Original article
Recepción: 29 Julio 2024
Corregido: 23 Octubre 2024
Aprobación: 18 Noviembre 2024
DOI: https://doi.org/10.53986/ibjm.2025.0003
Abstract:
Introduction: Vitamin B12 is essential for erythropoiesis, cell proliferation, nucleoprotein and myelin synthesis, and normal growth and development of cognitive functions.
Material and methods: A retrospective cohort follow-up study is planned to determine vitamin B12 levels and to reveal the symptoms that occur in deficiency. A complete blood count is conducted as part of the standard protocol for pregnant women (third trimester) of pregnancy. At six months of age, the infant's serum vitamin B12 level, iron concentration, ferritin level, and complete blood count are assessed. 70 mother-baby pairs were followed up over the period from 01/01/2021 to 01/01/2022. The infant cohort included 51.4% boys (n=36) and 48.6% girls (n=34).
Results: It was observed that 58.5% (n=41) of the mothers used multivitamin supplements, and 80% of them used iron medication. When the babies of mothers who took a multivitamin containing B12 were compared with the babies of other mothers, it was observed that there was a statistical significance in the B12 levels of the babies (p=0.012).
Discussion: The effects of B12 supplementation given to mothers on the intelligence development of children were investigated. It was hypothesised that the recommendation to provide routine vitamin B12 supplementation to mothers could be incorporated into the existing guidelines. The concept was initially proposed during the course of the study. It is our view that the administration of vitamin B12 supplements to mothers has a beneficial effect on the vitamin B12 levels of their babies, and that vitamin B12 supplementation should be provided to mothers. Studies conducted in our country and in the world show that keeping the vitamin B12 level high during pregnancy and lactation is important for the health of the mother and baby. It is therefore recommended that pregnant women receive vitamin B12 supplementation, with continued supplementation for the first six months postpartum.
Keywords: Infant, Vitamin B12 , Exclusive breastfeeding, Pregnancy , Anemia.
Resumen:
Introducción: La vitamina B12 es esencial para la eritropoyesis, la proliferación celular, la síntesis de nucleoproteínas y mielina, y el crecimiento y desarrollo normales de las funciones cognitivas.
Material y métodos: Se planifica un estudio de seguimiento de cohorte retrospectiva para determinar los niveles de vitamina B12 y revelar los síntomas que ocurren en la deficiencia. Se realiza un hemograma completo como parte del protocolo estándar para mujeres embarazadas (tercer trimestre) del embarazo. A los seis meses de edad, se evalúa el nivel sérico de vitamina B12 del bebé, la concentración de hierro, el nivel de ferritina y el hemograma completo. Se realizó un seguimiento de 70 parejas madre-bebé durante el período del 01/01/2021 al 01/01/2022. La cohorte de bebés incluyó un 51,4% de niños (n = 36) y un 48,6% de niñas (n = 34).
Resultados: Se observó que el 58,5% (n = 41) de las madres usaban suplementos multivitamínicos y el 80% de ellas usaba medicación con hierro. Cuando se compararon los bebés de madres que tomaron un multivitamínico que contenía B12 con los bebés de otras madres, se observó que había una significación estadística en los niveles de B12 de los bebés (p = 0,012).
Discusión: Se investigaron los efectos de la suplementación de B12 administrada a las madres sobre el desarrollo de la inteligencia de los niños. Se planteó la hipótesis de que la recomendación de proporcionar una suplementación de vitamina B12 de forma rutinaria a las madres podría incorporarse a las directrices existentes. El concepto se propuso inicialmente durante el curso del estudio. En nuestra opinión, la administración de suplementos de vitamina B12 a las madres tiene un efecto beneficioso sobre los niveles de vitamina B12 de sus bebés, y que se debe proporcionar suplementación de vitamina B12 a las madres. Los estudios realizados en nuestro país y en el mundo muestran que mantener el nivel de vitamina B12 alto durante el embarazo y la lactancia es importante para la salud de la madre y el bebé. Por lo tanto, se recomienda que las mujeres embarazadas reciban suplementos de vitamina B12, con una suplementación continua durante los primeros seis meses después del parto.
Palabras clave: Infancia, Vitamina B12, Lactancia materna exclusiva, Embarazo, Anemia.
INTRODUCTION
Vitamin B12 (cyanocobalamin) is a water-soluble vitamin that has important functions for body metabolism. It serves as a crucial cofactor for the synthesis of methionine. Furthermore, methionine is essential for the synthesis of s-adenosylmethionine, a crucial methyl donor within the organism. Consequently, it plays a pivotal role in the methylation of phospholipids, DNA, RNA, and neurotransmitters [1].
Vitamin B12 is especially found in foods of animal origin, such as meat, eggs, fish, and milk and dairy products. The daily dietary intake (RDA) for the first six months of life is 0.4 mcg. While the daily requirement for adults is 2.4 mcg, this requirement can increase up to 2.6 mcg in pregnancy and 2.8 mcg in lactation. Those who consume diets lacking in animal products, including strict vegetarians, are at risk of developing vitamin B12 deficiency [2].
Although the prevalence of vitamin B12 deficiency varies between countries throughout the world, it has been reported to be 6%-80%, more frequently in developing countries [3].During pregnancy, there is a gradual decrease in serum concentration of vitamin B12 and it is difficult to determine the prevalence. Worldwide deficiency can range from 5% (<28 days gestation) to 72% (just before birth) depending on the gestational week. The incidence of vitamin B12 deficiency in early childhood varies between 6-25%. The 2017 Turkish Nutrition and Health Survey indicates that the average intake of vitamin B12 is within the recommended range [4]. However, vitamin B12 deficiency is a common problem in pregnant women, mothers and children in our country. In a study by Halıcıoğlu et al. [5] in Turkey, the incidence of B12 deficiency in pregnant women in low socioeconomic regions was found to be 47.6%. In another study conducted by Koç et al [6], B12 deficiency was found in 72% of mothers and 41% of children, and severe vitamin B12 deficiency was found in 48% of mothers and 23% of children. It is obvious that vitamin B12 deficiency is a common problem.
According to the recommendation of the World Health Organization, all babies should be exclusively breastfed for the first six months. The content of some micronutrients in breastmilk (such as thiamine, riboflavin, vitamin B6, vitamin B12, choline, retinol, vitamin A, vitamin D and selenium) varies depending on the mother's intake, and it is predicted that the content in breastmilk will be inadequate if the mother is fed poorly in these micronutrients [7]. For this reason, vitamin B12 deficiency is an important problem in infants fed only with breastmilk if the mother's stores are insufficient [8, 9].Children above the 95th percentile have lower B12 levels. More vitamin B12 supplementation is needed [10].
Studies on vitamin B12 levels during pregnancy and early infancy have shown that low serum levels are generally high. As a result, increased homocysteine and methylmalonic acid in pregnancy bring fetal complications. These include intrauterine growth retardation, neural tube defects and preterm births. In some studies, possible immune system dysfunctions were also shown. In infants with vitamin B12 deficiency, findings such as growth retardation, skin hyperpigmentation, diarrhea, vomiting, seizures, hypotonia, motor development retardation, irritability and tremor are observed [11].
It is known that the resulting vitamin B12 deficiency may lead to disorders in neurological and cognitive functions in the long term. Although improvement in hematological parameters is achieved with treatment, if the deficiency is severe and persists for a long time, there may not be complete improvement in neurological findings. In this case, neurological sequelae may remain in infants [12]. Therefore, early detection and treatment of vitamin B12 deficiency in pregnant women and adequate vitamin B12 supplementation by mothers during pregnancy may be an effective step in preventing vitamin B12 deficiency in infants.
Prenatal multivitamin preparations, which are recommended in routine practice in Turkey and covered by the social security institution, contain 2.5 mcg of vitamin B12. In addition, vitamin B12 deficiency, which is common in our country, is not routinely screened during pregnancy. To date, no study has been conducted to assess the efficacy of the vitamin B12 content of multivitamin supplements recommended for pregnant women in our country in preventing vitamin B12 deficiency in mothers and babies. The effect of women taking this level of supplement during pregnancy on postpartum vitamin B12 levels in breastmilk is also unknown. Considering the nutritional practices of our country, vitamin B12 deficiency is observed in infants receiving only breastmilk.
In this study, we will present the original design model, which will be used to retrospectively evaluate the serum vitamin B12 levels of mothers and children from the early pregnancy period. Additionally, we will investigate the parameters affecting these levels. It will be possible to reveal causality for the results that will emerge with the study. Thus, eliminating the negative effects of vitamin B12 deficiency, which is on the list of preventable diseases, will enable a healthier generation to grow. This may also contribute to the reduction of health expenditures.
MATERIAL AND METHODS
A retrospective cohort follow-up study is planned to determine vitamin B12 levels and to reveal the symptoms that occur in deficiency, University of Health Sciences, Sancaktepe Training and Research Hospital, İstanbul, Turkey. Ethics committee approval numbered E-46059653-020-550 was received from the hospital's ethics committee unit on 17/06/2020. Complete blood count is routinely checked in pregnant women who come to the outpatient clinic in the last trimester of pregnancy (≥28 weeks according to the last menstrual period). The study will evaluate the demographic and nutritional characteristics of pregnant women with anaemia in their haemogram, serum iron and ferritin levels indicative of iron deficiency, and vitamin B12 levels suggestive of vitamin B12 deficiency. For pregnant women with vitamin B12 deficiency, 1000 mcg B12 replacement therapy for two weeks, three days a week will be administered parenterally. Multivitamin preparation (Omega3 (DHA) 200 mg, Omega 3 (EPA) 40 mg, Iodine 150 mcg, Vit D3 5 mcg, folic acid 400 mcg, Selenium 55 mcg, Zinc 10 mg, Vit B1 1.1 mg, Vit B2 1.4 mg, Vit B3 16 mg, Vit B122.5 mcg) daily use will be recommended. The mothers participating in the study will be called regularly every fortnight and questioned whether they use the multivitamin preparation regularly.
At six months of age, the infant's serum vitamin B12 level, iron and ferritin levels, and complete blood count are assessed in accordance with the recommendations of the World Health Organization (WHO) and the American Academy of Pediatrics (AAP) during a routine outpatient examination [12]. Simultaneous serum vitamin B12, iron, ferritin, and complete blood counts are checked in the mother. Examination results of the cases will be evaluated retrospectively.
In addition, the educational status, number of pregnancies, and nutritional habits of the mothers participating in the study (vegetarian history, frequency of consumption of red meat, offal, chicken, fish, fruit, legumes, eggs, and green leafy vegetables) were questioned.
The socioeconomic levels of the families were evaluated with questions prepared using the 5-point Likert scale. While evaluating the socio-economic conditions of our country, the current minimum wage (17000 Turkish Lira), hunger threshold (20000 Turkish Lira), poverty threshold (70000 Turkish Lira) were taken as basis, and the socio-economic conditions of the families were evaluated using a 5-point Likert scale. A socio-economic level (SEL) was assigned to each income bracket based on the following criteria: 17,000 TL and below was classified as low SEL, 17,001-20,000 TL as low-moderate SEL, 20,001-50,000 TL as moderate SEL, 50,001-70,000 TL as moderate-high SEL, and 70,001 TL and above was classified as high SEL.
The hemogram values of the study (XT-2000I; Symex, Osaka, Japan) were analyzed using an automated hematology device. Serum ferritin was measured by the electrochemiluminescence immunoassay method (ECLIA), and iron was measured by the photometric test method.
SERUM VITAMIN B12 MEASUREMENT
Vitamin B12 level will be measured by electrochemiluminescence immunological method (Modular Analytics, E170 analyzer, Roche Diagnostics, Germany).
The diagnostic cut-off values to be used in the study were determined as follows:
· <150 pmol/L (<203 pg/mL): deficiency.
· 150–220 pmol/L (203-300 pg/mL): borderline deficiency.
· >220 pmol/L (>300 pg/mL): normal.
SAMPLE
The population of the study consists of women who will give birth in our hospital. The number of births occurring annually at our hospital is estimated to be approximately 4,500–5,000. Assuming that regularly used prenatal vitamin B12 supplementation will reduce the vitamin B12 deficiency seen in infants by 50%, the sample size was calculated as 50 mothers (20-45 age)-infant pairs by accepting 90% strength and type 1 error 0.05. Considering the possibility of giving birth in other hospitals and the socio-cultural dynamics in the location of our hospital, it was initially aimed to reach approximately 100 pregnant women, since approximately 50% loss is expected due to poor regular drug use habits and low stability in participation in clinical trials.
We followed up 70 mother and baby couple of cases that we followed on 01/01/2021-01/01/2022. The infants included in the study were 51.4% (n=36) boys and 48.6% (n=34) girls.
VARIABLES OF THE STUDY
Dependent variable of the study: Serum vitamin B12 levels of mothers and their babies.
Independent variables of the study: Socioeconomic level of mothers, mother's treatment for vitamin B12 deficiency
STATISTICAL ANALYSIS
SPSS program (Version 21, Chicago, SPSS Inc., USA) will be used for statistical analysis and data recording. Indescriptive statistics, mean±standard deviation (SD) for parametric values, median (median), minimum (min), maximum (max) fornon-parametric values, n number and percentage (%) values for frequency analyses expressing frequency will be written. The conformity of the data to the normal distribution will be tested with the Kolmogorov-Smirnov test. In comparing two groups, a variety of statistical tests may be employed, depending on the nature and distribution of the data in question. Quantitative data is often analysed using tests such as the t-test, Mann-Whitney U test, Kruskal-Wallis test or one-way ANOVA, while qualitative data is typically assessed using the Chi-Square test for independent groups and McNemar test for dependent groups. Pearson or Spearman test will be used for correlation in correlation analysis, and linear or logistic regression tests will be used in modelling. For statistical significance, cases where the p-value is below 0.05 will be accepted.
EXCLUSION CRITERIA
Pregnant women with vitamin B12 levels within the normal range (300 pg/ml), patients with absorption disorders such as Imerslund-Grasbeck who were followed up in the hematology clinic, and patients with chronic diseases were excluded from the study.
RESULTS
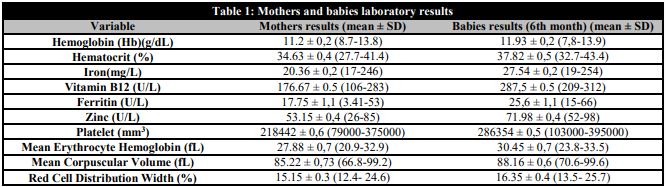
The infants included in the study were 51.4% (n=36) boys and 48.6% (n=34) girls. Laboratory parameters (mean, the lowest and the highest values) of the mothers and babies participating in our study are presented in Table 1.
Mothers and babies laboratory results
The mean age of pregnant women was 24.6±4.4 years. 60% (n=42) of pregnant women were classified as having a low socioeconomic level (SEL), while 22.8% (n=16) were assigned to the low-moderate SEL category, 10% (n=7) to the moderate SEL category, 4.3% (n=3) to the moderate-high SEL category, and 2.9% (n=2) to the high SEL category. The majority of participants (51.4%, n=36) were primary school graduates, while 35.8% (n=25) were secondary school graduates and 12.8% (n=9) received a higher education. Of the pregnant women, 48.5% (n=34) were experiencing their first pregnancy, 31.5% (n=22) were pregnant for the second time, 11.4% (n=8) were pregnant for the third time, 5.8% (n=4) were pregnant for the fourth time, and 2.8% (n=2) were pregnant for a fifth or higher number of times. There was no statistical significance between the low socioeconomic levels of the mothers and B12 levels (p=0.06). It was thought that the inclusion of families with low-income levels of mothers in the study was effective. It was observed that 58.5% (n=41) of the mothers used multivitamin supplements and 80% (n=56) used iron supplements. A comparison of the infants of mothers who used multivitamins containing vitamin B12 and received B12 treatment with those of other mothers revealed a statistically significant difference in B12 levels in 74.2% of cases (n=52; p=0.012). A comparison of the infants of mothers who received zinc supplements with those of other mothers revealed a statistically significant difference between the two groups in terms of level in 52.8% of cases (n=37; p=0.064). There was no statistically significant difference in hemoglobin between the babies of mothers who used iron supplements and the babies of mothers who did not use iron supplements (p=0.055). Statistical data of the cases are presented in Table 2.
Characteristics of the patients

DISCUSSION
Prenatal nutrition of the mother and nutrition of the child in the first two years (1000 days) play a very important role in the child’s neurodevelopment and lifelong mental health. Although all nutrients are necessary for the growth of the brain, the main nutrients that support neurodevelopment include protein; zinc; iron; choline; and folate; iodine; vitamins A, D, B6 and B12; and long-chain polyunsaturated fatty acids. Failure to provide essential nutrients during this critical period of brain development can result in lifelong deficits in brain function despite subsequent nutritional supplementation [13].
In a randomized, double-blind, placebo-controlled study of 800 pregnant Nepali women, Chandyo et al. administered 50 µg of vitamin B12 or a placebo to the subjects from the early stages of pregnancy until the latest point of 15 weeks to 6 months. The Bayley Scale of Infant and Toddler Development was measured at 6 and 12 months of age, and growth (height and weight) at 6 and 12 months [14]. The effects of B12 supplementation given to mothers on the intelligence development of children were investigated. It was thought that the recommendation to give routine vitamin B12 supplementation to mothers could be added to the current guidelines. We set out with this idea while doing the study. It is our contention that the administration of vitamin B12 supplements to pregnant women is an effective means of ensuring adequate vitamin B12 levels in the fetus. Therefore, we recommend the provision of vitamin B12 supplementation to pregnant women.
Pregnant women in resource-poor are at risk for multiple micronutrient deficiencies and low vitamin indicators. Vitamin B12 status has been associated with adverse pregnancy outcomes, including anemia, low birth weight, and intrauterine growth retardation. In Bangalore, India pregnant women were given<14 weeks of gestation, supplementation with vitamin B12 (50 mg) until the sixth postpartum week, and another group was given a placebo concurrently. All women were given iron and folic acid supplements throughout the process. Compared with those taking a placebo, women supplemented with vitamin B12 had significantly higher plasma vitamin B12 [15].
In the study by Siddiqua et al., Bangladeshi women (n=68, 18-35 years old, hemoglobin <110 g/L, 11-14 weeks pregnant) were randomized to receive 250 μg/day B12 or placebo throughout pregnancy and 60 mg iron + It was given up to three months after birth with 400 μg folate. Supplementation of 250 µg/day B12 during pregnancy and lactation has been shown to significantly improve maternal, infant and breastmilk B12 level [16].
The study by Bae et al. revealed that pregnancy and lactation consistently resulted in alterations to vitamin B12 status, with an increased supply of vitamin B12 to the child. The administration of a vitamin B12 dose (∼3 times the RDA) in the study resulted in an increase in the bioactive form of vitamin B12. This suggests that reproductive-age women may potentially derive benefit from vitamin B12 intake in accordance with current recommendations [17].
In the study of Dror et al., it was emphasized that supplementation of 50–250 µg vitamin B-12/day during pregnancy and lactation increases the concentrations of vitamin B12 in breast milk [18].
In the study conducted by Hazar Sayar et al. in Edirne, Turkey, 250 pregnant women who applied to the Obstetrics and Gynecology Department for delivery and their healthy babies born at 38-42 weeks of gestation and their healthy babies were included. The levels of vitamin B12 and folic acid in newborns were found to be correlated with those in their mothers [19].
In the study conducted by Karabulut et al. in Denizli, Turkey, iron and vitamin B12 deficiencies were found to be relatively common in the pregnant population consuming a vegetable-based diet. It was emphasized that pregnant women in Turkey should be given iron and vitamin B12 supplements in addition to folate [20].
The prevalence of anemia in Turkey is quite high in adolescence and in the reproductive age of 15-49 years. The cause of anemia in Turkey is mostly nutritional. To prevent anemia, it is necessary to pay attention to nutrition. Vitamin supplements such as Vitamin B12 and folate should be given to women during pregnancy [20, 21].
CONCLUSIONS
Our study shows that keeping vitamin B12 levels high during pregnancy and breastfeeding is important for the health of the mother and the baby. The mother should be supplemented with vitamin B12 during pregnancy and supplementation should be continued in the first 6 months. It will be possible to reveal the ideal amount of supplementation with comprehensive studies.
CONFLICT OF INTERESTS
The authors have no conflict of interest to declare. The authors declared that this study has received no financial support.
REFERENCES
1.Henjum S, Manger M, Hampel D, Brantsæter AL, Shahab-Ferdows S, Bastani NE, et al. Vitamin B12 concentrations in milk from Norwegian women during the six first months of lactation. Eur J Clin Nutr. 2020;74(5):749-56. doi: 10.1038/s41430-020-0567-x.
2.Aparicio E, Jardí C, Bedmar C, Pallejà M, Basora J, Arija V, et al. Nutrient Intake during Pregnancy and Post-Partum: ECLIPSES Study. Nutrients. 2020;12(5):1325. doi: 10.3390/nu12051325.
3.Allen LH. How common is vitamin B-12 deficiency? Am J Clin Nutr. 2009;89(2):693S-6S. doi: 10.3945/ajcn.2008.26947A.
4.Erdoğan Gövez N, Akpınar Şentüre Ş, Ayten Ş, Köksal E. Evaluation of the Turkey Nutrition and Health Surveys according to the mediterranean adequacy index and sustainability through water footprints. Public Health Nutr. 2023;26(12):2927-2935. doi: 10.1017/S1368980023001957.
5.Halicioglu O, Sutcuoglu S, Koc F, Ozturk C, Albudak E, Colak A, et al. Vitamin B12 and folate statuses are associated with diet in pregnant women, but not with anthropometric measurements in term newborns. J Matern Fetal Neonatal Med. 2012;25(9):1618-21. doi: 10.3109/14767058.2011.648244.
6.Koc A, Kocyigit A, Soran M, Demir N, Sevinc E, Erel O, et al. High frequency of maternal vitamin B12 deficiency as an important cause of infantile vitamin B12 deficiency in Sanliurfa province of Turkey. Eur J Nutr. 2006;45(5):291-7. doi: 10.1007/s00394-006-0598-7.
7.Allen LH. B vitamins in breast milk: relative importance of maternal status and intake, and effects on infant status and function. Adv Nutr. 2012;3(3):362-9. doi: 10.3945/an.111.001172.
8.Honzik T, Adamovicova M, Smolka V, Magner M, Hruba E, Zeman J. Clinical presentation and metabolic consequences in 40 breastfed infants with nutritional vitamin B12 deficiency--what have we learned? Eur J Paediatr Neurol. 2010;14(6):488-95. doi: 10.1016/j.ejpn.2009.12.003.
9.Dağ H, Koç MÖ, Dikker O, Dursun H. Vitamin B12 Serum Levels of Six to Nine-month old Infants According to Feeding Practices. J Pediatr Res. 2020;7(1):1-6. doi: 10.4274/jpr.galenos.2019.00377.
10.Doğan M. Evaluation of vitamin B12 and vitamin D levels in primary school-age children According to different body mass index percentages. The Injector, 2023;2(3):197-202. doi: 10.5281/zenodo.8408534.
11.Demir N, Koc A, Üstyol L, Peker E, Abuhandan M. Clinical and neurological findings of severe vitamin B12 deficiency in infancy and importance of early diagnosis and treatment. J Paediatr Child Health. 2013;49(10):820-4. doi: 10.1111/jpc.12292.
12.Ruangkit C, Prachakittikul N, Hemprachitchai N, Dumrongwongsiri O, Soonsawad S. Association of Infant Feeding Practices with Iron Status and Hematologic Parameters in 6-Month-Old Infants. Children (Basel). 2021;8(12):1159. doi: 10.3390/children8121159.
13.Schwarzenberg SJ, Georgieff MK; COMMITTEE ON NUTRITION. Advocacy for Improving Nutrition in the First 1000 Days to Support Childhood Development and Adult Health. Pediatrics. 2018;141(2):e20173716. doi: 10.1542/peds.2017-3716.
14.Chandyo RK, Ulak M, Kvestad I, Shrestha M, Ranjitkar S, Basnet S, et al. The effects of vitamin B12 supplementation in pregnancy and postpartum on growth and neurodevelopment in early childhood: Study Protocol for a Randomized Placebo Controlled Trial. BMJ Open. 2017;7(8):e016434. doi: 10.1136/bmjopen-2017-016434.
15.Duggan C, Srinivasan K, Thomas T, Samuel T, Rajendran R, Muthayya S, et al. Vitamin B-12 supplementation during pregnancy and early lactation increases maternal, breast milk, and infant measures of vitamin B-12 status. J Nutr. 2014;144(5):758-64. doi: 10.3945/jn.113.187278.
16.Siddiqua TJ, Ahmad SM, Ahsan KB, Rashid M, Roy A, Rahman SM, et al. Vitamin B12 supplementation during pregnancy and postpartum improves B12 status of both mothers and infants but vaccine response in mothers only: a randomized clinical trial in Bangladesh. Eur J Nutr. 2016;55(1):281-93. doi: 10.1007/s00394-015-0845-x.
17.Bae S, West AA, Yan J, Jiang X, Perry CA, Malysheva O, et al. Vitamin B-12 Status Differs among Pregnant, Lactating, and Control Women with Equivalent Nutrient Intakes. J Nutr. 2015;145(7):1507-14. doi: 10.3945/jn.115.210757.
18.Dror DK, Allen LH. Vitamin B-12 in Human Milk: A Systematic Review. Adv Nutr. 2018;9(suppl_1):358S-366S. doi: 10.1093/advances/nmx019.
19.Sayar EH, Orhaner BB, Sayar E, NesrinTuran F, Küçük M. The frequency of vitamin B12, iron, and folic acid deficiency in the neonatal period and infancy, and the relationship with maternal levels. Turk Pediatri Ars. 2020;55(2):139-48. doi: 10.14744/TurkPediatriArs.2020.14042.
20.Karabulut A, Sevket O, Acun A. Iron, folate and vitamin B12 levels in first trimester pregnancies in the Southwest region of Turkey. J Turk Ger Gynecol Assoc. 2011;12(3):153-6. doi: 10.5152/jtgga.2011.36.
21.Güzeloğlu E. Causes of Nutritional Anemia in Adolescent Children. Online Turkish Journal of Health Sciences (OTSBD). 2020;5(1):25-32. doi: 10.26453/otjhs.515125.
Notas de autor
dr.erenguzeloglu@gmail.com
Información adicional
redalyc-journal-id: 6920
