Review
The use of isotretinoin increases the risk of inflammatory bowel disease. A narrative review
El uso de isotretinoína aumenta el riesgo de enfermedad inflamatoria intestinal. Una revisión narrativa
 Juan Esteban Ospina-Gómez
María Paula Saavedra-Díaz
Juan Esteban Ospina-Gómez
María Paula Saavedra-Díaz
The use of isotretinoin increases the risk of inflammatory bowel disease. A narrative review
Iberoamerican Journal of Medicine, vol. 6, núm. 4, pp. 120-125, 2024
Hospital San Pedro
Recepción: 10 Abril 2024
Corregido: 04 Julio 2024
Aprobación: 23 Agosto 2024
Abstract:
Introduction: Acne vulgaris represents a prevalent dermatological condition capable of exerting a profound impact on an individual's quality of life. Isotretinoin, despite its wellestablished status as a highly effective remedy for severe acne, concerns surrounding the potential linkage with inflammatory bowel disease (IBD) have led to inquiries about its association.
Objective: The primary objective of this review is to critically assess the existing body of evidence pertaining to the efficacy and safety of isotretinoin, with a particular emphasis on its association with IBD.
Methods: A literature review was undertaken to examine the utilization of isotretinoin in the management of acne and to evaluate the subsequent risk of inflammatory bowel disease, aiming to determine the relevance of considering this factor when utilizing this treatment.
Conclusions: Isotretinoin is widely recognized as the most effective therapeutic approach to treat acne. This compound competently addresses all underlying factors contributing to acne pathogenesis. Over time, extensive deliberation has arisen concerning concerns related to its potential correlation with the onset of IBD. The currently available evidence conveys a paucity of substantial scientific support for a causal relationship between the use of isotretinoin and the development of IBD.
Keywords: Isotretinioin , Acne vulgaris , Inflammatory bowel disease.
Resumen:
Introducción: El acné vulgaris representa una afección dermatológica prevalente capaz de ejercer un profundo impacto en la calidad de vida de un individuo. La isotretinoina, a pesar de su estatus bien establecido como un fármaco altamente efectivo para el acné severo, las preocupaciones en torno a la posible asociación con la enfermedad inflamatoria intestinal (EII) han llevado a investigaciones sobre su seguridad.
Objetivo: El objetivo principal de esta revisión es evaluar de manera crítica el cuerpo existente de evidencia relacionada con la eficacia y seguridad de la isotretinoína, con un énfasis particular en su asociación con la EII.
Métodos: Se realizó una revisión de la literatura para examinar la utilización de la isotretinoina en el tratamiento del acné y evaluar el riesgo subsiguiente de enfermedad inflamatoria intestinal, con el objetivo de determinar la relevancia de considerar este factor al utilizar este tratamiento.
Conclusiones: La isotretinoína es ampliamente reconocida como el enfoque terapéutico más efectivo para tratar el acné. Este compuesto aborda de manera competente todos los factores subyacentes que contribuyen a la patogénesis del acné. Con el tiempo, ha surgido una extensa deliberación con respecto a preocupaciones relacionadas con su posible correlación con el inicio de la EII. La evidencia científica actualmente disponible muestra un vacío significativo, que respalde un vínculo causal entre el uso de la isotretinoina y la aparición de la EII.
Palabras clave: Isotretinoina , Acne vulgaris, Enfermedad inflamatoria intestinal.
INTRODUCTION
Acne is a chronic inflammatory dermatological condition that affects the pilosebaceous unit, which includes the hair follicle, hair shaft, and sebaceous gland [1]. Globally, around 650 million people suffer from acne, with higher prevalence in regions such as Western Europe, North America, and South America [2]. This condition predominantly manifests during adolescence, affecting over 95% of adolescent males and approximately 85% of adolescent females [3, 4]. In the United States, it is estimated that 85% of individuals aged 12 to 25-experience acne [5, 6, 7].
The pathogenesis of acne involves a complex interplay of factors including androgen-induced stimulation of sebaceous glands, alterations in the pilosebaceous follicle microbiome, and innate and cellular immune responses [8, 9]. Key pathogenic factors include follicular hyperkeratinization, increased sebum production, the presence of Cutibacterium acnes, and inflammation [10, 11].
Androgens play a crucial role in acne development by promoting the growth and activity of sebaceous glands, leading to increased sebum production that creates an environment conducive to C. acnes. Immune responses to C. acnes contribute to inflammation and lesion formation [12]. Genetic predisposition also influences acne severity and variability in immune response and bacterial strains [13, 14].
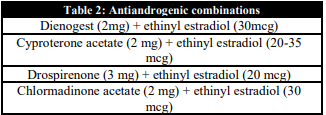
Treatment of acne should be tailored to the specific pathophysiology and patient characteristics, as summarized in Table 1, which outlines various treatment modalities and their mechanisms of action [15]. Hormonal treatments are considered for cases of hyperandrogenism, late-onset acne, perimenstrual exacerbations, or resistance to other therapies [16]. Oral contraceptives work by reducing androgen production through suppression of luteinizing hormone (LH), increasing sex hormone-binding globulin (SHBG) to lower free testosterone, inhibiting 5-alpha reductase activity, and blocking androgen receptors to mitigate androgen effects. Table 2 lists the most common antiandrogenic combinations used in these treatments [16]. Antibiotic treatments, including tetracyclines, are also outlined in Table 3, typically used at non-antimicrobial doses [17].


For severe acne, isotretinoin is often recommended, particularly for cases involving nodules, cysts, or inflammatory acne with a high risk of scarring [18]. However, concerns about isotretinoin's side effects, including its potential association with Inflammatory Bowel Disease (IBD), have prompted further research [19].
The aim of this review is to critically assess the available evidence regarding the efficacy and safety of isotretinoin, with a particular focus on its relationship with IBD.
ISOTRETINOIN IN THE MANAGEMENT OF ACNE
Isotretinoin, also referred to as 13-cis-retinoic acid, constitutes a naturally occurring derivative of vitamin A. Formulations for its application are available in both topical and oral forms. In 1982, the United States Food and Drug Administration granted the approval for oral isotretinoin in treating nodulocystic acne. Subsequently, in 1983, its usage also garnered the endorsement of the European Medicines Agency (EMA). Since then, the lives of numerous acne patients have been significantly enhanced by isotretinoin [20].
Across time, isotretinoin has brought about a transformation in the realm of acne therapy and continues to be acknowledged by the medical community as the most clinically effective anti-acne treatment. According to the European guidelines, the indications for the utilization of oral isotretinoin encompass severe acne manifestations, specifically nodular and conglobate presentations, regardless of responses to prior treatments. It is the primary preference for individuals contending with severe forms of acne, including cystic and nodular phenotypes, as well as any type of acne linked to active scarring. It is imperative to underscore that all acne lesions, not solely cysts and nodules, harbor the potential to induce permanent scarring. Consequently, isotretinoin emerges as a viable alternative when initial treatments prove unproductive [21].
The mode of action of isotretinoin exhibits a distinct capacity to address comprehensively all fundamental factors contributing to the onset of acne. It results in a notable reduction in the production of sebum and the dimensions of sebaceous glands, which yields effective suppression of Propionibacterium acnes and a concomitant reduction in inflammation associated with acne [22].
Generally, isotretinoin is administered at a daily dosage ranging from 0.5 to 1.0 mg/kg of body weight, with most patients experiencing substantial improvements within a span of 16 weeks [23]. The consumption of isotretinoin with a fatty meal is advisable to optimize its absorption. In situations of severe acne, initial doses of a lesser magnitude may be employed alongside oral corticosteroids to mitigate the risk of severe outbreaks and scarring, a condition known as fulminant pseud acne. Typically, the objective is to reach a cumulative dosage within the range of 120 to 150 mg/kg over a period of 4 to 6 months to curtail the likelihood of relapses [24].
Nonetheless, prior to treatment initiation, the performance of laboratory tests becomes imperative, encompassing lipid profiles and liver function assessments. These evaluations must be executed both at the onset of therapy and approximately in the second month, particularly as the maximum daily dosage is attained. Significantly, heightened triglyceride levels emerge as the laboratory abnormality most frequently detected in isotretinoin-treated patients, with normalization typically ensuing upon completion of treatment [25].
Isotretinoin is associated with several potential side effects, including dryness of the lips, skin, and eyes. Elevations in liver enzyme levels are a commonly observed occurrence, which typically revert to baseline upon treatment cessation. Less frequent side effects encompass headaches and joint and muscle discomfort, which are generally manageable. Although initial concerns regarding psychiatric side effects existed, current evidence suggests an uncertain and controversial connection between isotretinoin and psychiatric issues [26].
IS THERE A RELATIONSHIP BETWEEN THE USE OF ISOTRETINOIN AND INFLAMMATORY BOWEL DISEASE?
The potential relationship between isotretinoin and IBD, encompassing both Crohn's disease and ulcerative colitis, has been the subject of continuous debate, supported by limited evidence. Guidelines issued by the U.S. working group in 2016 assert that the current evidence is insufficient to confirm an association or causal link between isotretinoin and IBD [27]. Canadian guidelines provide some information based on studies regarding the potential correlation between isotretinoin and IBD development. They suggest that before initiating isotretinoin treatment, it would be advisable to inquire about IBD symptoms and assess relevant family history while addressing the ongoing debate on this matter. However, these guidelines do not provide a conclusive recommendation on the subject [28]. In contrast, European S3 guidelines do not offer specific recommendations concerning the relationship between oral isotretinoin and IBD [29].
Considering the most robust and currently available information, a comprehensive analysis of the risk of developing IBD associated with isotretinoin was conducted through a meta-analysis encompassing studies published up to July 2015 [30].
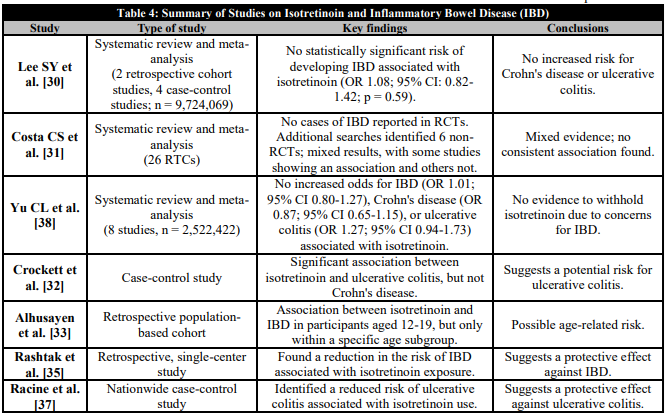
In parallel, in a comprehensive systematic review conducted by Cochrane, the effectiveness and safety of oral isotretinoin as an acne treatment were assessed based on the best available evidence [31].This review, which comprised 26 RCTs, did not report any cases of IBD. In addition to the RCTs, supplementary searches for non-RCT related to adverse effects were conducted, and the references of the RCTs were reviewed, leading to the identification of six non-RCT investigating the relationship between oral isotretinoin and the risk of IBD. Among these studies, Crockett et al. [32] identified a significant association between oral isotretinoin and ulcerative colitis (though not with Crohn's disease), while Alhusayen et al. [33] found a link between oral isotretinoin and IBD in participants aged 12 to 19, but only within a predefined age range subgroup. In contrast, the other four studies [34, 35, 36, 37] did not reveal an increased incidence of IBD in relation to oral isotretinoin use. In 2014, Rashtak et al. [35] found even a reduction in the risk of IBD associated with isotretinoin exposure, and Racine et al. [37] identified that isotretinoin use was linked to a reduced risk of ulcerative colitis. It is important to note that there was no assessment of bias risk or evaluation of the quality of evidence in these studies related to oral isotretinoin and IBD. Additionally, it is reported that no reports of serious adverse effects were found in other non-RCT reviewed during the additional selection process.
The most recent systematic review and meta-analysis, which included eight studies (four case-control and four cohort studies) with a total of 2,522,422 participants found no increased odds for IBD among patients receiving isotretinoin (OR 1.01; 95% confidence interval [CI] 0.80-1.27). Nor did the meta-analysis find increased odds for either Crohn disease (OR 0.87; 95% CI 0.65-1.15) or ulcerative colitis (OR 1.27; 95% CI 0.94-1.73) associated with isotretinoin exposure. The sensitivity and subgroup analyses produced similar results. In TSA, the Z-curve reached the futility boundaries when using relative risk reduction thresholds ranging from 5% to 15% and argues that Isotretinoin should not be withheld because of unnecessary concerns for the development of IBD [38]. Finally, reviewing other articles, they also maintain that there is not a consistent association between isotretinoin use and risk of inflammatory bowel disease. There is no clear evidence of a causal link [39, 40, 41]. See Table 4 for a summary of these studies.
CONCLUSIONS
Acne is a multifaceted dermatological condition that necessitates a tailored approach to treatment. Various therapeutic options are available, with isotretinoin emerging as a highly effective treatment for severe cases, particularly nodular and conglobate forms, along with any acne types associated with active scarring. It stands out as the sole therapy addressing all critical factors contributing to acne development. When considering isotretinoin therapy, healthcare professionals should conduct a comprehensive evaluation of each patient's medical history and assess the severity of their acne. Treatment should be individualized, and potential risks must be carefully weighed. Monitoring for adverse effects should be continuous throughout the treatment period.
Based on the most rigorous and up-to-date scientific evidence, it is evident that concerns regarding the potential causal association between isotretinoin use and IBD lack substantial scientific support. The prevailing data strongly suggests that the advantages of utilizing isotretinoin in the treatment of severe acne far surpass the risk of IBD onset. Furthermore, isotretinoin remains a pivotal component in the management of severe acne, markedly enhancing the quality of life for numerous individuals grappling with this condition. Overall, isotretinoin continues to play a crucial role in the management of severe acne, significantly improving the quality of life for many individuals affected by this condition. Patient-specific assessments and ongoing monitoring are essential to ensure the safe and effective use of this medication.
CONFLICT OF INTERESTS
The authors have no conflict of interest to declare. The authors declared that this study has received no financial support.
REFERENCES
1.Kaminsky A, Florez-White M, Arias MI, Bagatin E. Classification of acne: An Ibero-Latin American Consensus, 2014. Med Cutan Iber Lat Am. 2015;43(1):18-23.
2.Gollnick HP, Finlay AY, Shear N; Global Alliance to Improve Outcomes in Acne. Can we define acne as a chronic disease? If so, how and when? Am J Clin Dermatol. 2008;9(5):279-84. doi: 10.2165/00128071-200809050-00001.
3.Ramrakha S, Fergusson DM, Horwood LJ, Dalgard F, Ambler A, Kokaua J, et al. Cumulative mental health consequences of acne: 23-year follow-up in a general population birth cohort study. Br J Dermatol. 2016;175(5):1079-81. doi: 10.1111/bjd.13786.
4.Sutaria AH, Masood S, Saleh HM, Schlessinger J. Acne Vulgaris. 2023 Aug 17. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–.
5.Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2163-96. doi: 10.1016/S0140-6736(12)61729-2.
6.Burton JL, Cunliffe WJ, Stafford I, Shuster S. The prevalence of acne vulgaris in adolescence. Br J Dermatol. 1971;85(2):119-26. doi: 10.1111/j.1365-2133.1971.tb07195.x.
7.Ghodsi SZ, Orawa H, Zouboulis CC. Prevalence, severity, and severity risk factors of acne in high school pupils: a community-based study. J Invest Dermatol. 2009;129(9):2136-41. doi: 10.1038/jid.2009.47.
8.Lynn DD, Umari T, Dunnick CA, Dellavalle RP. The epidemiology of acne vulgaris in late adolescence. Adolesc Health Med Ther. 2016;7:13-25. doi: 10.2147/AHMT.S55832.
9.Collier CN, Harper JC, Cafardi JA, Cantrell WC, Wang W, Foster KW, et al. The prevalence of acne in adults 20 years and older. J Am Acad Dermatol. 2008;58(1):56-9. doi: 10.1016/j.jaad.2007.06.045.
10.Sharma S, Khaitan BK, Kumarasinghe SP. Cutaneous Signs in Dermatological Diseases; An Overview. Indian J Dermatol. 2021;66(5):530-9. doi: 10.4103/ijd.ijd_141_21.
11.Hay RJ, Johns NE, Williams HC, Bolliger IW, Dellavalle RP, Margolis DJ, et al. The global burden of skin disease in 2010: an analysis of the prevalence and impact of skin conditions. J Invest Dermatol. 2014;134(6):1527-34. doi: 10.1038/jid.2013.446.
12.Del Rosso JQ, Kircik L. The primary role of sebum in the pathophysiology of acne vulgaris and its therapeutic relevance in acne management. J Dermatolog Treat. 2024;35(1):2296855. doi: 10.1080/09546634.2023.2296855.
13.Herane MI, Ando I. Acne in infancy and acne genetics. Dermatology. 2003;206(1):24-8. doi: 10.1159/000067819.
14.Evans DM, Kirk KM, Nyholt DR, Novac C, Martin NG. Teenage acne is influenced by genetic factors. Br J Dermatol. 2005;152(3):579-81. doi: 10.1111/j.1365-2133.2005.06387.x.
15.Habeshian KA, Cohen BA. Current Issues in the Treatment of Acne Vulgaris. Pediatrics. 2020;145(Suppl 2):S225-S230. doi: 10.1542/peds.2019-2056L.
16.Nast A, Rosumeck S, Erdmann R, Alsharif U, Dressler C, Werner RN. Methods report on the development of the European evidence-based (S3) guideline for the treatment of acne - update 2016. J Eur Acad Dermatol Venereol. 2016;30(8):e1-e28. doi: 10.1111/jdv.13783.
17.Layton A. The use of isotretinoin in acne. Dermatoendocrinol. 2009;1(3):162-9. doi: 10.4161/derm.1.3.9364.
18.Dessinioti C, Zouboulis CC, Bettoli V, Rigopoulos D. Comparison of guidelines and consensus articles on the management of patients with acne with oral isotretinoin. J Eur Acad Dermatol Venereol. 2020;34(10):2229-40. doi: 10.1111/jdv.16430.
19.Vallerand IA, Lewinson RT, Farris MS, Sibley CD, Ramien ML, Bulloch AGM, et al. Efficacy and adverse events of oral isotretinoin for acne: a systematic review. Br J Dermatol. 2018;178(1):76-85. doi: 10.1111/bjd.15668.
20.Layton AM, Dreno B, Gollnick HP, Zouboulis CC. A review of the European Directive for prescribing systemic isotretinoin for acne vulgaris. J Eur Acad Dermatol Venereol. 2006;20(7):773-6. doi: 10.1111/j.1468-3083.2006.01671.x.
21.Gollnick HP, Bettoli V, Lambert J, Araviiskaia E, Binic I, Dessinioti Cet al. A consensus-based practical and daily guide for the treatment of acne patients. J Eur Acad Dermatol Venereol. 2016;30(9):1480-90. doi: 10.1111/jdv.13675.
22.Leyden JJ, Del Rosso JQ, Baum EW. The use of isotretinoin in the treatment of acne vulgaris: clinical considerations and future directions. J Clin Aesthet Dermatol. 2014;7(2 Suppl):S3-S21.
23.Nast A, Bayerl C, Borelli C, Degitz K, Dirschka T, Erdmann R, et al. [S2k-guideline for therapy of acne]. J Dtsch Dermatol Ges. 2010;8 Suppl 2:s1-59. doi: 10.1111/j.1610-0387.2010.07466.x.
24.Coates P, Adams CA, Cunliffe WJ, McGinley KT, Eady EA, Leyden JJ, et al. Does oral isotretinoin prevent Propionibacterium acnes resistance? Dermatology. 1997;195 Suppl 1:4-9; discussion 38-40. doi: 10.1159/000246012.
25.Villani A, Nastro F, Di Vico F, Fabbrocini G, Annunziata MC, Genco L. Oral isotretinoin for acne: a complete overview. Expert Opin Drug Saf. 2022;21(8):1027-37. doi: 10.1080/14740338.2022.2102605.
26.Kaminsky A. Less common methods to treat acne. Dermatology. 2003;206(1):68-73. doi: 10.1159/000067824.
27.Zaenglein AL, Pathy AL, Schlosser BJ, Alikhan A, Baldwin HE, Berson DS, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2016;74(5):945-73.e33. doi: 10.1016/j.jaad.2015.12.037.
28.Asai Y, Baibergenova A, Dutil M, Humphrey S, Hull P, Lynde C, et al. Management of acne: Canadian clinical practice guideline. CMAJ. 2016;188(2):118-26. doi: 10.1503/cmaj.140665.
29.Nast A, Rosumeck S, Erdmann R, Alsharif U, Dressler C, Werner RN. Methods report on the development of the European evidence-based (S3) guideline for the treatment of acne - update 2016. J Eur Acad Dermatol Venereol. 2016;30(8):e1-e28. doi: 10.1111/jdv.13783.
30.Lee SY, Jamal MM, Nguyen ET, Bechtold ML, Nguyen DL. Does exposure to isotretinoin increase the risk for the development of inflammatory bowel disease? A meta-analysis. Eur J Gastroenterol Hepatol. 2016;28(2):210-6. doi: 10.1097/MEG.0000000000000496.
31.Costa CS, Bagatin E, Martimbianco ALC, da Silva EM, Lúcio MM, Magin P, et al. Oral isotretinoin for acne. Cochrane Database Syst Rev. 2018;11(11):CD009435. doi: 10.1002/14651858.CD009435.pub2.
32.Crockett SD, Porter CQ, Martin CF, Sandler RS, Kappelman MD. Isotretinoin use and the risk of inflammatory bowel disease: a case-control study. Am J Gastroenterol. 2010;105(9):1986-93. doi: 10.1038/ajg.2010.124.
33.Alhusayen RO, Juurlink DN, Mamdani MM, Morrow RL, Shear NH, Dormuth CR, et al. Isotretinoin use and the risk of inflammatory bowel disease: a population-based cohort study. J Invest Dermatol. 2013;133(4):907-12. doi: 10.1038/jid.2012.387.
34.Etminan M, Bird ST, Delaney JA, Bressler B, Brophy JM. Isotretinoin and risk for inflammatory bowel disease: a nested case-control study and meta-analysis of published and unpublished data. JAMA Dermatol. 2013;149(2):216-20. doi: 10.1001/jamadermatol.2013.1344.
35.Rashtak S, Khaleghi S, Pittelkow MR, Larson JJ, Lahr BD, Murray JA. Isotretinoin exposure and risk of inflammatory bowel disease. JAMA Dermatol. 2014;150(12):1322-6. doi: 10.1001/jamadermatol.2014.1540.
36.Bernstein CN, Nugent Z, Longobardi T, Blanchard JF. Isotretinoin is not associated with inflammatory bowel disease: a population-based case-control study. Am J Gastroenterol. 2009;104(11):2774-8. doi: 10.1038/ajg.2009.417.
37.Racine A, Cuerq A, Bijon A, Ricordeau P, Weill A, Allemand H, et al. Isotretinoin and risk of inflammatory bowel disease: a French nationwide study. Am J Gastroenterol. 2014;109(4):563-9. doi: 10.1038/ajg.2014.8.
38.Yu CL, Chou PY, Liang CS, Chiang LH, Wang TY, Tu YK, et al. Isotretinoin Exposure and Risk of Inflammatory Bowel Disease: A Systematic Review with Meta-Analysis and Trial Sequential Analysis. Am J Clin Dermatol. 2023;24(5):721-30. doi: 10.1007/s40257-023-00765-9.
39.Coughlin SS. Clarifying the Purported Association between Isotretinoin and Inflammatory Bowel Disease. J Environ Health Sci. 2015;1(2):10.15436/2378-6841.15.007. doi: 10.15436/2378-6841.15.007.
40.Miqdad MA, Alatta L, Abdelsamad A, Fouda S, Cherukuri ASS, Eltanany M, et al. Isotretinoin-Induced Inflammatory Bowel Disease: Is There a Real Association? Cureus. 2022;14(10):e29825. doi: 10.7759/cureus.29825.
41.Barbieri JS. Isotretinoin and risk of inflammatory bowel disease: More data to support lack of meaningful risk. J Am Acad Dermatol. 2021;84(1):228-9. doi: 10.1016/j.jaad.2020.07.041.
Notas de autor
colmedgroup.bga@gmail.com
Información adicional
redalyc-journal-id: 6920