ABSTRACT
Objective: to verify the factors associated with the practice of skin-to-skin contact with breastfeeding in the first hour of life and its influence on exclusive breastfeeding in the first month.
Method: a retrospective cross-sectional study with medical records from a breastfeeding outpatient clinic in São Paulo, Brazil. The sample included all the medical records of the mother-baby dyad who had been consulted by nurses between 2004 and 2010. Data were collected from the medical records between 2014 and 2015.
Results: 1,030 medical records were identified, 71 were excluded and the final sample was 959. The prevalence of skin-to-skin contact with breastfeeding in the first hour was 37.2%. The Apgar score between 8 and 10 in the first minute of life and the higher birth weight of the newborn were protective factors of contact with early breastfeeding; lower maternal age and cesarean delivery and forceps were risk factors for this practice. Exclusive breastfeeding was statistically higher in the group of newborns who had contact with breastfeeding in the first hour; however, there was no association with duration of exclusive breastfeeding.
Conclusion: good birth conditions were protective factors for breastfeeding followed by skin-to-skin contact in the first hour, while younger maternal age and surgical deliveries proved to be risk factors. Exclusive breastfeeding in the baby´s first month of life was not associated with skin-to-skin contact followed by breastfeeding in the first hour of life.
DESCRIPTORS: Breastfeeding, Postpartum period, Newborn, Childbirth Health promotion, Obstetric nursing.
RESUMO
Objetivo: verificar os fatores associados à prática do contato pele a pele com amamentação na primeira hora de vida e sua influência no aleitamento materno exclusivo no primeiro mês.
Método: estudo transversal, retrospectivo, com prontuários de um ambulatório especializado em aleitamento materno em São Paulo, Brasil. Fizeram parte da amostra todos os prontuários das duplas mãe-filho que passaram em consulta com enfermeiras entre os anos de 2004 e 2010. A coleta de dados nos prontuários ocorreu entre 2014 e 2015.
Resultados: identificaram-se 1.030 prontuários, 71 foram excluídos e a amostra final foi de 959. A prevalência do contato pele a pele com amamentação na primeira hora foi de 37,2%. A nota do Apgar entre 8 e 10 no 1º minuto de vida e o maior peso ao nascimento do recém-nascido foram fatores protetores do contato com a amamentação precoce; já a menor idade materna e os partos cesárea e fórceps foram fatores de risco para esta prática. O aleitamento materno exclusivo foi estatisticamente maior no grupo dos recém-nascidos que realizaram o contato com a amamentação na primeira hora, no entanto, não houve associação com o tempo de aleitamento materno exclusivo.
Conclusão: as boas condições de nascimento da criança foram fatores protetores para a realização do contato pele a pele com amamentação na primeira hora, enquanto a menor idade materna e os partos cirúrgicos demonstraram-se como fatores de risco. O aleitamento materno exclusivo no primeiro mês de vida da criança não esteve associado ao contato e amamentação precoce.
DESCRITORES: Aleitamento materno, Período pós-parto, Recém-nascido, Parto, Promoção da saúde, Enfermagem obstétrica.
RESUMEN
Objetivo: verificar los factores asociados con la práctica del contacto piel con piel con la lactancia materna en la primera hora de vida y su influencia en la lactancia materna exclusiva en el primer mes.
Método: estudio transversal retrospectivo con registros médicos de un servicio de lactancia en São Paulo, Brasil. La muestra incluyó todos los registros médicos de las parejas madre-hijo que consultaron con enfermeras entre 2004 y 2010. Los datos se recopilaron de los registros entre 2014 y 2015.
Resultados: han detectado 1.030 registros médicos, se excluyeron 71 y la muestra final fue 959. La prevalencia del contacto piel a piel con la lactancia materna en la primera hora fue del 37,2%. El puntaje de Apgar entre 8 y 10 en el primer minuto de vida y el mayor peso al nacer del recién nacido fueron factores protectores del contacto con la lactancia materna precoce; La menor edad materna, el parto fórceps y la cesária fueron factores de riesgo para esta práctica. La lactancia materna exclusiva fue estadísticamente mayor en el grupo de recién nacidos que tuvieron contacto piel con piel y amamantar en la lactancia materna en la primera hora; sin embargo, no hubo asociación con la duración de la lactancia materna exclusiva.
Conclusión: las buenas condiciones de nacimiento del bebe fueron factores protectores contacto piel con piel con la lactancia materna en la primera hora, mientras que la edad materna más joven y los partos por cesárea y fórceps resultaron ser factores de riesgo. La lactancia materna exclusiva en el primer mes de vida no se asoció con el contacto y la lactancia materna precoz.
DESCRIPTORES: Lactancia, Período posparto, Recién nacido, Parto Promoción de la salud, Enfermería obstétrica.
Carátula del artículo
SKIN-TO-SKIN CONTACT FOLLOWED BY BREASTFEEDING IN THE FIRST HOUR OF LIFE: ASSOCIATED FACTORS AND INFLUENCES ON EXCLUSIVE BREASTFEEDING
CONTATO PELE A PELE E MAMADA PRECOCE: FATORES ASSOCIADOS E INFLUÊNCIA NO ALEITAMENTO MATERNO EXCLUSIVO
CONTACTO CON LA PIEL Y LA MAMA PRECOZ: FACTORES ASOCIADOS E INFLUENCIA EN LA LACTANCIA MATERNA EXCLUSIVA
 Márcia Carneiro Saco ma_boaro@yahoo.com.br
Márcia Carneiro Saco ma_boaro@yahoo.com.br
Centro Universitário São Judas Tadeu, Brasil
Kelly Pereira Coca
Universidade Federal de São Paulo, Brasil
Karla Oliveira Marcacine
Universidade Federal de São Paulo, Brasil
Érika de Sá Vieira Abuchaim
Universidade Federal de São Paulo, Brasil
Ana Cristina Freitas de Vilhena Abrão
Universidade Federal de São Paulo, Brasil
Texto & Contexto - Enfermagem, vol. 28, e20180260, 2019
Universidade Federal de Santa Catarina, Programa de Pós Graduação em Enfermagem
Received: 17 July 2018
Accepted: 08 March 2019
INTRODUCTION
Early skin-to-skin contact (SSC) and breastfeeding in the first hour of life have been widespread practices in the humanization of care for women in childbirth, with the aim of promoting the quality of care in the delivery room and breastfeeding. It is a recommendation set out in the fourth step of the “Ten Steps to Successful Breastfeeding” promoted by the World Health Organization (WHO) and the United Nations (UNICEF) since the creation of the Baby Friendly Hospital Initiative (BFH).1
The practice of SSC is currently defined as the baby placed belly-down (naked) directly on the mother´s chest within the first five minutes of birth and continued for at least one hour.1 Step four also involves supporting mothers to breastfeed in the first hour of life: encouraging the mother to identify if the baby is showing signs of wanting to breastfeed, and offering help if needed.1
Among the benefits of SSC, studies have shown a greater likelihood of breastfeeding immediately after delivery,2 favoring newborn skin colonization from the mother, better neonate blood glucose control, 3 body temperature control, cardiovascular dynamics stabilization, lower body weight loss and maternal satisfaction.4 In addition to SSC, breastfeeding in the first hour of life also reflects a number of advantages such as decreased risk of postpartum hemorrhage,5 lower risk of infections, and neonatal death.6
Despite the benefits, Brazilian studies showed low prevalence of early skin-to-skin contact and breastfeeding in the first hour of life, as observed in a maternity hospital in São Paulo, where only 7% (n = 118/1787) of babies born in a Baby Friendly Hospital had early contact in the first 30 minutes of life and 24% (n = 431/1787) had between 30 and 60 minutes;7 while in a maternity hospital located in Rio de Janeiro maternity, 16% of women practiced SSC.8 In 2015, the national prevalence of breastfeeding in the first hour of life was 43 %, while global data ranged from 42% in Latin America and Asia and 49% in Central and Eastern Europe.9 In the latest national survey conducted in 2008, an increase in the practice of breastfeeding in the first hour of life was identified to 67.7%, showing increasing rates over the years.10
SSC and breastfeeding in the first hour of life are recommended by WHO1 because of their impact on the protection of neonatal death and the numerous benefits that breastfeeding offers for both mother and baby.6
One study that examined breastfeeding in the first hour life, showed that breastfeeding was negatively associated with maternal complications during pregnancy, caesarean section and lack of institutional protocols; however, no associations were found with sociodemographic characteristics of the woman.11
Regarding the duration of breastfeeding, a recent systematic review showed that breastfeeding in the first hour life, appears to increase breastfeeding time in the first four months and contributes to exclusive breastfeeding (EBF), however, these studies had limitations.3
The low rate of this practice has been challenging to overcome and, therefore, it is necessary to understand the factors that protect or prevent this practice, as well as to know other characteristics that may interfere with skin-to-skin contact with breastfeeding in the first hour of life. Therefore, the present study aimed to verify the factors associated with the practice of skin-to-skin contact with breastfeeding in the first hour of life and its influence on exclusive breastfeeding in the first month.
METHOD
A retrospective cross-sectional study conducted at an outpatient breastfeeding clinic in São Paulo, Brazil. The service serves lactating women who wish to breastfeed their children. Most of the population comes from a University Hospital, a large institution linked to the Federal University of São Paulo, which provides support for the practice of breastfeeding in the maternity ward. The obstetric unit of the hospital cares for pregnant women and mostly high-risk parturients, who are hospitalized in rooming-in wards in the postpartum period and receive appointments to be seen in the outpatient clinic on their day of discharge.
The study population consisted of medical records of women and babies attended at the outpatient clinic. The sample included all the medical records of the mother-child dyad who had been consulted with nurses between January 2004 and December 2010, and had a follow-up consultation scheduled for at least the first month of life of the baby. Records referring to women with multiple pregnancies, those which did not use a standard form, recommended by the institution or which did not have complete registration data related to the main objectives of the study were excluded.
Data collection began in December 2014 and was completed in January 2015. A questionnaire developed specifically for this study was used and data entry was performed by two trained obstetric nurses.
The dependent variable was defined as the type of breastfeeding, and as independent: sociodemographic data (age, education, occupation and marital status), and women's obstetric data (parity, previous experience in breastfeeding and type of delivery); and neonatal data (gender of the child, Apgar score at 1 and 5 minutes, SSC with breastfeeding in the first hour of life, birth weight, weight at hospital discharge, type of breastfeeding and pacifier use in the first month of life).
SSC at birth with breastfeeding in the first hour of life was defined as the practice of placing the child on its mother's chest or belly after birth (yes or no) followed by the child suckling on its mother's breast within the first hour after birth.1 The classification of breastfeeding was; exclusive breastfeeding (breast milk only), complementary breastfeeding (breast and artificial milk), predominant breastfeeding (breast milk and water/ water-based drinks) and bottle-feeding (infant formula only).12
Statistical analysis was performed using Minitab 16.1 software. The numerical characterization variables were calculated by mean and standard deviation, while the categorical variables by frequency and percentage. The comparison between the groups with and without SSC/breastfeeding in the first hour of life was performed by Student's t-test or Mann-Whitney test and Chi-square or Fisher's exact test for quantitative and categorical variables, respectively. The logistic regression model was used to estimate the odds ratio (OR) and its 95% confidence interval (CI) to assess the univariate association between SSC/Breastfeeding in the first hour of life and study variables. All variables presented significance of p≤0.20 in the univariate analysis in the initial logistic regression model. The backward process was used, i.e., the non-significant variables were removed from the initial model, one by one, until in the final model only the variables with significance of p <0.05 remained.
The study was approved by the Research Ethics Committee of the Universidade Federal de São Paulo under number 907.103/14 and all ethical principles governing studies involving human beings, established in Resolution No. 466 of December 12, 2012, of the National Health Council were respected, with the following CAAE: 37542414.2.0000.5505. The consent form was waived because it was a study with secondary data.
RESULTS
A total of 1,030 medical records were identified between the study period. Among these, 71 were excluded according to the established criteria. The final sample consisted of 959 records of women and their children. Women had a mean age of 28.6 years (SD 7.1; n = 949 *). Tables 1 and 2 show the other characteristics of women and data of children, respectively, whose records were studied.
Table 1
Sociodemographic and obstetric characteristics of women. São Paulo, SP, Brazil, 2015.
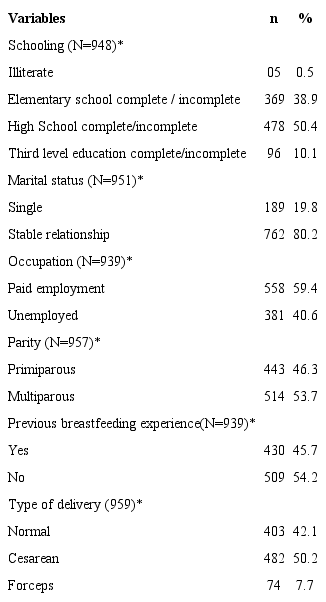 * Sample variation due to data loss.
* Sample variation due to data loss.
The babies had an average birth weight of 3,051 grams (SD = 521; n = 958 *) and hospital discharge weight 2,895.73 grams (SD = 481; n = 939 *).
Table 2
Characteristics of children. São Paulo, SP, Brazil, 2015.
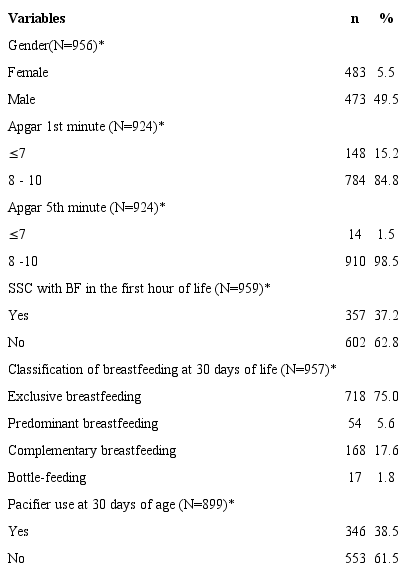 * Sample variation due to data loss; BF =.
* Sample variation due to data loss; BF =.
In the univariate analysis, a significant difference was observed between the groups for the variables related to women: age, type of delivery; and to the child: Apgar at the 1st and 5th minutes of life, birth weight, hospital discharge weight and type of breastfeeding in the 1st month of life. The multivariate analysis in logistic regression identified that the Apgar score between 8 and 10 in the first minute of life and greater birth weight of the newborn were protective factors for SSC with breastfeeding in the first hour of life, whereas younger maternal age and the use of caesarean sections and forceps were shown to be risk factors for this practice (Table 3).
Table 3
Association between skin-to-skin contact and maternal and child variables, São Paulo, SP, Brazil, 2015. (N = 959).
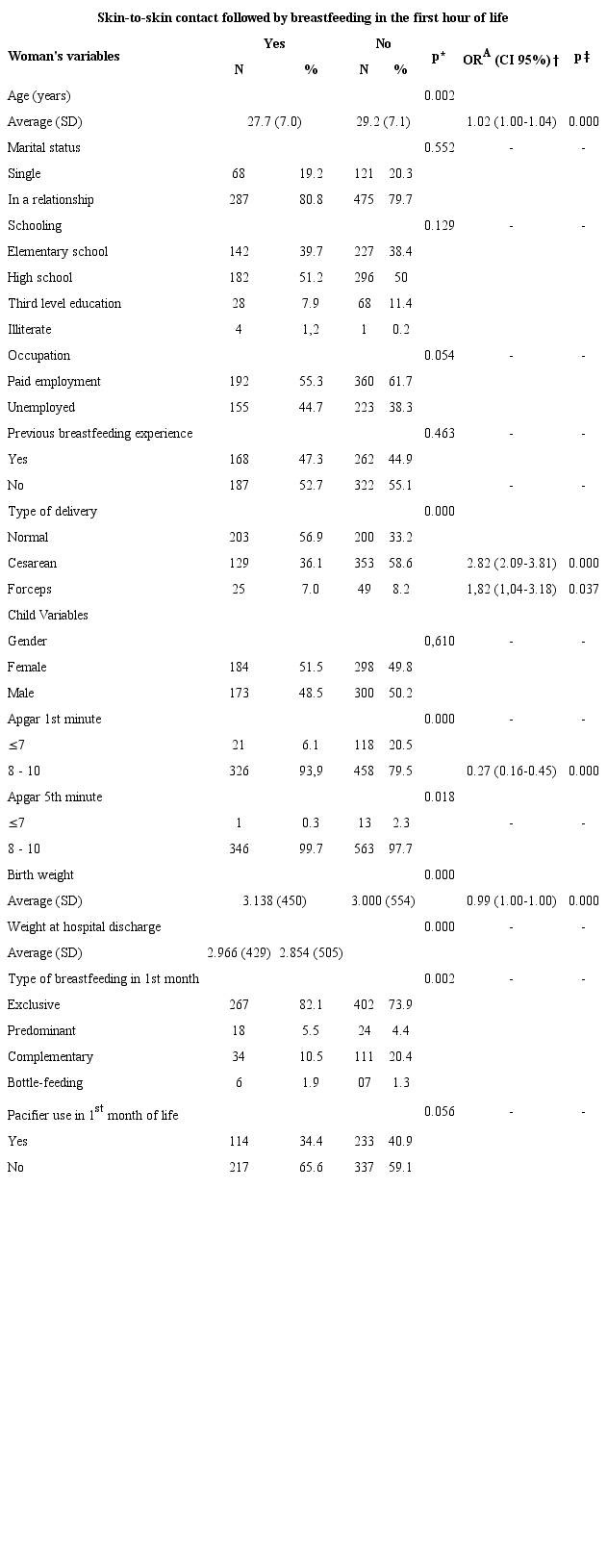 * P value in univariate analysis; †ORA = Odds Ratio, logistic regression adjusted for multivariate analysis; ‡P value in multivariate analysis.
* P value in univariate analysis; †ORA = Odds Ratio, logistic regression adjusted for multivariate analysis; ‡P value in multivariate analysis.
DISCUSSION
The prevalence of SSC followed by breastfeeding in the first hour of life found in this study (37.2%) is below the national average identified in 2008 (67.7%),10 however, it is close to the world average (43%) presented by UNICEF9 and to a recent publication which analyzed the rate of breastfeeding in the first hour of life (31-60%) between 2000 and 2013 in 57 countries.13 The low prevalence may be related to the characteristic of maternity, which serves high-risk women, increasing the occurrence of cesarean section and the conditions relating to the birth of the child.14
Cesarean section and forceps as types of delivery were risk factors for the practice of SSC with breastfeeding in the first hour of life, as well as younger maternal age. Multivariate analysis showed that a woman exposed to cesarean section is almost three times more likely to fail to perform SSC with breastfeeding in the first hour of life when compared to women who had a vaginal birth. This finding is consistent with a systematic review that, in 11 of the 14 studies investigated, identified cesarean delivery as the factor most consistently associated with not breastfeeding in the first hour of life.15 Studies have confirmed this result even in hospitals that adopt practices that promote the use of breastfeeding.16-18 In relation to forceps delivery, there was a higher risk of not performing SSC followed by breastfeeding in the first hour of life, likely due to the presence of analgesia, which may interfere with breastfeeding in the first hour of life.19
The country's high cesarean section rates and childbirth interventions such as the use of oxytocin, early rupture of the amniotic membrane and other unnecessary procedures have been a national concern due to the consequences for women and children.20 Thus, it is important to highlight the need to discuss obstetric care when it comes to encouraging SSC with breastfeeding in the first hour of life.
Regarding maternal age, younger women were associated with not performing SSC with breastfeeding in the first hour of life , a result also confirmed in the literature, where extreme ages were occasionally associated with a higher risk of not breastfeeding, and maternal age under 25 years was identified as a risk factor for not breastfeeding in the first hour of life.15 This finding may be related to greater inexperience and insecurity among these women, despite women having little or no decision-making power about SSC followed by breastfeeding in the first hour of life and depend on the professionals and institutional and clinical routines.18
The lack of knowledge regarding HIV serological status is an obstacle to SSC and breastfeeding in the first hour of life which needs to be faced in Brazil. It is identified as a risk factor for starting breastfeeding which, despite having national norms in place for HIV prevention and control, failures and misconceptions in practice are still present.21 The risk of virus transmission through breastfeeding is well established, and the practice is contraindicated for women with a confirmed diagnosis.22 Nevertheless, the challenge has been to promote breastfeeding in the first hour of life in women who have not been attended prenatally and/or who have not performed tests to prove the negativity of the disease during pregnancy.23 The rapid test is used as a tool for the initial identification of the disease before delivery, but hospital routine may delay diagnosis and interfere with breastfeeding in the first hour of life.21
Regarding protective factors, Apgar score between 8 and 10 in the first minute of life and higher birth weight were related to the practice of SSC with breastfeeding in the first hour of life. The result coincides with those identified in a systematic review, in which immediate complications with the newborn and consequent decline in the Apgar score increase the time interval for breastfeeding in the first hour of life.24
Similarly, the birth weight of children, when adequate, was related to the practice of SSC with breastfeeding in the first hour of life, and 24 and in agreement with these findings, a study conducted in Nigeria25 and Nepal26 also identified a greater weight relationship with the practice of breastfeeding in the first hour of life. Birth weight greater than 2,500 grams is shown to be a protective factor for breastfeeding in the first hour of life.27
It is known that immaturity may limit the skills needed to adapt a child to extrauterine life, which decreases the chance of breastfeeding in the first hour of life15 and increases the need for interventions to ensure the child's stability at birth.28
It is at the moment of birth and in the immediate postpartum that hospital practices can directly interfere with women's expectation of being able to breastfeed.29 Therefore, it is understood that obstetric care has an impact on the viability of SSC and breastfeeding in the first hour of life, as well as the organization of health services that assist women in childbirth, 13 and the need to prepare them for this practice, which is still lacking.30 In this context, it is noteworthy that the performance of nursing professionals deserves to be mentioned because it has constant and direct participation in the care and referral of the mother-child binomial, during and after delivery.30
Regarding the type of breastfeeding practiced, breastfeeding was statistically higher in the group of newborns who underwent SSC with breastfeeding in the first hour of life, when compared to those with children who did not perform this practice. These data corroborate the findings of international studies, which found that SSC with breastfeeding in the first hour of life were positively associated with the success of the first breastfeeding moment, and SSC enabled a shorter time for effective breastfeeding to occur in the first hour of life, improving maternal satisfaction rates.3
Regarding the continuation of exclusive breastfeeding, this type of breastfeeding in the first month of life had no impact with the practice of skin-to-skin contact or breastfeeding in the first hour of life. Contrary to what was identified in this study, research shows that SSC with breastfeeding in the first hour of life were associated with longer duration of EBF in the first month of life3,15and at four months of age.3 The stimulation of breastfeeding in the first hour of life and skin-to-skin contact with the mother favors the establishment of effective suction,31 as a positive consequence for continuity in maternity, and prolongation of EBF.15
The limitation of the study is the loss of some data due to the use of secondary data. On the other hand, the historical analysis of the consultations performed at the specialized breastfeeding service provided more data in less time when prospective studies were performed. The data allowed the identification of other factors associated with SSC with breastfeeding in the first hour of life, besides those found in the literature, which will allow comparisons in future research, as well as benefiting strategies that aim to improve the prevalence of this practice in the service.
Thus, despite the obstacles concerning effective SSC and breastfeeding in the first hour of life, the work of a skilled team which promotes SSC and breastfeeding in the first hour of life immediately after delivery is essential for the successful implementation of Step 4 of the Baby Friendly Hospital Initiative or even for institutions who do not have this title, given its short, medium and long term impact on maternal and child health.
CONCLUSION
The prevalence of SSC followed by breastfeeding in the first hour of life (37.2%) is within the world average. Good birth conditions of the child were protective factors for this practice, while younger maternal age and cesarean section and forceps proved to be risk factors. EBF in the first month of life had no impact on skin-to-skin contact or breastfeeding in the first hour of life.
The preparation of the health team to care for women in the delivery room is essential so that the indication of childbirth interventions and assessments of the child's birth condition are relevant to ensure skin-to-skin contact followed by breastfeeding in the first hour of life and consequently promote EBF.
ACKNOWLEDGMENT
To nurse Barbara Tideman Sartório Camargo, who contributed to the data collection. Study conducted at the Outpatient Breastfeeding Clinic of UNIFESP - Ana Abrão Center - Assistance, Teaching and Research on Breastfeeding and Human Milk Bank, São Paulo, Brazil.
