Case Report
Epilepsy secondary to intracranial calcification cause by hypothyroidism and chronic hypocalcaemia: a case report
Epilepsia secundaria a calcificación intracraneal causada por hipotiroidismo e hipocalcemia crónica: reporte de un caso


Epilepsy secondary to intracranial calcification cause by hypothyroidism and chronic hypocalcaemia: a case report
Iberoamerican Journal of Medicine, vol. 8, núm. 1, pp. 27-31, 2026
Hospital San Pedro
Recepción: 17 Octubre 2025
Corregido: 11 Febrero 2026
Aprobación: 17 Febrero 2026
Abstract: Intracranial calcification is a rare complication of endocrine disorders, such as hypothyroidism. We present a case of a 37-year-old woman who had recurrent generalized tonic-clonic seizures since the age of 19 that were unresponsive to antiepileptic medications. Upon examination, cerebellar ataxia was observed. A brain CT scan and laboratory investigations conducted in April 2023 revealed extensive bilateral symmetric cerebral and cerebellar calcifications, hypothyroidism, hypocalcemia, hypophosphatemia, vitamin D deficiency, and normal levels of parathyroid hormone and kidney, and liver function tests. Antithyroid peroxidase antibodies were negative. The patient's brain calcifications, epilepsy, and ataxia were attributed to chronic hypocalcemia secondary to hypothyroidism and vitamin D deficiency. Treatment included levothyroxine, calcium, vitamin D supplements, and antiepileptic drugs (oxcarbazepine and levetiracetam). Over a year of follow-up, significant medical and neurological improvements were noted, with normalization of thyroid function tests and well-controlled seizures on medication. In conclusion, extensive intracranial calcification and recurrent seizures are uncommon complications of hypothyroidism, likely due to chronic hypocalcemia and hypovitaminosis D. Management involved long-term therapy with levothyroxine, calcium, vitamin D supplements, and antiepileptic drugs.
Keywords: Epilepsy, Hypothyroidism , Hypocalcemia, Hypovitaminosis D, Brain calcification .
Resumen: La calcificación intracraneal es una complicación poco frecuente de trastornos endocrinos, como el hipotiroidismo. Presentamos el caso de una mujer de 37 años que presentó convulsiones tónico-clónicas generalizadas recurrentes desde los 19 años, que no respondieron a la medicación antiepiléptica. En la exploración, se observó ataxia cerebelosa. Una tomografía computarizada cerebral y estudios de laboratorio realizados en abril de 2023 revelaron extensas calcificaciones cerebrales y cerebelosas simétricas bilaterales, hipotiroidismo, hipocalcemia, hipofosfatemia, deficiencia de vitamina D y niveles normales de hormona paratiroidea y pruebas de función renal y hepática. Los anticuerpos antiperoxidasa tiroidea fueron negativos. Las calcificaciones cerebrales, la epilepsia y la ataxia de la paciente se atribuyeron a hipocalcemia crónica secundaria al hipotiroidismo y a la deficiencia de vitamina D. El tratamiento incluyó levotiroxina, calcio, suplementos de vitamina D y fármacos antiepilépticos (oxcarbazepina y levetiracetam). Tras un año de seguimiento, se observaron mejoras médicas y neurológicas significativas, con normalización de las pruebas de función tiroidea y convulsiones bien controladas con medicación. En conclusión, la calcificación intracraneal extensa y las convulsiones recurrentes son complicaciones poco frecuentes del hipotiroidismo, probablemente debidas a la hipocalcemia crónica y la hipovitaminosis D. El tratamiento incluyó terapia a largo plazo con levotiroxina, calcio, suplementos de vitamina D y antiepilépticos.
Palabras clave: Epilepsia , Hipotiroidismo , Hipocalcemia, Hipovitaminosis D, Calcificaciones cerebrales .
INTRODUCTION
Hypothyroidism is a common endocrine disorder, with an estimated prevalence rate of 0.2%-5.7% [1]. However, it is believed that up to 5% of hypothyroidism cases remain undiagnosed, ranging from subclinical to overt [1]. The condition is linked to various risks, including genetic, environmental, and autoimmune factors. The primary global causes of hypothyroidism are iodine deficiency and Hashimoto's thyroiditis [2]. Symptoms of adult-onset hypothyroidism include fatigue, cold intolerance, periorbital puffiness, dry skin, decreased sweating, and myalgia, constipation, thickening of the skin, hypocalcemia, hypophosphatemia, and hypovitaminosis D [2].
Hypothyroidism and its complications are rare contributors to intracranial calcification [3]. Studies have shown that extensive intracranial calcification is a rare condition, with an estimated prevalence of one in 1,000,000 [4]. The differential diagnosis of this condition is traditionally divided into primary (Fahr's disease) and secondary (Fahr's syndrome) intracranial calcification [5, 6, 7, 8]. Fahr's Disease, also known as primary familial brain calcification, is a rare genetic neurodegenerative disorder inherited in an autosomal dominant manner and often associated with mutations in the SLC20A2 and XPR1 genes. The SLC20A2 gene produces the sodium-dependent phosphate transporter 2 (PiT-2) protein, which regulates brain phosphate levels. The XPR1 gene (Xenotropic and Polytropic Retrovirus Receptor 1) encodes a critical transmembrane protein that exports inorganic phosphate from cells, maintaining phosphate balance [4, 5, 6]. Fahr's syndrome results from abnormal calcium deposition in the brain, typically caused by underlying metabolic issues such as endocrine disorders like hypoparathyroidism, pseudohypoparathyroidism, hypothyroidism, and hypovitaminosis D [4, 5, 7, 8]. Central nervous system infections like HIV, toxoplasmosis, rubella, cytomegalovirus, neurocysticercosis, and tuberculosis, as well as toxic exposure like lead poisoning, radiotherapy, and chemotherapy, can also contribute to the condition. Additionally, vascular diseases, mitochondrial disorders, and inflammatory processes may lead to secondary calcification [4, 5, 6]. Both Fahr’s disease and syndrome present with similar CT scan results, showing bilateral calcification of the basal ganglia, thalamus, and dentate nucleus, leading to symptoms such as seizures, headache, movement disorders, cognitive impairment, dementia, and psychiatric disorders (such as psychosis) [9]. Correcting treatable underlying causes of Fahr’s syndrome is essential to improve the patient's condition and prevent disease progression.
In this report, we present a rare case of long-standing refractory epilepsy, ultimately attributed to intracranial calcifications secondary to chronic hypocalcemia caused by untreated hypothyroidism and vitamin D deficiency.
CASE REPORT
A 37-year-old right-handed woman presented with a history of frequent generalized tonic-clonic seizures (≥10 attacks/month) starting at age 19. She had a normal birth and development, reached menarche at 11, and experienced normal menstrual cycles until age 24, after which she developed amenorrhea. She had no history of head trauma or infections. She had no memory or behavioral issues and was independent in daily activities. There was no family history of epilepsy. However, she reported sensitivity to cold, hair loss, constipation, and muscle cramps since her twenties. She received short-term vitamin D, calcium, and levothyroxine therapy for deficiencies but was not on regular medication. She reported compliance on different combination of antiepileptic medications. However, her seizures were uncontrolled despite antiepileptic treatment. Her interictal electroencephalogram (EEG) showed generalized spike-and-wave discharges. In the 6 months before presentation, she was treated with carbamazepine (CBZ) (400 mg twice daily) and sodium valproate (VPA) (500 mg twice daily).
During the physical examination, her vital signs were stable, with a heart rate of 75 beats per minute. She measured 152 cm in height, weighed 55 kg, and had a body mass index (BMI) of 23.8 kg/m2, indicating a normal weight. She had multiple facial and body bruises from falls during uncontrolled seizures. Her skin was dry, but there were no signs of goiter or myxedema. Cardiovascular, respiratory, and abdominal examinations revealed no abnormalities. Neurological examination showed bilateral cerebellar signs, including end-gaze nystagmus, dysarthria, dysmetria, and dysnergia of the upper limbs. She was unable to walk in tandem. A brain computed tomography (CT) scan conducted in April 2023 revealed bilateral symmetrical brain calcifications in the frontal and parietal lobes, basal ganglia, thalami, periventricular white matter, and cerebellar hemispheres (Figure 1).
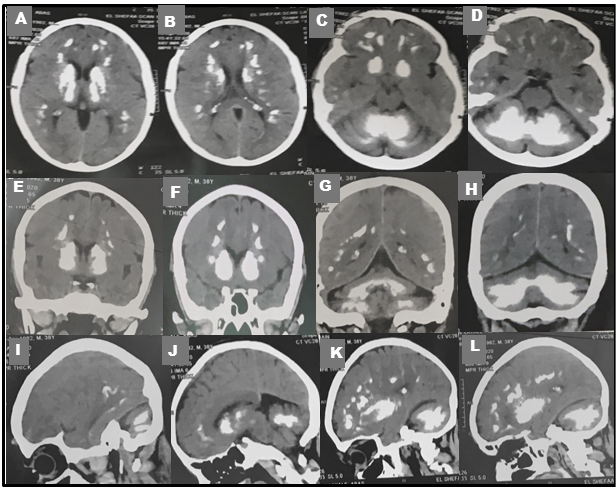
Figure 1
CT scan images from April 2023 revealing widespread bilateral hyperdense lesions (Calcifications) in the frontal and parietal lobes, periventricular white matter, basal ganglia, thalami, and cerebellar hemispheres. The calcifications are visible in axial (A-D), coronal (E-H) and sagittal (I-L) views, with no signs of mass effects.
Comprehensive laboratory testing showed low serum levels of calcium (5.0 mg/dl (normal: 8.6-12.2 mg/dl)), phosphate (0.70 mmol/L (normal: 0.87-1.5 mmol/L)), and vitamin D (25(OH)D) (8 ng/ml (normal: 20–50 ng/ml)). Normal serum parathyroid hormone (PTH) level (1.84 pmol/L (normal: 1.6-6.9 pmol/L)), elevated thyroid stimulating hormone (TSH) level (>150 µIU/ml (normal: 0.27-5.5 µIU/ml)), and decreased levels of free thyroxine (FT4) (0.56 ng/dl (normal: 0.8-1.8 ng/dl)) and triiodothyronine (FT3) (1.09 pg/ml (normal: 1.95-4.8 pg/ml)) were also observed. It indicates hypothyroidism, hypocalcemia, and hypovitaminosis D. The anti-thyroid peroxidase (anti-TPO) antibody test was negative. The patient was diagnosed with symptomatic epilepsy due to intracranial calcification, which was linked to chronic hypocalcemia from hypothyroidism and vitamin D deficiency.
Treatment involved initiating levothyroxine at 50 µg/day, adjusting based on follow-up TSH levels, calcium supplementation (Osteocare tablets twice daily, each containing calcium 1,000 mg, magnesium 100 mg, vitamin D 3,200 I.U., and zinc 5 mg), vitamin D supplementation with cholecalciferol 200,000 I.U using a loading protocol for severe deficiency (intramuscular injections every 10 days for 3 months followed by a maintenance dose of 5000 I.U. twice daily), iron supplement, and switching from CBZ and VPA to oxcarbazepine (OXC) (600 mg twice daily) and levetiracetam (LEV) (500 mg twice daily). Within the first two months, clinical and laboratory improvements were noted, with increased calcium levels (8.6 mg/dL) and decreased TSH levels from >150 µIU/ml to 30 µIU/ml. Follow-up after a year showed sustained improvement, normalization of TSH level (3.2 µIU/ml), and seizure control with the new antiepileptic medications.
DISCUSSION
The patient's epilepsy cause was identified 18 years after the onset of seizures through a CT brain scan, which showed bilateral brain calcification. The symmetric cerebral calcification led to generalized tonic-clonic (GTC) seizures, while ataxia was due to cerebellar calcification. Further investigation revealed hypothyroidism, hypocalcemia, and vitamin D deficiency that had been previously underdiagnosed and undertreated. Ataxia was detected during a neurological examination. With normal parathyroid hormone (PTH) levels, no family history of similar conditions and after ruling out common causes of extensive brain calcification, chronic hypocalcemia associated with hypothyroidism and vitamin D deficiency was identified as the underlying cause of the intracranial calcifications. Hypophosphatemia is often linked with hypocalcemia.
The cause of hypothyroidism in this patient is still unknown. While iodine deficiency and Hashimoto's thyroiditis are common causes of hypothyroidism worldwide [2], the absence of thyroid peroxidase antibodies makes Hashimoto's thyroiditis less likely in this case. Moreover, the fact that the patient's relatives and neighbors living in the same area do not have hypothyroidism makes iodine deficiency an unlikely cause. The patient's hypocalcemia is caused by a combination of hypothyroidism and vitamin D deficiency. Thyroid hormones play a crucial role in regulating calcium and phosphorous levels in the body to maintain balance. They also affect tissue phosphate metabolism and renal phosphate handling, leading to changes in phosphate levels [8]. Research has shown a connection between the thyroid gland and vitamin D, with thyroid hormones activating vitamin D in the kidneys [9]. Studies indicate that hypovitaminosis D is prevalent in individuals with hypothyroidism, with up to 98% of patients affected. The severity of hypothyroidism is also linked to vitamin D deficiency [10]. This association may be due to the shared evolutionary origin of the vitamin D3 receptor and the thyroid hormone receptor from a single gene, resulting in similarities between these receptors [11]. Vitamin D is essential for regulating calcium and phosphorus levels in the blood and increasing their serum concentrations [12].
The precise mechanisms of brain calcification in the presence of chronic hypocalcemia are not fully understood. It can result from various factors, such as an imbalance in the calcium/phosphorus ratio and molecular processes that result in decreased bone turnover, heightened calcium mobilization, decreased absorption of calcium in the intestines, and increased excretion of calcium [7, 8, 9, 10, 11, 12, 13].
The patient's therapy goals include maintaining normal thyroid function, serum calcium, phosphate, and vitamin D levels. The treatment plan consists of: (a) long-term hormone replacement with levothyroxine starting at 50 µg daily, with adjustments based on TSH levels; (b) oral calcium intake ranging from 1-4 grams per day; (c) calcitriol supplementation at 5000 I.U. twice daily; and (d) the use of antiepileptic drugs that have minimal impact on thyroid function (e.g., OXC and LEV) [14]. A follow-up after a year revealed significant improvement in the patient's medical and neurological conditions. Research indicates that regular vitamin D supplementation for a minimum of 3 months can lead to reduced TSH levels and anti-thyroid antibodies in patients with primary hypothyroidism [15].
In conclusion, the reported case demonstrates a clinically significant link between hypothyroidism, chronic hypocalcemia, hypovitaminosis D, intracranial calcifications, and epilepsy. The underdiagnosis of adult-onset hypothyroidism and vitamin D deficiency can result in chronic hypocalcemia, leading to intracranial calcifications. This highlights the importance of investigating metabolic and endocrine factors in patients with refractory epilepsy and intracranial calcifications. Treatment involves long-term adherence to optimal therapy with levothyroxine, as well as calcium and vitamin D supplements, in addition to antiepileptic drugs.
CONFLICT OF INTERESTS
The authors have no conflict of interest to declare. The authors declared that this study has received no financial support.
REFERENCES
1.Garmendia Madariaga A, Santos Palacios S, Guillén-Grima F, Galofré JC. The incidence and prevalence of thyroid dysfunction in Europe: a meta-analysis. J Clin Endocrinol Metab. 2014;99(3):923-31. doi: 10.1210/jc.2013-2409.
2.Almandoz JP, Gharib H. Hypothyroidism: etiology, diagnosis, and management. Med Clin North Am. 2012;96(2):203-21. doi: 10.1016/j.mcna.2012.01.005.
3.Lee JE, Hsieh ST, Lin SK, Wang KC. Extensive bilateral striocerebellar calcifications associated with Hashimoto’s Hypothyroidism. Tzu Chi Med J. 2011;23(1):23-5. doi: 10.1016/j.tcmj.2011.01.010.
4.Saleem S, Aslam HM, Anwar M, Anwar S, Saleem M, Saleem A, et al. Fahr's syndrome: literature review of current evidence. Orphanet J Rare Dis. 2013;8:156. doi: 10.1186/1750-1172-8-156.
5.Perugula ML, Lippmann S. Fahr's Disease or Fahr's Syndrome? Innov Clin Neurosci. 2016;13(7-8):45-6.
6.Golüke NMS, Meijer E, van Maren EA, de Jonghe A, Emmelot-Vonk MH, van Valen E, et al. Amount and Distribution of Intracranial Calcification in Symptomatic and Asymptomatic Primary Familial Brain Calcification. Neurol Clin Pract. 2023;13(4):e200163. doi: 10.1212/CPJ.0000000000200163.
7.Sava A, Dumitrescu G, Haba D, Hodorog D, Mihailov C, Şapte E. The Fahr syndrome and the chronic lymphocytic thyroiditis. Rom J Morphol Embryol. 2013;54(1):195-200.
8.Kavitha MM, Chandrashekharyya SH. Alteration in levels of serum calcium, phosphorous and magnesium in patients of hypothyroidism. Int J Biol Med Res. 2014;5(4):4594-6.
9.Le Hir A, Hak JF, Gragueb-Chatti I, Bobot M. Hypocalcemia-induced seizure with Fahr's syndrome. J Nephrol. 2022;35(3):1047-8. doi: 10.1007/s40620-022-01260-w.
10.Mirhosseini N, Brunel L, Muscogiuri G, Kimball S. Physiological serum 25-hydroxyvitamin D concentrations are associated with improved thyroid function-observations from a community-based program. Endocrine. 2017;58(3):563-73. doi: 10.1007/s12020-017-1450-y.
11.McDonnell DP, Pike JW, O'Malley BW. The vitamin D receptor: a primitive steroid receptor related to thyroid hormone receptor. J Steroid Biochem. 1988;30(1-6):41-6. doi: 10.1016/0022-4731(88)90074-x.
12.Srichawla BS, Andrade E, Kipkorir V. Decoding brain calcifications: A single-center descriptive case series and examination of pathophysiological mechanisms. SAGE Open Med Case Rep. 2023;11:2050313X231197521. doi: 10.1177/2050313X231197521.
13.Hossein-nezhad A, Holick MF. Vitamin D for health: a global perspective. Mayo Clin Proc. 2013;88(7):720-55. doi: 10.1016/j.mayocp.2013.05.011.
14.Hamed SA. The effect of antiepileptic drugs on thyroid hormonal function: causes and implications. Expert Rev Clin Pharmacol. 2015;8(6):741-50. doi: 10.1586/17512433.2015.1091302.
15.Chaudhary S, Dutta D, Kumar M, Saha S, Mondal SA, Kumar A, et al. Vitamin D supplementation reduces thyroid peroxidase antibody levels in patients with autoimmune thyroid disease: An open-labeled randomized controlled trial. Indian J Endocrinol Metab. 2016;20(3):391-8. doi: 10.4103/2230-8210.179997.
Notas de autor
hamedsherifa@aun.edu.eg
Información adicional
redalyc-journal-id: 6920