticas
Received: 17 December 2008
Accepted: 10 February 2009
Aims: This article aims to describe the education, research, practice and policy in the area of adherence to therapy in Australia with a focus on community pharmacists.
Methods: A search of MEDLINE and International Pharmaceutical Abstracts as well as hand searches of the bibliographies of retrieved articles was conducted for the period 2000-2008. All pharmacy schools in Australia were also contacted to obtain information on the patient adherence to therapy content of their courses.
Results: Ten studies met the inclusion criteria. Only one study had a specific adherence focus, with the remainder including adherence support and monitoring as part of the overall interventions delivered by the community pharmacists. In the majority of cases the interventions resulted in an improvement in patients’ adherence to therapy. The research was supported by government and pharmacy professional organisation initiatives in the area of cognitive pharmaceutical services. All universities which responded delivered specific patient adherence courses.
Conclusions: Australian pharmacy schools are educating cohorts of students who will have the skills to monitor and support patient medication adherence in the context of contemporary pharmacy practice. This is supported by research evidence, government policy and fits well into the move to expand community pharmacy services to include chronic disease state management and primary health care.
Keywords: Medication Adherence+ Pharmacists+ Australia.
INTRODUCTION
Adherence to therapy is a challenge not only for patients, but also for health practitioners and researchers. Despite efforts to educate patients and provide interventions to address factors contributing to non-adherence, non-adherence and non persistence to therapy remain high, both across different populations and disease states. Adherence and persistence are influenced by many factors, and a single intervention is unable to address all issues resulting in non-adherence in all populations. A lack of consensus about the use and definitions of adherence (and compliance), the absence of a gold standard to measure adherence and the use of, primarily, self-report methods also introduce a bias in the results and further complicate adherence research and the assessment of interventions provided.
In addressing non-adherence and non persistence, a multidisciplinary approach to patient care is advocated. However to achieve this, health practitioners must be appropriately educated about how to identify barriers to adherence and support adherence. More importantly, there need to be national policies that promote patient adherence to therapy and support both research and interventions delivered by health practitioners. This article describes the education, research, practice and policy in the area of adherence to therapy in Australia with a focus on community pharmacists as the health practitioners.
METHODS
Adherence Education
All Australian pharmacy schools were contacted to collect information about their adherence programs.
Research in Adherence
Study Selection and Review
The databases MEDLINE and International Pharmaceutical Abstracts were searched, with the search being limited to Australia and the time period 2000-2008, as it is only in that past 9 years that adherence monitoring services and government and professional pharmacy organisation initiatives have emerged in the Australian setting. The following key words were used: “community pharmacist” or “pharmacist” or “community pharmacy” or “pharmacy” AND “adherence” or “compliance”; “pharmaceutical care” or “pharmaceutical services” or “disease state management” AND community pharmacist” or “pharmacist” or “community pharmacy” or “pharmacy”. Searches were also conducted based on the names of key Australian researchers in the areas of cognitive pharmaceutical services and disease state management. A hand search of the bibliographies of retrieved articles, as well as a search of the Research and Development projects funded through the Pharmacy Guild of Australia (http://beta.guild.org.au/research/funded_projects.a sp) was also conducted.
Each retrieved article was then reviewed based on the study design, description of the interventions provided, and outcome measures evaluated (with a focus on adherence measures).
The study was included if it was an intervention program delivered in a community pharmacy by the pharmacist to patients with a chronic disease; the intervention either directly or indirectly addressed adherence assessment, monitoring and support and adherence was either a direct study outcome measure or was measured indirectly. All study designs were included.
A total of 11 studies met the inclusion criteria and were reviewed.
RESULTS AND DISCUSSION
Adherence Education
Nine of the 16 Australian institutions responded. The majority offer a Bachelor of Pharmacy program which is a four-year undergraduate degree. Some institutions also offer the Master of Pharmacy degree, which is a two-year postgraduate degree. However, students completing either the Bachelor or Masters programs are still required to complete a 12 month pharmacy graduate training program prior to being eligible to register as pharmacists. The content of the degree programs is not prescribed by state or federal regulations or guidelines. However, all programs are accredited through the New Zealand and Australian Pharmacy Schools Accreditation Committee (NAPSAC).
Patient medication adherence, including definitions, causes of non-adherence and non persistence, measures of adherence, strategies to promote adherence and persistence and psychological models of non-adherence are taught in almost all of the Pharmacy degree programs across Australia. Table 1 provides examples of the curriculum content. The institutions appear to have similar programs though named differently, assessed differently and taught at various levels in the degree.
| University Name and State/ Territory | Degree | Year of Degree | Course | Content | Assessment |
|---|---|---|---|---|---|
| Charles Sturt University, New South Wales | BPharm | 4 | All pharmacy practice and professional practice courses | Definition and introduction to the concept and importance of adherence; strategies to improve adherence to non-pharmacotherapeutic interventions and to therapy. Dealing with patients in whom adherence is often an issue e.g. schizophrenia; bipolar disorder; alzheimer’s disease | Direct assessment of knowledge and the ability to link knowledge to practice; and application to case studies |
| Curtin University of Technology, Western Australia | BPharm | 3,4 | All Pharmacotherapy courses | Specific lectures on Patient Monitoring, Adherence and Communication; Problem Based Learning tutorials, where nonadherence is often a potential cause of the patient’s problem; discussion in the context of final year clinical practice placements with regard to patient interviews, case studies and patient management | Mid-semester tests, oral and written exams |
| Curtin University of Technology, Western Australia | M Clin Pharm | 2 | Clinical Pharmacy 527 and 528 | As per BPharm degree above | As per BPharm degree above |
| James Cook University, Queensland | BPharm | 1-4 | All pharmacy practice and professional units of study | Introductory aspects of adherence are dealt within years 1 and 2 as a component of the Practice Subjects with applications in years 3 and 4 both in terms of theory and practice in Clinical Dispensing and Placements | Workshops (on-course assessment); examination (written [including theory and case studies especially in years 3 and 4] and practice [clinical dispensing and OSCEs]) and in Clinical Placement activities |
| Griffith University, Queensland | BPharmSci | 2 | Drug Information and Evaluation 1 | Definitions, introduction to concepts and importance to health outcomes, health beliefs and behaviour change models, role of communication | Direct knowledge assessment via MCQs and written responses |
| Griffith University, Queensland | BPharmSci | 3 | Quality Use of Medicines | Introduction to initiatives and interventions to enhance adherence in hospital and community | Direct knowledge assessment via MCQs and written responses |
| Griffith University, Queensland | MPharm | 1 & 2 | Professional Pharmacy Practice 1, 2 & 3 | Causes, measures and strategies to enhance adherence to both pharmacotherapeutic and lifestyle measures | Ability to link knowledge to practice assessed via counselling and dispensing case studies |
| Queensland University of Technology, Queensland | BPharm | 1-4 | All Pharmacy Practice units | Definition of adherence, causes, identification of disease states with adherence issues. Integration of this content with Quality Use of Medicines and case scenarios in counselling workshops | Theory based assessment in addition to case scenarios for oral exams |
| University of Canberra, Australian Capital Territory | MPharm | 2 | Quality Use of Medicine 2 | Current Quality Use of Medicines (QUM) programs in Australia, adherence aspect of QUM | Major project to increase QUM in practice setting |
| University of Canberra, Australian Capital Territory | MPharm | 2 | Pharmacy Practice 1 | Identifying patients “at risk” of poor adherence, counselling and communication skills to promote adherence | Role play/oral examination |
| University of Sydney, New South Wales | BPharm | 1-4 | All Pharmacy Practice units of study | Introduction to the concept of adherence; detailed information on adherence, causes, measures and strategies; integrated in all cases in the final two years | Direct knowledge assessment, as well as application in cases assessed through role plays, OSCEs and written examinations |
| University of Sydney, New South Wales | MPharm | 2 | All Pharmacy Practice units of study | As per BPharm degree above | As per BPharm degree above |
| University of Tasmania, Tasmania | BPharm | 1, 3, 4 | All Pharmacy Practice units of study | Introduction to concept and some of the problems associated with poor adherence; detailed lectures and workshops on adherence, including definitions, measures and interventions; adherence is integrated in case-studies and dispensing practical classes in the final two years | Knowledge assessment, in addition to application in case-studies |
| University of Western Australia, Western Australia | MPharm | 1,2 | All pharmacy practice and pharmacy placement units of study | Introduction in Pharmacy Practice 1, followed by case studies in labs throughout the course that re-enforces the teaching | In dispensing labs |
Research Intervention Program Characteristics
Several studies demonstrated a positive impact of the community pharmacy delivered service on medication adherence1-8, measured predominantly by the use of validated self report questionnaires.9,10 No studies used the Medication Events Measuring System (MEMS) considered the gold standard for adherence measurement, possibly due to the cost of the devices.
The majority of studies used a parallel, controlled, repeated measures design (with 2 or more post-intervention data collection points) to strengthen the research design. In all studies the community pharmacy was recruited first, and the pharmacists then recruited patients (Table 2). Two studies reported using a randomised controlled design1,5 these were randomised at the pharmacy and not the patient level. It is recognised that conducting a true randomised controlled trial with a community pharmacy setting is not easy. Some studies experienced difficulty recruiting pharmacists, who in turn had difficulties recruiting patients.3,11 The low recruitment and high attrition rates compromise the research design and make statistical analyses difficult.
| Study characteristics | Intervention | Study Outcomes | Comments |
|---|---|---|---|
| Armour et al (1) Design: randomised, controlled, repeated measures; multi-site (across three states) Duration: 6 months Intervention: 26 community pharmacists, 165 patients Control: 24 community pharmacists, 186 patients | Pharmacy Asthma Care Plan: four visits involving assessment, monitoring and review, based on the Six-Step Asthma Management Plan (27) (counselling and education on asthma, triggers and medications including inhaler technique, adherence assessment and goal setting) | Improved adherence as measured by BMQ*, decrease in the proportion of patients with severe asthma, improved asthma quality of life, knowledge and perceived control, increased proportion of patients using a combination of reliever and preventer medications | Intervention delivered by trained community pharmacists. Monitoring adherence to medication was part of the overall service delivered. Pharmacists received remuneration for participation |
| Aslani et al (11) Design: parallel, controlled, repeated measures (Sydney metropolitan) Duration: 9 months Intervention: 19 community pharmacists, 48 patients Control: 19 community pharmacists, 49 patients | Therapeutics Outcome Monitoring Service for Hyperlipidaemia with a focus on adherence assessment, monitoring and strategy development | Significant reduction in total cholesterol levels, no change in adherence as measured with BMQ* and MARS** | Trained community pharmacists provided the intervention and received remuneration for participation |
| Benrimoj et al (2) Design: parallel, controlled, pre and post-intervention. Patients either randomly assigned to intervention and control groups, or non-randomly assigned to control group. Duration: 12 months retrospective data collected; 3 months post-intervention data collected 54 pharmacists in 9 study sites delivering services through 3 alternative healthcare models; metropolitan and rural settings | Patient medication management service (PMMS) and patient medication concordance service (PMCS) | Clinical (eg drug therapy changes) and economic (eg number and costs of drugs) impact data recorded by project pharmacists on study data collection forms: patients receiving PMMS showed reductions in drug related side effects (by 3.6%), improvements in symptoms (by 16.6%) and compliance (by 13.7%). PMCS resulted in significant reductions in drug related side effects (from 17.6% to 2.7%), and improvement in patient knowledge. PMMS resulted in a net medication cost saving of AUS$67.85 per patient | PMMS required referral of the patient by the general practitioner; PMCS was within the role of the pharmacist |
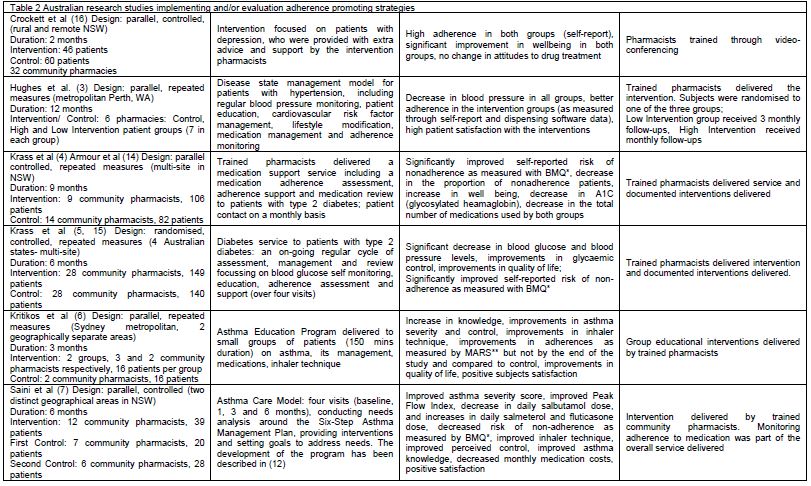
| Crockett et al (16) Design: parallel, controlled, (rural and remote NSW) Duration: 2 months Intervention: 46 patients Control: 60 patients 32 community pharmacies | Intervention focused on patients with depression, who were provided with extra advice and support by the intervention pharmacists | High adherence in both groups (self-report), significant improvement in wellbeing in both groups, no change in attitudes to drug treatment | Pharmacists trained through videoconferencing |
| Hughes et al. (3) Design: parallel, repeated measures (metropolitan Perth, WA) Duration: 12 months Intervention/ Control: 6 pharmacies: Control, High and Low Intervention patient groups (7 in each group) | Disease state management model for patients with hypertension, including regular blood pressure monitoring, patient education, cardiovascular risk factor management, lifestyle modification, medication management and adherence monitoring | Decrease in blood pressure in all groups, better adherence in the intervention groups (as measured through self-report and dispensing software data), high patient satisfaction with the interventions | Trained pharmacists delivered the intervention. Subjects were randomised to one of the three groups; Low Intervention group received 3 monthly follow-ups, High Intervention received monthly follow-ups |
| Krass et al (4) Armour et al (14) Design: parallel controlled, repeated measures (multi-site in NSW) Duration: 9 months Intervention: 9 community pharmacists, 106 patients Control: 14 community pharmacists, 82 patients | Trained pharmacists delivered a medication support service including a medication adherence assessment, adherence support and medication review to patients with type 2 diabetes; patient contact on a monthly basis | Significantly improved self-reported risk of nonadherence as measured with BMQ*, decrease in the proportion of nonadherence patients, increase in well being, decrease in A1C (glycosylated heamaglobin), decrease in the total number of medications used by both groups | Trained pharmacists delivered service and documented interventions delivered |
| Krass et al (5,15) Design: randomised, controlled, repeated measures (4 Australian states- multi-site) Duration: 6 months Intervention: 28 community pharmacists, 149 patients Control: 28 community pharmacists, 140 patients | Diabetes service to patients with type 2 diabetes: an on-going regular cycle of assessment, management and review focussing on blood glucose self monitoring, education, adherence assessment and support (over four visits) | Significant decrease in blood glucose and blood pressure levels, improvements in glycaemic control, improvements in quality of life; Significantly improved self-reported risk of nonadherence as measured with BMQ* | Trained pharmacists delivered intervention and documented interventions delivered. |
| Kritikos et al (6) Design: parallel, repeated measures (Sydney metropolitan, 2 geographically separate areas) Duration: 3 months Intervention: 2 groups, 3 and 2 community pharmacists respectively, 16 patients per group Control: 2 community pharmacists, 16 patients | Asthma Education Program delivered to small groups of patients (150 mins duration) on asthma, its management, medications, inhaler technique | Increase in knowledge, improvements in asthma severity and control, improvements in inhaler technique, improvements in adherences as measured by MARS** but not by the end of the study and compared to control, improvements in quality of life, positive subjects satisfaction | Group educational interventions delivered by trained pharmacists |
| Saini et al (7) Design: parallel, controlled (two distinct geographical areas in NSW) Duration: 6 months Intervention: 12 community pharmacists, 39 patients First Control: 7 community pharmacists, 20 patients Second Control: 6 community pharmacists, 28 patients | Asthma Care Model: four visits (baseline, 1, 3 and 6 months), conducting needs analysis around the Six-Step Asthma Management Plan, providing interventions and setting goals to address needs. The development of the program has been described in (12) | Improved asthma severity score, improved Peak Flow Index, decrease in daily salbutamol dose, and increases in daily salmeterol and fluticasone dose, decreased risk of non-adherence as measured by BMQ*, improved inhaler technique, improved perceived control, improved asthma knowledge, decreased monthly medication costs, positive satisfaction | Intervention delivered by trained community pharmacists. Monitoring adherence to medication was part of the overall service delivered |
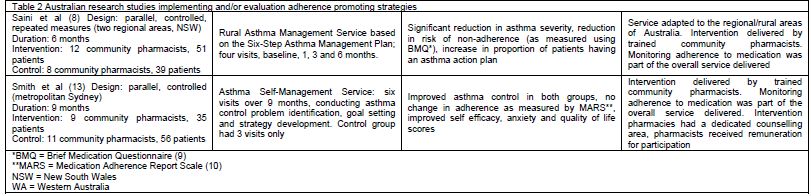
| Saini et al (8) Design: parallel, controlled, repeated measures (two regional areas, NSW) Duration: 6 months Intervention: 12 community pharmacists, 51 patients Control: 8 community pharmacists, 39 patients | Rural Asthma Management Service based on the Six-Step Asthma Management Plan; four visits, baseline, 1, 3 and 6 months. | Significant reduction in asthma severity, reduction in risk of non-adherence (as measured using BMQ*), increase in proportion of patients having an asthma action plan | Service adapted to the regional/rural areas of Australia. Intervention delivered by trained community pharmacists. Monitoring adherence to medication was part of the overall service delivered |
| Smith et al (13) Design: parallel, controlled (metropolitan Sydney) Duration: 9 months Intervention: 9 community pharmacists, 35 patients Control: 11 community pharmacists, 56 patients | Asthma Self-Management Service: six visits over 9 months, conducting asthma control problem identification, goal setting and strategy development. Control group had 3 visits only | Improved asthma control in both groups, no change in adherence as measured by MARS**, improved self efficacy, anxiety and quality of life scores | Intervention delivered by trained community pharmacists. Monitoring adherence to medication was part of the overall service delivered. Intervention pharmacies had a dedicated counselling area, pharmacists received remuneration for participation |
All but one2 of the studies had a disease focus for the interventions which were delivered by the community pharmacists. The majority focused on asthma1,6-8,12,13 with diabetes as the next most common disease state.4,14,15 Other areas included depression16 and cardiovascular disease.3,11 Improving adherence was not the primary outcome of any of the studies, but rather a means to produce better disease or risk factor control. All studies included some elements of patient education about the disease, therapy and monitoring, as well as lifestyle factors. In most cases the interventions included an assessment of patient’s beliefs and knowledge, patient goal setting, with a review of the goals at the planned patient visits to the pharmacy when the pharmacist would provide tailored strategies to optimise medication taking and improve therapeutic outcomes. The types of interventions implemented by researchers highlights the complex nature of adherence behaviour and the need for multiple strategies to support behaviour change. However, in one study, the pharmacists only delivered the intervention on a single occasion.6
In all reported studies, participating community pharmacists who delivered the interventions received training. In addition, in some studies pharmacists were remunerated for their services.1,8,11,13 Some interventions appeared complicated2 and not all authors provided a detailed description of the interventions delivered or how sustainable and reproducible they were outside the research studies.
POLICY AND PRACTICE OF ADHERENCE SERVICES
Following World Health Organization’s (WHO) leadership, Australia has been very active in the development and implementation of a National Drug Policy. The Australian Government launched its National Medicines Policy (NMP) in 1999. It focuses on four main objectives 1) timely access to medicines that Australians need at a cost that individuals and the community can afford, 2) medicines meeting appropriate standards of quality, safety and efficacy, 3) quality use of medicines, and 4) maintaining a responsible and viable medicines industry.17
The aspect of the NMP which pertains to compliance or adherence to medication is the Quality Use of Medicines (QUM) policy. Its aims are “to optimize the use of medicines to improve health outcomes for all Australians” through the “judicious selection of management options, appropriate choice of medicines where a medicine is considered necessary, and safe and effective use of medicines”.18 While the QUM policy does not specify adherence to medications per se, it is implicit in the notion of effective use of medicines.
Pharmacists in executing their professional responsibilities with respect to QUM have a key role in identifying and addressing non-adherence to medication. This has been recognised by official pharmacy organisations through a number of policies, practice standards and programs over recent years.19,20 For example the Pharmaceutical Society of Australia in its “Framework Document endorsed by all stakeholders in February 2001” for Home Medicines Review (HMR) refers to one of the purposes of HMR which is to identify consumer management issues such as continuing ceased medication; misuse, overuse or underuse of medicine; signs of non-adherence; and misunderstanding, confusion or problems with purpose or use.19 Indeed HMR is one of a number of professional pharmacy programs funded under 3rd (2000-2005) and 4th (2005-2010) Guild Government Agreements which have been introduced to community pharmacy by the Pharmacy Guild of Australia over the past decade.20 Most of these programs address adherence to medication as a component of the service. Services other than HMR include Dose Administration Aids (DAA), Patient Medication Profiling, and the Diabetes Medication Assistance Service (DMAS).
Home Medicines Review (HMR)
Introduced in 2001, the HMR is a consumer focused structured and collaborative health care service which involves the consumer, his/her general practitioner, his/her pharmacy and other relevant health care professionals. The program targets consumers at risk of medication related problems such as those on multiple medications or multiple daily doses, those with suspected non-adherence or inability to manage medication related therapeutic devices or recently discharged from hospital. The GP initiates the service by writing a referral to the local pharmacy and provides relevant clinical information including diagnoses, recent laboratory results and a list of prescribed medications to inform the pharmacist conducting the review. In the next phase, the pharmacist conducts an interview preferably in the consumer’s home and uses this as an opportunity to identify and address any gaps in consumer understanding of their medicines and barriers to medication adherence. Following this the pharmacist prepares a report for the GP with their findings and recommendations. The GP then discusses the report with their patient and considers any recommendations for changes to the regimen for the patient. A medication plan is produced by the GP and once agreed with the patient, a copy is sent to the preferred community pharmacist. The pharmacy is remunerated for each HMR (AUD 180; [92EUR]) and the GP receives a fee (AUD 134; [68EUR]). The service aims to improve the appropriate use of medicines and thereby improve patient outcomes.20 There are currently 1794 pharmacists in Australia accredited to deliver home medicines reviews.21 The data from Medicare Australia indicate that 189,108 HMRs have been claimed by health professionals.22
Dose Administration Aids (DAA)
If non adherence to medication or difficulty in managing the medication regimen are identified as issues, a suitable strategy is to supply the patient with a dose administration aid. In Australia, under the 4th Guild Government Agreement a new pharmacy program, the Dose Administration Aids (DAA) is paying community pharmacists to supply a dose administration aid to eligible community based patients enrolled in the program.23 Currently, the DAA program is in the implementation trial phase. During Phase 1 (July 1 2008 – 30 June 2009) specified data are collected for a minimum of five patients every three months and provided for the evaluation of the DAA Program. Pharmacists are eligible to receive incentive payments totalling AUS$8,900 when participating in Phase 1. The data collected during Phase 1 will be used to review patient eligibility and to develop a service and payment model to trial in Phase 2.24
Patient Medication Profile (PMP)
Another recent program to be introduced into community pharmacy under the 4th Guild Government Agreement is the Patient Medication Profile Program (PMP). Its aim is to assist eligible patients to better understand and manage their medicines and to provide a tool for communication between health care providers, such as pharmacists, GPs, allied health and community health careworkers, and the patient.
The PMP is a comprehensive summary of all regular medicines taken by a patient and must include complete information (brand, strength, dose, dose regimen, directions, prescriber) on all regular prescription medicines (including regular ‘when necessary’ medicines), regular over-the-counter and complementary medicines. It must also include patient details such as the patient’s name and address; date of birth, allergies or previous adverse drug reactions, and pharmacy contact details.
The PMP should provide space for the pharmacist to include additional advice or information and for additional comments to be annotated by different health care providers to facilitate effective inter-professional communication. An integral part of preparing the PMP is a patient consultation with a trained pharmacist which must take place in a suitable counselling area.
As with the DAA, the PMP Program is trialling the service within the community setting in a 2 phase process and will collect evaluation data to establish its benefits and sustainability. During Phase 1, incentives of up to AUD 4,200 [2,150EUR] (excluding Goods and Services Tax) are available to pharmacies for full participation in the PMP Program which comprises the collection and provision of evaluation data for a minimum of five patients every three months between July 2008 and July 2009. Pharmacists are also expected to charge patients AUD 5 [2.6EUR] per PMP per calendar year.25
Diabetes Medication Assistance Service (DMAS)
One of the Better Community Health Initiatives programs of the 4th Guild-Government Community Pharmacy Agreement which addresses medication adherence in a specific disease state is the Diabetes Pilot Program: Diabetes Medication Assistance Service (DMAS). Its aim is to assess the effectiveness and feasibility of a broader implementation of the Diabetes Medication Assistance Service within community pharmacy and its effect on the access to professional health support for eligible patients. The DMAS was trialled under the 3rd Guild-Government Community Pharmacy Agreement in people with type 2 diabetes and demonstrated improved diabetes control, an improved understanding of the long-term management of their diabetes and improved medication adherence.5,15
This service, focused on patients with type 2 diabetes, comprises a cycle of pharmacy visits which follow a defined protocol. Using a patient-centered approach, the pharmacist provides support to the patient to better self manage their diabetes by reviewing self-monitoring of blood glucose (SMBG) results with the patient, providing targeted disease, medication, and lifestyle information; giving adherence support; detecting drug-related problems; and making referrals as appropriate to the GP. At the end of each visit the patient with the help of the pharmacist will set a few key goals to improve self management to be reviewed at the next visit.
The program will be implemented in two stages. Evaluation of Stage 1 will focus on both process and outcome measures. The implementation process will be monitored with data collected on the recruitment rate of both pharmacies and patients. A wide range of clinical (e.g. HbA1c, BP, lipids, 10 year CV risk) and humanistic (quality of life and satisfaction) outcomes will be collected to determine the optimum number of visits to achieve the greatest improvements in diabetes.
Adherence Assessment Tool- MedsIndex®
This tool was developed by the Pharmacy Guild of Australia and launched in 2008. It computes a score out of 100 for up to five chronic medications in the patient computerized medication history by comparing actual refill intervals over expected refill intervals based on the dosage regimen. Thus it enables the pharmacist to identify potential non adherence and propose to their customer to enroll in one of the other professional pharmacy programs such as the DAA or the PMP (Figure 1).26
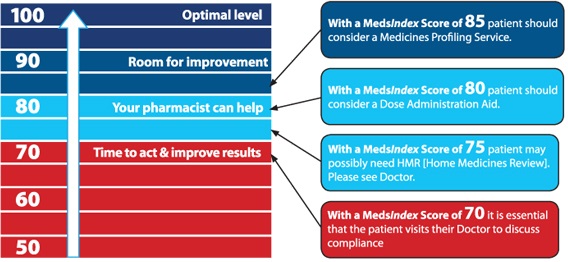
Figure 1
Recommended actions on the basis of the MedsIndex score
(http://www.medsindex.com.au/index.php/Content/what-ismedsindex.html)
CONCLUSIONS
Australian pharmacy schools are educating cohorts of students who will have the skills to monitor and support patient medication adherence in the context of contemporary pharmacy practice. This is supported by government policy and fits well into the move to expand community pharmacy services to include chronic disease state management and primary health care. A great deal of research has been conducted in the past 5-10 years on development, implementation and evaluation of disease specific interventions to be delivered by community pharmacists to their patients with chronic diseases, namely asthma, diabetes and cardiovascular diseases. Although these studies have shown a positive impact of the interventions on medication adherence as well as various health outcomes, the long term (more than 12 months) impact of these interventions is unknown, and an area which should be considered for further research.
References
Armour C, Bosnic-Anticevich S, Brillant M, Burton D, Emmerton L, Krass I, et al. Pharmacy Asthma Care Program (PACP) improves outcomes for patients in the community. Thorax. 2007;62(6):496-502.
Benrimoj S, Peacocke G, Whitehead P, Kopecny E, Ward P, Emerson L. Cognitive pharmaceutical services in emerging healthcare systems- new patient medication management and concordance services in community pharmacy. J Soc Admin Pharm. 2003;20(1):2-11.
Hughes J, Keen N, Dillon M, Maricic T. Hypertension: improving patient compliance and clinical outcomes through community pharmacist managed care. 2003. URL: http://www.guild.org.au/uploadedfiles/Research_and_Development_Grants_Program/Projects/2001-055_fr.pdf. (accessed 12 Dec. 08).
Krass I, Taylor S, Smith C, Armour C. Impact on medication use and adherence of Australian pharmacists' diabetes care services. J Am Pharm Assoc. 2005;45(1):33-40.
Krass I, Armour C, Taylor S, Hughes J, Peterson G, Stewart K, et al. The Pharmacy Diabetes Care Program. Final report to The Commonwealth Department of Health and Ageing as part of the Third Community Pharmacy Research and Development Grants Program. April 2005. URL: http://www.guild.org.au/uploadedfiles/Research_and_Development_Grants_Program/Projects/2002-518_fr.pdf (accessed 12 Dec. 08).
Kritikos V, Armour C, Bosnic-Anticevich S. Interactive small-group asthma education in the community pharmacy setting: a pilot study. J Asthma. 2007;44(1):57-64.
Saini B, Krass I, Armour C. Development, implementation and evaluation of a community pharmacy-based asthma care model. Ann Pharmacother. 2004;38(11):1954-1960.
Saini B, Filipovska J, Bosnic-Anticevich S, Taylor S, Krass I, Armour C. An evaluation of a community pharmacy-based rural asthma management service. Aust J Rural Health. 2008;16(2):100-108.
Svarstad B, Chewning B, Sleath B, Claesson C. The brief medication questionnaire: a tool for screening patient adherence and barriers to adherence. Patient Educ Counselling. 1999;37(2):113-124.
Horne R. The medication adherence report scale. Brighton, UK: University of Brighton; 2003.
Aslani P, Krass I, Chen T, Whitehead P, Rose G, editors. A community pharmacist delivered therapeutics outcome monitoring service for hyperlipidaemia. Sydney: The University of Sydney; 2006. URL: http://www.guild.org.au/uploadedfiles/Research_and_Development_Grants_Program/Projects/2002- 024%20Final%20version.pdf (accessed 30 January 2009)
Saini B, Smith L, Armour C, Krass I. An educational intervention to train community pharmacists in providing specialized asthma care. Am J Pharm Educ. 2006;70(5):118.
Smith L, Bosnic-Anticevich S, Mitchell B, Saini B, Krass I, Armour C. Treating asthma with a self-managment model of illness behaviour in an Australian community pharmacy setting. Soc Sci Med. 2007;64(7):1501-1511.
Armour C, Taylor S, Hourihan F, Smith C, Krass I. Implementation and evaluation of Australian pharmacists' diabetes care services. J Am Pharm Assoc. 2004;44(4):455-466.
Krass I, Armour CL, Mitchell B, Brillant M, Dienaar R, Hughes J, Lau P, Peterson G, Stewart K, Taylor S, Wilkinson J. The Pharmacy Diabetes Care Program: assessment the impact of a diabetes service model delivered by community pharmacists in Australia. Diabet Med. 2007;24(6):677-683.
Crockett J, Taylor S, Grabham A, Stanford P. Patient outcomes following an intervention involving community pharmacists in the management of depression. Aust J Rural Health. 2006 Dec;14(6):263-269.
Commonwealth Department of Health and Aged Care. National Medicines Policy. Canberra, ACT; 1999.
Commonwealth Department of Health and Ageing. The National Strategy for Quality Use of Medicines - Executive Summary. Canberra, ACT; 2002.
Pharmaceutical Society of Australia. Framework Document endorsed by all stakeholders in February 2001. URL: http://www.psa.org.au/site.php?id=1090 (accessed 15 July 2008).
Pharmacy Guild of Australia. Medication Management Review program. URL: http://www.guild.org.au/mmr/ (accessed 15 July 2008).
Pharmacy Guild of Australia, 2009. URL: http://www.guild.org.au/mmr/content.asp?id=2030 (accessed 2 February 2009).
Medicare Australia Statistics, Item Reports 2009. URL: https://www.medicareaustralia.gov.au/cgibin/ broker.exe?_PROGRAM=sas.mbs_item_standard_report.sas& SERVICE=default&DRILL=ag&_DEBUG=0&group=900&VAR=services&STAT=count&RPT_FMT=by+state&PTYPE=finyear&START_DT=199807&END_DT=200812(accessed 2 February 2009).
Pharmacy Guild of Australia. Dose Administration Aids URL: http://www.guild.org.au/pps/content.asp?id=1425 (accessed 15 July 2008).
Pharmacy Guild of Australia. Operations Manual: Dose Administration Aids Program. URL: http://www.guild.org.au/uploadedfiles/Professional_Pharmacy_Services/PPS_Programs/Dose_Administration_Aids/2_o perations_manual.pdf (accessed 15 July 2008).
Pharmacy Guild of Australia. Operations Manual: Patient Medication Profile Program. URL: http://www.guild.org.au/uploadedfiles/Professional_Pharmacy_Services/PPS_Programs/Medication_Profiling/pmp_oper ations_manual_020408.pdf (accessed 15 July 2008).
MedsIndex: A medicine compliance indicator. URL: http://www.medsindex.com.au/index.php/Content/what-ismedsindex. html (accessed 15 July 08).
National Asthma Council Australia. The asthma management handbook. Melbourne: National Asthma Council Australia; 2002.
Notes
None declared.