Original article
Association between possible eating disorders and clinical factors in middle-aged Afro-descendant women
Asociación entre posible trastorno de la conducta alimentaria y factores clínicos en mujeres afrodescendientes de mediana edad

 Virginia Romero-Gutiérrez
Angélica Monterrosa-Blanco
Virginia Romero-Gutiérrez
Angélica Monterrosa-Blanco
Association between possible eating disorders and clinical factors in middle-aged Afro-descendant women
Iberoamerican Journal of Medicine, vol. 8, núm. 1, pp. 3-12, 2026
Hospital San Pedro
Recepción: 23 Julio 2025
Corregido: 16 Octubre 2025
Aprobación: 13 Noviembre 2025
Abstract:
Introduction: Eating disorders (EDs) are a group of entities that are characterized by a persistent alteration in behavior in the face of basic food needs, which cause alterations in the absorption of food and damages to physical health or psychosocial functioning. Although the DSM criteria are used for the diagnosis of EDs, screening with simple tools, such as the SCOFF scale, is recommended to identify people at risk and implement the necessary preventive measures. The objective was to determine the frequency of possible EDs and to establish their association with various clinical factors.
Material and methods: A cross-sectional study belonging to the research project Quality of life in menopause and Colombian ethnicities [CAVIMEC]. It was performed in women self-identified as Afro-descendants, with skin phototype V-VI and aged between 40-59 years. The SCOFF questionnaire was applied, a five-item tool that allows establishing the existence of possible EDs. Bivariate and adjusted logistic regression was performed, considering possible EDs as a dependent variable, clinical factors as independent variables, and as covariates: age, coffee consumption, and smoking.
Results: 420 women were studied, 22.8% postmenopausal and possible EDs in 130 (30.9%) of the participants. The following were associated with eating disorders: mood alterations with menstruation OR: 4.92 [95%CI: 2.60-9.32], more than one severe depressive episode OR: 4.81 [95%CI: 1.19-19.3], consultation with psychology OR: 4.11 [95%CI: 2.09-8.12], consultation with psychiatry OR: 3.73 [95%CI: 1.05-13.21], increased metabolic risk OR: 3.53 [95%CI: 2.09-5.95], abdominal hysterectomy: 3.19 [95%CI: 1.45-7.00], excessive sadness after childbirth OR: 3.15 [95%CI: 1.11-8.86], abdominal obesity OR: 3.14 [95%CI: 1.54-6.39], diabetes mellitus OR: 2.99 [95% CI: 1.56-5.72], obesity OR: 2.33 [95%CI: 1.26-3.94], postmenopause OR: 2.05 [95%CI: 1.25-3.37].
Conclusions: In a group of Afro-descendant women in middle age, it was found that one third had possible EDs. Several clinical factors were significantly associated with an increased chance of EDs.
Keywords: Feeding and eating disorders , Black people , Women, Psychiatry, Middle aged , Mental disorders .
Resumen:
Introducción: Los trastornos de la conducta alimentaria (TCA) son un grupo de entidades que se caracterizan por una alteración persistente en el comportamiento ante las necesidades básicas alimentarias, lo que provoca alteración en la absorción de los alimentos y perjuicios en la salud física o el funcionamiento psicosocial. Si bien, para el diagnóstico de los TCA se utilizan los criterios del DSM, se recomienda el tamizaje con herramientas sencillas, como la escala SCOFF, para identificar a las personas en riesgo e implementar las medidas preventivas necesarias. El objetivo fue determinar la frecuencia de posible TCA y establecer su asociación con diversos factores clínicos.
Material y métodos: Estudio transversal perteneciente al proyecto de investigación Calidad de vida en la menopausia y las etnias colombianas [CAVIMEC]. Se realizó en mujeres auto reconocidas como afrodescendientes, con fototipo cutáneo V-VI y con edad entre 40-59 años. Se aplicó el cuestionario SCOFF, herramienta de cinco ítems que permite establecer la existencia de posible TCA. Se realizó regresión logística bivariada y ajustada, considerando posible TCA como variable dependiente, los factores clínicos como variables independientes y como covariables: la edad, el consumo de café y el hábito de fumar.
Resultados: Se estudiaron 420 mujeres. 22,8% posmenopáusica y posibles TCA en 130 (30,9%) de las participantes. Se asociaron a TCA: alteraciones del estado de ánimo con la menstruación OR: 4,92 [IC95%: 2,60-9,32], más de un episodio depresivo severo OR: 4,81 [IC95%: 1,19-19,3], consulta con psicología OR: 4,11 [IC95%: 2,09-8,12], consulta con psiquiatría OR: 3,73 [IC95%: 1,05-13,21], aumento del riesgo metabólico OR: 3,53 [IC95%: 2,09-5,95], histerectomía abdominal 3,19 [IC95%: 1,45-7,00], tristeza excesiva después del parto OR: 3,15 [IC95%: 1,11-8,86], obesidad abdominal OR: 3,14 [IC95%: 1,54-6,39], diabetes mellitus OR: 2,99 [IC95%: 1,56-5,72], obesidad OR: 2,33 [IC95%: 1,26-3,94], postmenopausia OR: 2,05 [IC95%: 1,25-3,37].
Conclusiones: En un grupo de mujeres afrodescendientes en la edad media de la vida, se encontró que un tercio presentaba posible TCA. Varios factores clínicos se asociaron significativamente con una mayor posibilidad de TCA.
Palabras clave: Trastornos de alimentación y de la ingestión de alimentos , Población negra, Mujer, Psiquiatría , Mediana edad, Trastornos mentales .
INTRODUCTION
Eating disorders (EDs) are characterized by a persistent alteration in eating or eating-related behavior, which causes a disturbance in food absorption and significantly impairs physical health or psychosocial functioning [1, 2]. Globally, around 55.5 million people are affected by eating disorders, and the rate seems to be increasing [3]. The DSM-V-TR classifies EDs as Anorexia Nervosa, Bulimia Nervosa, Binge Eating Disorder, Pica, Rumination Disorder, and Avoidant/Restrictive Food Intake Disorder, which may have in common excessive preoccupation with weight, body shape, food, and the use of unhealthy nutritional measures [1]. EDs tend to impair physical, psychological, and social functioning, they are diagnosed using DSM criteria and have been reported to affect 1.6% of the general female population [1, 4, 5, 6] Screening for Eds are recommended to identify individuals at risk and implement necessary preventive measures. The SCOFF scale is one such assessment tool, confirming that it is not a diagnostic test [3, 7, 8].
EDs are three to four times more common in women than in men [2, 5]. The National Survey of American Life found that men are 65% less likely to develop any Eds [9]. It has also been pointed out that eating disorders are common in adolescents and youth, with a notable increase observed in recent years among middle-aged women and older adults [8]. The latter are more likely to have binge eating disorders than other EDs and tend to have even more serious complications [10, 11]. Malnutrition, electrolyte imbalance, muscle weakness, gastroesophageal reflux, irritable bowel syndrome, loss of bone mineral density, thyroid dysfunction, and cardiac arrhythmias, among others, can be complications of Eds [7, 12]. Few studies worldwide address EDs considering the transition to menopause and postmenopause. At the same time, there are few evaluations of Eds among women belonging to groups that are ancestrally discriminated against and violated, such as Afro-descendants women, who have their own social, nutritional and cultural patterns [9]. It seems that there are no studies on EDs in women in the climacteric stage of life who reside in Latin America. The objective of the study was to determine the frequency of possible EDs and to establish their association with clinical factors in middle-aged Afro-descendant women living in the Colombian Caribbean region.
MATERIAL AND METHODS
DESIGN AND ETHICAL CONSIDERATIONS
The University of Cartagena (Colombia) ethics committee, according to Act 117-2019, approved a cross-sectional study part of the research project Quality of Life in Menopause and Colombian Ethnicities (CAVIMEC). Participation was anonymous and voluntary, with participants receiving information about the research and signing informed consent. The study considered Helsinki's Declaration, the Belmont Report, and the Scientific, Technical, and Administrative Standards for Health Research, Resolution 8430-1993 of Colombia's Ministry of Health. The suggestions, recommendations, and checklist of the STROBE initiative were considered when structuring the research report.
PARTICIPANTS
Women aged between 40-59 years, daughters of a Black father and mother, with the phenotype of the same ethnicity, skin phototype V or VI, self-recognition as Afro-descendant, and compliant with routine activities. These women were contacted in community settings through visits to their homes, never in waiting rooms of health centers or in medical consultations. All of them are face-to-face pollsters. They received invitations from previously trained surveyors who visited urban and rural municipalities in the Colombian Caribbean region, considered to be the settlement of African ancestors' communities brought as enslaved people in colonial times. Pregnant women, those who had given birth for less than five years, those with mental, visual, reading, and writing disabilities, and those who had received or were receiving any medical or surgical intervention to modify body weight were excluded. At their convenience, no visits were made to closed settlements, protected communities, special districts, or reservations.
TOOLS
Participants filled out a printed form containing three sections. The first part had questions about age, main activity, the sexual partner, coffee or smoking habit, and prior consultation with psychology or psychiatry. In addition, other questions were asked to find out their perception or opinion about "a history of excessive sadness after childbirth", "mood swings with menstruation" and "more than one major depressive episode". A history of abdominal hysterectomy, bilateral oophorectomy, treatment for high blood pressure or diabetes mellitus was questioned. Menstrual cycles were also asked about menopausal status. In the second section, some measurements were recorded: weight (kg) with a digital scale, height (cm) with a wall height meter, abdominal circumference (cm) and hip circumference (cm) with tape at the umbilical scar and the upper border of the iliac crests, respectively. The surveyor carried out all measurements with the participants standing barefoot and lightly dressed. The third section of the form included the five questions of the SCOFF [Sick-Control-One stone-Fat-Food] questionnaire. A short, simple, robust EDs detection instrument that was published in 1999 and administered in health, educational, and community institutions. Each item of the SCOFF questionnaire is answered "Yes" or "No"; one point is assigned to the affirmative answers. Two or more points on the SCOFF questionnaire suggest a possible case of Eds [3, 13, 14, 15, 16]. In a study conducted in Brazilian adult male and female populations, the SCOFF questionnaire had a sensitivity of 80%, a specificity of 71%, an accuracy of 72.3%, a positive predictive value of 23.1%, a negative predictive value of 97.1%, a positive likelihood ratio of 2.81, and a negative likelihood ratio of 0.28 [15]. The SCOFF scale has been validated in different countries, ethnic groups, and age groups. In Colombia, the SCOFF scale has been used and validated in adolescents and in university communities, it is considered useful as a rapid screening tool with the caveat that its reliability and consistency are oscillating. SCOFF allows initial screening for possible EDs and does not establish a diagnosis of altered eating behavior. It is recommended that immediately after a positive test, it is considered complementing it with other more robust instruments, including the recommendations provided by the DSM-V-TR [1]. The cut-off point used for the SCOFF scale is based on what has been indicated in previous studies [3, 13, 14, 15, 16].
DEFINITIONS
According to the menstrual situation at the time of the survey, the following were established: menopause transition (with menstrual bleeding or amenorrhea for less than twelve months) and post menopause (with twelve or more months of amenorrhea). Diabetes mellitus or arterial hypertension was considered if these entities had been previously diagnosed, received medication and were under clinical follow-up. The other four metabolic factors were defined as follows. With the body mass index, the nutritional status was determined according to WHO criteria: underweight (≤18.49 kg/m2), normal (18.50-24.99 kg/m2), overweight (25.00-29.99 kg/m2), and obesity (≥30.00 kg/m2) [17]. Abdominal obesity was considered when the measurement of the circumference of the abdomen was >88 cm, following recommendations from the WHO. Metabolic risk increased significantly, also called cardiometabolic risk, was established when the circumference of the abdomen was >80cm, as established by the WHO in a technical document released in 2008 and endorsed by the International Diabetes Federation [IFD]. Finally, android obesity was identified with the waist-to-hip ratio >0.85, also established by the WHO.
SAMPLE SIZE
The program for epidemiological and statistical analysis (EPIDAT-3.1) estimated a sample of 384 women, defining a confidence level of 95%, expected proportion of 50%, significance of 5%, and absolute precision of 5%. The 2019 projection of the 2005 Colombian population census by the National Department of Statistics (DANE) was used for sample size assumptions. It estimated that 73.0% and 27.0% of the total population resided in urban and rural areas, respectively, and that women between 40-59 years of age were 4,347,590. In addition, 10.6% identified themselves as Afro-descendants and 32.0% were settled in the Caribbean region. Therefore, 592,514 were considered Colombian women aged 40-59 years who self-identified as Afro-descendants, and 189,605 resided in the Caribbean region. The latter is the universe of study. An additional twenty percent over the sample size was added to replace partially completed forms and another 10% to replace the lost ones. 506 forms were available and applied daily, according to the population size of the Colombian Caribbean's geographical departments and considering the population's urban/rural distribution.
STATISTICAL ANALYSIS
Conducted with Epi-Info-7 (Centers for Disease Control and Prevention, Atlanta, USA). The information was tabulated into a Microsoft Excel 2007© database. Participants were divided into two groups according to the overall score of the SCOFF questionnaire: women with possible EDs and without possible EDs. Continuous data were expressed in means and standard deviation, and categorical data in absolute and percentage values. Statistical differences between continuous data were estimated with the Mann-Whitney/Wilcoxon test (due to heterogeneity of variance between groups, which was calculated with the Bartlett test). Statistical differences in the percentage data were established with Chi2. Unadjusted logistic regression was calculated; possible EDs were the dependent variable, and the independent ones were sociodemographic and clinical characteristics established in the study. An adjusted logistic regression model was performed, with the same dependent variable and for each independent variables that were statistically significant in the bivariate analysis, adjusting for age, coffee consumption and smoking habit. For each of these models, the likelihood ratio was estimated, and to identify the presence of multicollinearity, the Variance Inflation Factor (FIV) was calculated. For all analyses, a p value <0.05 was considered statistically significant.
RESULTS
Five hundred-six forms were applied, and 86 (16.9%) were discarded because of incomplete completion. The study included 420 women, exceeding the sample size by 9.4%. Participants' average age was 50.1 years; 22.8% were in post menopause, 82.8% had abdominal obesity, and 65.7% had significantly increased metabolic risk. Possible EDs were identified in 130 (30.9%) of those who had greater abdominal and hip circumference than those without possible EDs (p<0.001). In addition, among women with possible EDs, a higher frequency of mood swings with menstruation, a history of abdominal hysterectomy, prior consultations to psychology, abdominal obesity, increased metabolic risk, and diabetes mellitus, were observed (p<0.001) (Table 1).
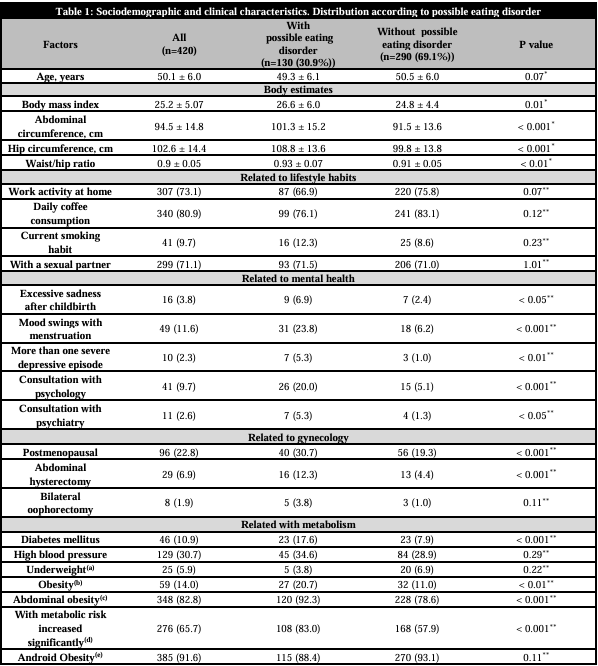
Data are presented in means and standard deviation or in absolute values (percentages). p value calculated with (*)MannWhitney/Wilcoxon or (**)Chi2.
(a) Body Mass Index between 25.0-29.9 kg/m2 [WHO]. (b) Body Mass Index >30 kg/m2 [WHO]. (c) Abdominal circumference ≥88 cm [WHO]. (d)Abdominal circumference ≥80 cm [WHO] and [International Diabetes Federation]. (e)Waist/hip ratio ≥0.85 [WHO].Of the participants, 24 (5.7%) answered affirmatively all the questions of the SCOFF questionnaire while 238 (56.6%) answered all negatively. The most frequently reported manifestation in relation to EDs was feeling sick when a full stomach felt uncomfortable (Figure 1).
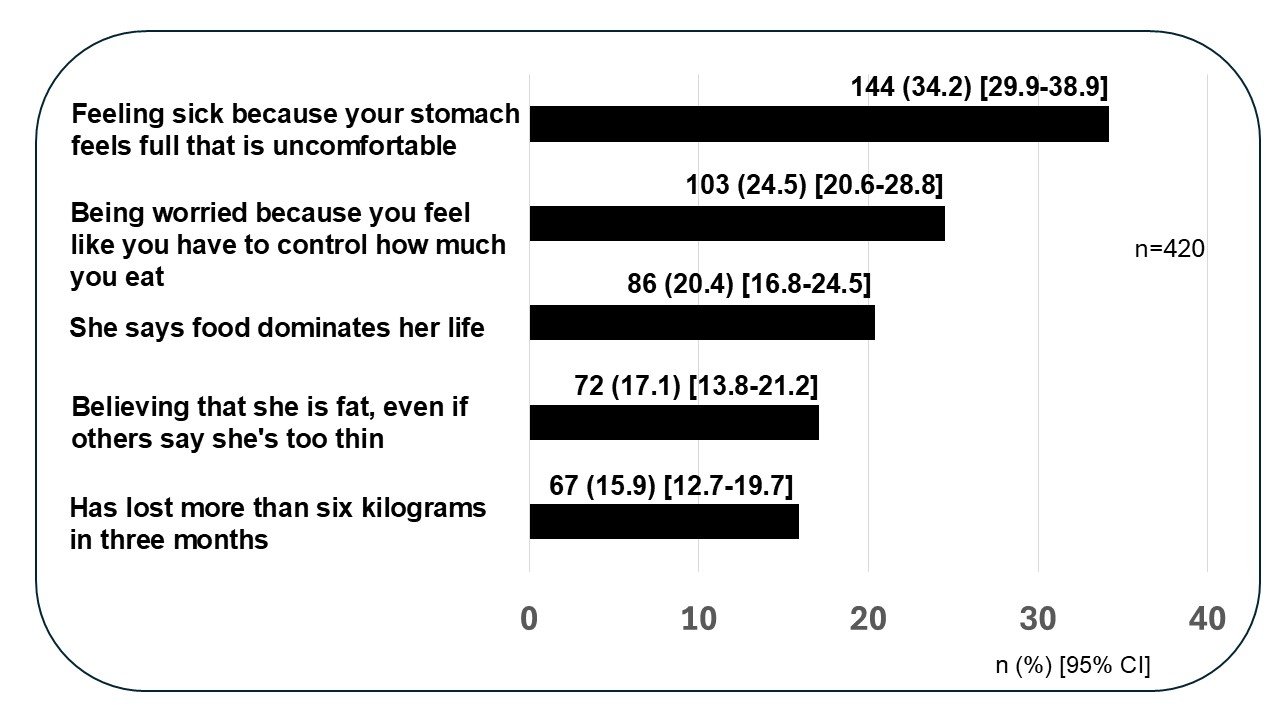
Figure 1
Manifestations related to eating disorders (Eds). SCOFF Scale.
Among the participants, 24 (5.7%) answered affirmatively all the questions on the SCOFF questionnaire, while 238 (56.6%) answered all negatively. Mood swings with menstruation, more than one severe depressive episode, consultation with psychology, consultation with psychiatry, having a significantly increased metabolic risk, abdominal hysterectomy, excessive sadness after childbirth, abdominal obesity, Type II diabetes, obesity, and post menopause were significantly associated with possible EDs in the bivariate analysis and adjusted models (Table 2).
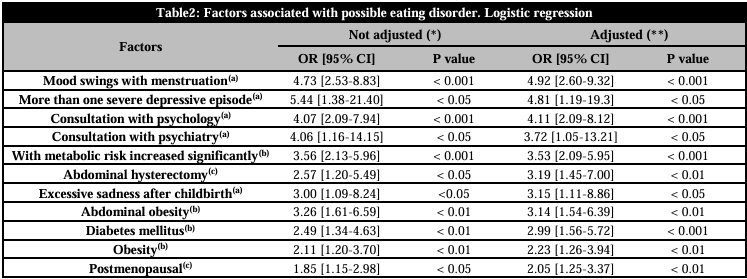
(*) Not associated with eating disorders: age, work activity, sexual partner, daily coffee consumption, smoking, bilateral oophorectomy, high blood pressure and android obesity (p>0.05). (**) Each variable was adjusted for age, smoking and daily coffee consumption. (Likelihood Ratio <0.05) (Variance Inflation Factor (FIV) <10). (a)Related to mental health. (b)Related with metabolism. (c)Related to gynecology
DISCUSSION
In a group of women between 40-59 years of age living in Colombia, we found that 30.9% had possible EDs when assessed with the SCOFF questionnaire. A similar frequency has been described in other population groups on the same scale. In a French cohort of fifty-four patients affected by endometriosis, aged between 18-50 years, 35.2% had possible Eds [18]. Texeira et al. [15] found possible EDs in 33.5% of adults of both sexes aged 18-32 years. Bazzazian et al. [14] found possible EDs in 29% of Iranians aged between 17-49 years, of whom 67.4% were women. We could not identify another study specifically in climacteric women that assessed EDs with the SCOFF questionnaire. There appears to be no differences in the frequency of eating disorders according to ethnic characteristics. Marques et al. [19] did not find them when evaluating anorexia nervosa, bulimia nervosa, or binge eating disorders. However, the frequency of binge eating was higher in African Americans than in whites, but the latter had been more likely to have received mental health services than the former. Similarly, in another assessment, the rate of bulimia and binge eating in African American adults was like that found in whites [9].
Among the women studied, it was found that post menopause was associated with twice the possibility of EDs. By study design, this relationship is statistical and not causal. Several authors point out that estrogenic decrease, an essential characteristic of post menopause, may contribute to an increased risk of Eds [20, 21, 22, 23]. Lower estradiol levels are associated with higher food intake and binge eating episodes in humans and animals [23, 24]. In ovariectomized adult rats, increased food intake and frequency of binge eating states have been reported, which are usually reversed with the administration of estradiol [25]. In women, low estradiol levels predict binge-eating episodes [26]. As with menopausal symptoms, there seems to be individual susceptibility to the influence that ovarian hormones would have on Eds [20]. Mangweth-Matzek et al. [27] and Khalil et al. [28] agree that menopause favors the most significant risk of generating overt expressions or subclinical pictures of de Novo EDs or promoting the disorder relapsed in those in remission. A woman’s psychosocial and genetic identity may not be as important for developing EDs as gonadal function and ovarian hormones [2].
We have found in the present study that a history of mood swings with menstruation, excessive sadness after childbirth, and more than one severe depressive episode were associated with a higher possibility of EDs. Several authors have made similar notes and pointed out that ovarian hormones are involved [2, 29, 30, 31, 32, 33]. The decrease in estrogen and progesterone at the beginning of menstruation and after childbirth affects the bioavailability of neurotransmitters such as serotonin, norepinephrine, and gamma-aminobutyric acid [GABA], causing emotional lability that makes many women more sensitive to environmental demands [2]. Changes in mood, tolerance, patience, irritability, sadness, easy crying, anxiety, depression, ability to control or cope before menstruation are called premenstrual syndrome, and if severe, they are recognized as premenstrual dysphoric disorder. Çoban et al. [31] and Hardin et al. [32] have noted that women with premenstrual syndrome are more prone to EDs than women without premenstrual syndrome. In this regard, Finch et al. [29] suggest that the relation between EDs and premenstrual symptoms is evident, and the mechanisms are shared; both overeating, intense cravings and negative emotional states connect EDs with premenstrual dysphoric disorder. A study of Japanese women found that those with EDs had greater severity of premenstrual symptoms, both physical and psychological, compared to others without Eds [34]. It has also been pointed out that EDs represent a greater risk for postpartum depressive symptomatology, a condition of high emotional vulnerability for some women. In this regard, Makino et al. [35] noted the relationship between EDs recurrence and postpartum depression, while Easter et al. [30] indicated that women with active or remission EDs had higher depression scores during pregnancy and postpartum compared to women without a history of EDs. A systematic review identified that depression is one of the most prevalent psychiatric comorbidities in patients with EDs, especially with anorexia nervosa and bulimia [36]. The simultaneous presence of EDs and major depression leads to greater functional deterioration, poorer adherence to any treatment, and a higher rate of relapse of both conditions [37]. A meta-analysis suggests that the relationship between EDs and depression is bidirectional, i.e., depressive symptoms can be both a cause and a consequence of Eds [38].
In this study, we identified that having a history of consultation with psychology and psychiatry was associated with four- and three-times possible EDs, respectively. This is consistent with other studies that associate anxiety, depression, low self-esteem, inability to cope with emotions, identity problems, and poor coping skills with EDs. Information from the National Institute of Mental Health indicates that in adults, EDs are related to other central disorders such as anxiety, difficulties with mood, impulse control, and substance use disorders [4].
We also found that women with Type II diabetes had a higher possibility of EDs, OR: 2.99 [95%CI: 1.56-5.72], which is in line with what was indicated by Nieto-Martínez et al. [39] who also found an increased risk of EDs with Type II diabetes mellitus, OR: 3.7 [95%CI: 1.1-12.1]. Similar data were found in a meta-analysis on the relationship between Type I diabetes and EDs, bulimia, and binge eating, RR: 2.47 [95% CI: 1.84-3.32], RR: 2.80 [95% CI: 1.18-6.65], and RR: 1.53 [95% CI: 1.18-1.98], respectively [40]. The relationship between diabetes and EDs seems independent of the screening or diagnostic tools used. In turn, we identified in this study that having a very high metabolic risk, abdominal obesity, and obesity were related to a higher possibility of EDs. Several authors have pointed out that EDs are related to metabolic alterations, obesity, dyslipidemia, heart disease, deterioration of quality of life in terms of health, and increased health costs [1, 6, 41, 42]. The effect of EDs on the components of metabolic syndrome has been demonstrated [41, 43]. For example, in a seven-year follow-up cohort of obese/overweight young adults, 23% reported having EDs, which were associated with hyperlipidemia and higher body mass index [43]. Caroleo et al. [44] reported that cytokines and growth factors play a role in the interaction between obesity and EDs, suggesting a potential immune component in the metabolic implications of EDs. The relationship between obesity and EDs, in addition to being a factor that negatively affects diabetes treatment, has a strong association with various mental disorders, for example, binge eating disorders [1].
In this study in Colombian women, a relationship was found between possible EDs with abdominal hysterectomy but not with bilateral oophorectomy. EDs are associated with many multi-system medical complications, some of which are life-threatening. Therefore, early identification and intervention are necessary. In addition, EDs are related to or fostered by sociocultural postures or events: family dysfunction, intimate partner violence, sexual abuse, victimization by appearance-related teasing, controlling relationships, dissatisfaction with body shape, beauty patterns, stereotypes of femininity, and even anti-aging demands, for example [33, 45]. Comprehensive care for patients with EDs must be guaranteed, with a multidisciplinary approach that includes physicians, psychologists, nutritionists, and other specialists according to the needs of each case, including primary care [7, 12].
STRENGTHS, LIMITATIONS AND RECOMMENDATIONS
The strength of this study is that it is one of the first to highlight the problem of eating disorders among women in the climacteric stage of life. The intention is to raise awareness among professionals who care for women in the climacteric stage about the importance of questioning EDs. It is also a strength to have used the SCOFF questionnaire, a short, easy-to-apply and interpretable, relevant, valid, widely used tool, translated into several languages and recognized as a strategy for screening or detecting EDs [3, 13, 14, 15, 16]. It is a strength to have surveyed the participants in their housing units and within the conceptualization of primary or community care. It avoids the exclusion bias due to the reduced opportunity for care that some Afro-descendant groups tend to have. At the same time, there are limitations inherent in cross-sectional studies, which allow for establishing statistical associations and not causal relationships. Although the sample size was estimated using the Colombian population census data projected for the year of application of the questionnaires and stratification according to geographical areas, extrapolations to other ethnic groups, including Afro-descendants, should be done with caution due to the different sociocultural, nutritional, environmental, genetic influences and the individual perception of body image. Some data may be over- or under-dimensioned because selection or perception biases could not be controlled entirely. It should be considered that recall bias might be present in self-reported variables, as well as the possibility of multicollinearity in logistic regression models, despite the tests applied. Finally, and it may also be a limitation to use a rapid detection test such as SCOFF and not a structured or semi-structured diagnostic tool, which could not be applied by the professionals who performed the community visits.
We recommend that healthcare policies advise routine screening for possible EDs in climacteric women with the SCOFF questionnaire, which has important advantages [3, 13, 14, 15, 16] However, other tools can also be used: Eating Disorder Examination Questionnaire [EDE-Q], Clinical Impairment Assessment Questionnaire [CIA], Eating Attitudes Test (EAT), Bulimic Investigatory Test Edinburgh (BITE), Disordered Eating Attitude Scale (DEAS) [8, 16]. The need to identify EDs is supported by the fact that up to 15.3% of middle-aged women live with the probability of presenting expressions of these diseases at some point in their lives, which offer a greater risk for various disabling physical and emotional morbidities, as well as mortality at an early age [6, 12, 33]. Although this study's results should be taken as initial and are strictly for detection and not diagnosis, it is suggested that professionals who take care of menopausal women's health at the primary or specialized care levels be interested in implementing programs or actions that seek to promote prevention. Early identification, diagnosis, timely treatment and follow-up of EDs, to preserve the good health conditions, the adequate perception of well-being and the sufficient quality of life in the middle-aged women. Health professionals who perform primary care and community care may consider the SCOFF scale for screening for EDs because of its brevity, ease of application, and simplicity of interpretation. In the event of scores suggestive of possible EDs, they should make a timely referral to specialized health authorities where diagnostic tools will be used.
CONCLUSIONS
In a group of Afro-descendant women from the Colombian Caribbean, in the climacteric stage and surveyed in their housing units, it was found that a third had possible EDs when the SCOFF questionnaire was applied. The clinical factors that were related to a higher possibility of eating disorders were having a history of mood swings with menstruation, excessive sadness after childbirth, more than one severe depressive episode, consulting psychology, consulting psychiatry, abdominal hysterectomy, diabetes mellitus, having a significantly increased metabolic risk, abdominal obesity, obesity and being in post menopause. More research is needed in other ethnic communities and under different cultural influences, to better establish the interrelationship between EDs and various biological, psychological, social, and environmental factors in middle-aged women. In addition, it is necessary to explore how poverty, margination, violence, and discrimination are contributors to possible Eds.
ACKNOWLEDGMENTS
Thank you to all the women who accepted and were able to participate in the study. Thanks to the general practitioners Geraldine Romero Martínez, Veronica Daza Daza, Camila Castro Barraza, Angie Rosales Becerra, and Maria Angélica Gómez, who participated in the fieldwork phase of the study, and Mrs. Mabel Vergara Borja and Judith Ramos Vásquez, who supervised and coordinated the necessary planning.
CONFLICT OF INTERESTS
The authors have no conflict of interest to declare. The authors declared that this study has received no financial support.
REFERENCES
1.American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition. Text Revision. Washington, DC: American Psychiatric Association: 2022.
2.Young JK. Ovarian hormones and eating disorders. Front Psychol. 2024;15:1467795. doi: 10.3389/fpsyg.2024.1467795.
3.Coop A, Clark A, Morgan J, Reid F, Lacey JH. The use and misuse of the SCOFF screening measure over two decades: a systematic literature review. Eat Weight Disord. 2024;29(1):29. doi: 10.1007/s40519-024-01656-6.
4.Treasure J, Duarte TA, Schmidt U. Eating disorders. Lancet. 2020;395(10227):899-911. doi: 10.1016/S0140-6736(20)30059-3.
5.Qian J, Wu Y, Liu F, Zhu Y, Jin H, Zhang H, et al. An update on the prevalence of eating disorders in the general population: a systematic review and meta-analysis. Eat Weight Disord. 2022;27(2):415-28. doi: 10.1007/s40519-021-01162-z.
6.Tith RM, Paradis G, Potter BJ, Low N, Healy-Profitós J, et al. Association of Bulimia Nervosa With Long-term Risk of Cardiovascular Disease and Mortality Among Women. JAMA Psychiatry. 2020;77(1):44-51. doi: 10.1001/jamapsychiatry.2019.2914.
7.Voss MM. Eating Disorders & the Primary Care Physician. Mo Med. 2022;119(3):243-9.
8.Thompson KA, Bardone-Cone AM. Disordered eating behaviors and attitudes and their correlates among a community sample of older women. Eat Behav. 2019;34:101301. doi: 10.1016/j.eatbeh.2019.05.004.
9.Taylor JY, Caldwell CH, Baser RE, Faison N, Jackson JS. Prevalence of eating disorders among Blacks in the National Survey of American Life. Int J Eat Disord. 2007;40 Suppl(Suppl):S10-4. doi: 10.1002/eat.20451.
10.Mangweth-Matzek B, Hoek HW, Pope HG Jr. Pathological eating and body dissatisfaction in middle-aged and older women. Curr Opin Psychiatry. 2014;27(6):431-5. doi: 10.1097/YCO.0000000000000102.
11.Westmoreland P, Krantz MJ, Mehler PS. Medical Complications of Anorexia Nervosa and Bulimia. Am J Med. 2016;129(1):30-7. doi: 10.1016/j.amjmed.2015.06.031.
12.Podfigurna-Stopa A, Czyzyk A, Katulski K, Smolarczyk R, Grymowicz M, Maciejewska-Jeske M, et al. Eating disorders in older women. Maturitas. 2015;82(2):146-52. doi: 10.1016/j.maturitas.2015.06.036.
13.Morgan JF, Reid F, Lacey JH. The SCOFF questionnaire: assessment of a new screening tool for eating disorders. BMJ. 1999;319(7223):1467-8. doi: 10.1136/bmj.319.7223.1467.
14.Bazzazian S, Ozgoli G, Kariman N, Nasiri M, Mokhtaryan-Gilani T, Hajiesmaello M. The translation and psychometric assessment of the SCOFF eating disorder screening questionnaire: the Persian version. J Eat Disord. 2022;10(1):38. doi: 10.1186/s40337-022-00564-3.
15.Teixeira AA, Roque MA, de Freitas AA, Dos Santos NF, Garcia FM, Khoury JM, et al. The Brazilian version of the SCOFF questionnaire to screen eating disorders in young adults: cultural adaptation and validation study in a university population. Braz J Psychiatry. 2021;43(6):613-6. doi: 10.1590/1516-4446-2020-1667.
16.Moser CM, Terra L, Behenck ADS, Brunstein MG, Hauck S. Cross-cultural adaptation and translation into Brazilian Portuguese of the instruments Sick Control One Stone Fat Food Questionnaire (SCOFF), Eating Disorder Examination Questionnaire (EDE-Q) and Clinical Impairment Assessment Questionnaire (CIA). Trends Psychiatry Psychother. 2020;42(3):267-71. doi: 10.1590/2237-6089-2019-0083.
17.Chooi YC, Ding C, Magkos F. The epidemiology of obesity. Metabolism. 2019;92:6-10. doi: 10.1016/j.metabol.2018.09.005.
18.Aupetit A, Grigioni S, Roman H, Coëffier M, Bréant A, Hennetier C, et al. Association between Endometriosis, Irritable Bowel Syndrome and Eating Disorders: ENDONUT Pilot Study. J Clin Med. 2022;11(19):5773. doi: 10.3390/jcm11195773.
19.Marques L, Alegria M, Becker AE, Chen CN, Fang A, Chosak A, et al. Comparative prevalence, correlates of impairment, and service utilization for eating disorders across US ethnic groups: Implications for reducing ethnic disparities in health care access for eating disorders. Int J Eat Disord. 2011;44(5):412-20. doi: 10.1002/eat.20787.
20.Anaya C, Culbert KM, Klump KL. Binge Eating Risk During Midlife and the Menopausal Transition: Sensitivity to Ovarian Hormones as Potential Mechanisms of Risk. Curr Psychiatry Rep. 2023;25(2):45-52. doi: 10.1007/s11920-022-01405-5.
21.Mikhail ME, Anaya C, Culbert KM, Sisk CL, Johnson A, Klump KL. Gonadal Hormone Influences on Sex Differences in Binge Eating Across Development. Curr Psychiatry Rep. 2021;23(11):74. doi: 10.1007/s11920-021-01287-z.
22.Culbert KM, Sisk CL, Klump KL. A Narrative Review of Sex Differences in Eating Disorders: Is There a Biological Basis? Clin Ther. 2021;43(1):95-111. doi: 10.1016/j.clinthera.2020.12.003.
23.Klump KL, Culbert KM, Sisk CL. Sex Differences in Binge Eating: Gonadal Hormone Effects Across Development. Annu Rev Clin Psychol. 2017;13:183-207. doi: 10.1146/annurev-clinpsy-032816-045309.
24.Foright RM, Johnson GC, Kahn D, Charleston CA, Presby DM, Bouchet CA, Wellberg EA., et al. Compensatory eating behaviors in male and female rats in response to exercise training. Am J Physiol Regul Integr Comp Physiol. 2020;319(2):R171-R183. doi: 10.1152/ajpregu.00259.2019.
25.Micioni Di Bonaventura MV, Lutz TA, Romano A, Pucci M, Geary N, Asarian L, Cifani C. Estrogenic suppression of binge-like eating elicited by cyclic food restriction and frustrative-nonreward stress in female rats. Int J Eat Disord. 2017;50(6):624-635. doi: 10.1002/eat.22687.
26.Klump KL, Racine SE, Hildebrandt B, Burt SA, Neale M, Sisk CL, Boker S, Keel PK. Ovarian Hormone Influences on Dysregulated Eating: A Comparison of Associations in Women with versus without Binge Episodes. Clin Psychol Sci. 2014;2(4):545-59. doi: 10.1177/2167702614521794.
27.Mangweth-Matzek B, Hoek HW, Rupp CI, Kemmler G, Pope HG Jr, Kinzl J. The menopausal transition--a possible window of vulnerability for eating pathology. Int J Eat Disord. 2013;46(6):609-16. doi: 10.1002/eat.22157.
28.Khalil J, Boutros S, Kheir N, Kassem M, Salameh P, Sacre H, et al. Eating disorders and their relationship with menopausal phases among a sample of middle-aged Lebanese women. BMC Womens Health. 2022;22(1):153. doi: 10.1186/s12905-022-01738-6.
29.Finch JE, Xu Z, Baker JH. Understanding comorbidity between eating disorder and premenstrual symptoms using a network analysis approach. Appetite. 2023;181:106410. doi: 10.1016/j.appet.2022.106410.
30.Easter A, Solmi F, Bye A, Taborelli E, Corfield F, Schmidt U, Treasure J, Micali N. Antenatal and postnatal psychopathology among women with current and past eating disorders: longitudinal patterns. Eur Eat Disord Rev. 2015;23(1):19-27. doi: 10.1002/erv.2328.
31.Çoban ÖG, Karakaya D, Önder A, İşleyen Z, Adanır AS. Association of Premenstrual Dysphoric Disorder and Eating Behaviors Among Nursing Students: A Cross-Sectional Study. J Pediatr Adolesc Gynecol. 2021;34(2):203-208. doi: 10.1016/j.jpag.2020.11.019.
32.Hardin SL, Thornton LM, Munn-Chernoff MA, Baker JH. Premenstrual symptoms as a marker of ovarian hormone sensitivity in eating disorders. Int J Eat Disord. 2020;53(2):296-301. doi: 10.1002/eat.23213.
33.Hambleton A, Pepin G, Le A, Maloney D; National Eating Disorder Research Consortium; Touyz S, Maguire S. Psychiatric and medical comorbidities of eating disorders: findings from a rapid review of the literature. J Eat Disord. 2022;10(1):132. doi: 10.1186/s40337-022-00654-2.
34.Yoshinari Y, Morino S, Shinohara Y, Chen CY, Onishi M, Akase Y, et al. Association between premenstrual syndrome and eating disturbance in college students: a cross-sectional study. BMC Womens Health. 2024;24(1):330. doi: 10.1186/s12905-024-03158-0.
35.Makino M, Yasushi M, Tsutsui S. The risk of eating disorder relapse during pregnancy and after delivery and postpartum depression among women recovered from eating disorders. BMC Pregnancy Childbirth. 2020;20(1):323. doi: 10.1186/s12884-020-03006-7.
36.Solmi M, Radua J, Olivola M, Croce E, Soardo L, Salazar de Pablo G, et al. Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol Psychiatry. 2022;27(1):281-95. doi: 10.1038/s41380-021-01161-7.
37.Gianini LM, White MA, Masheb RM. Eating pathology, emotion regulation, and emotional overeating in obese adults with Binge Eating Disorder. Eat Behav. 2013;14(3):309-13. doi: 10.1016/j.eatbeh.2013.05.008.
38.Kenny B, Fuller-Tyszkiewicz M, Moodie M, Brown V, Williams J. Bi-directional associations between depressive symptoms and eating disorder symptoms in early adolescence. Body Image. 2022;42:246-56. doi: 10.1016/j.bodyim.2022.06.012.
39.Nieto-Martínez R, González-Rivas JP, Medina-Inojosa JR, Florez H. Are Eating Disorders Risk Factors for Type 2 Diabetes? A Systematic Review and Meta-analysis. Curr Diab Rep. 2017;17(12):138. doi: 10.1007/s11892-017-0949-1.
40.Dean YE, Motawea KR, Aslam M, Pintado JJL, Popoola-Samuel HAO, Salam M, et al. Association Between Type 1 Diabetes Mellitus and Eating Disorders: A Systematic Review and Meta-Analysis. Endocrinol Diabetes Metab. 2024;7(3):e473. doi: 10.1002/edm2.473.
41.Chevinsky JD, Wadden TA, Chao AM. Binge Eating Disorder in Patients with Type 2 Diabetes: Diagnostic and Management Challenges. Diabetes Metab Syndr Obes. 2020;13:1117-31. doi: 10.2147/DMSO.S213379.
42.Olguin P, Fuentes M, Gabler G, Guerdjikova AI, Keck PE Jr, McElroy SL. Medical comorbidity of binge eating disorder. Eat Weight Disord. 2017;22(1):13-26. doi: 10.1007/s40519-016-0313-5.
43.Nagata JM, Garber AK, Tabler J, Murray SB, Vittinghoff E, Bibbins-Domingo K. Disordered eating behaviors and cardiometabolic risk among young adults with overweight or obesity. Int J Eat Disord. 2018;51(8):931-41. doi: 10.1002/eat.22927.
44.Caroleo M, Carbone EA, Greco M, Corigliano DM, Arcidiacono B, Fazia G, et al. Brain-Behavior-Immune Interaction: Serum Cytokines and Growth Factors in Patients with Eating Disorders at Extremes of the Body Mass Index (BMI) Spectrum. Nutrients. 2019;11(9):1995. doi: 10.3390/nu11091995.
45.Solmi M, Radua J, Stubbs B, Ricca V, Moretti D, Busatta D, et al. Risk factors for eating disorders: an umbrella review of published meta-analyses. Braz J Psychiatry. 2021;43(3):314-23. doi: 10.1590/1516-4446-2020-1099.
Notas de autor
alvaromonterrosa@gmail.com
Información adicional
redalyc-journal-id: 6920