Caso Clínico
Malignant Pericardial Effusion Secondary to Lung Adenocarcinoma: Case Report
Derrame pericárdico maligno secundario a adenocarcinoma de pulmón: Reporte de caso
Derrame pericárdico maligno secundário ao adenocarcinoma pulmonar: relato de caso
Malignant Pericardial Effusion Secondary to Lung Adenocarcinoma: Case Report
MedUNAB, vol. 20, no. 1, pp. 63-69, 2017
Universidad Autónoma de Bucaramanga

This work is licensed under Creative Commons Attribution 4.0 International.
Received: 19 October 2015
Accepted: 02 February 2017
Resumen: Introducción: El derrame pericárdico maligno es la acumulación de líquido en el espacio pericárdico secundario a neoplasias en estadios avanzados, siendo así, un indicador de mal pronóstico. Los tumores malignos que con mayor frecuencia se relacionan con esta entidad son los de origen pulmonar, mamario y hematolinfoides. Clínicamente puede cursar con signos inminentes de taponamiento cardiaco e inestabilidad hemodinámica, por lo que amerita un diagnóstico temprano y manejo urgente con maniobras de descompresión. Objetivo: Este articulo busca presentar un caso de derrame pericárdico maligno, debido a que esta condición clínica implica un reto diagnóstico. Presentación del caso y conclusiones: Presentamos el caso de un paciente masculino de 63 años de edad, con cuadro clínico de 1 mes de evolución, caracterizado por presencia de adenopatías cervicales, quien en los últimos 15 días presenta saciedad precoz, sudoración nocturna, sensación de distensión abdominal y deterioro de la clase funcional hasta disnea de pequeños esfuerzos, motivo por el cual consulta al servicio de urgencias. Durante la observación médica rápidamente progresa a inestabilidad hemodinámica, refractaria a manejo; se realizan estudios imagenológicos, en donde se evidencia derrame pericárdico severo, por lo que se procede a realizar pericardiocentesis descompresiva emergente y manejo integral multidisciplinario. [Chilatra- Fonseca JM, Morales-Camacho WJ, Plata-Ortiz JE, Gómez- Mancilla YP, Villabona-Rosales SA. Derrame pericárdico maligno secundario a adenocarcinoma de pulmón: Reporte de caso. MedUNAB 2017; 20(1): 63-69].
Palabras clave: Taponamiento Cardíaco, Derrame Pericárdico, Neoplasias Pulmonares, Invasividad Neoplásica, Pericardiocentesis.
Abstract: Introduction: Malignant pericardial effusion is the accumulation of liquid in the pericardial space secondary to advanced stage neoplasia, becoming in an indicator of bad prognosis. Malignant tumors that are most often related to this entity are the ones from pulmonary, mammary, and hematolymphoid origin. Clinically, it may present imminent signs of cardiac tamponade and hemodynamic instability, so that it merits an early diagnosis and management with emerging decompression maneuvers. Objective: This article presents a malignant pericardial effusion case, since this clinical condition implies a diagnostic challenge. Case presentation and Conclusions: A case of a 63 year old male patient is presented. He has one month of clinical evolution characterized by cervical adenopathies, also in the past fifteen days has been presenting precocious satiety, nocturnal sweating, sensation of distended abdomen, and functional class deterioration to having dyspnea during small physical efforts. This was the reason why he went to the emergency room. During the medical observation, the patient quickly deteriorates to hemodynamic instability, refractory to treatment. Some imaging studies were performed, which show severe pericardial effusion so a decompressive pericardiocentesis and a multidisciplinary integral management were performed. [Chilatra-Fonseca JM, Morales-Camacho WJ, Plata-Ortiz JE, Gómez-Mancilla YP, Villabona-Rosales SA. Malignant Pericardial Effusion Secondary to Lung Adenocarcinoma: Case Report. MedUNAB 2017; 20(1): 63-69].
Keywords: Cardiac Tamponade, Pericardial Effusion, Lung Neoplasms, Neoplasm Invasiveness, Pericardiocentesis.
Resumo: Introdução: O derrame pericárdico maligno é o acúmulo de líquido no espaço pericárdico secundário a neoplasias em estádios avançados, sendo, portanto, um indicador de mau prognóstico. Os tumores malignos, frequentemente associados a esta categoría, são aqueles de origem pulmonar, mamária e hematolinfóides. Clinicamente, podem apresentar sinais iminentes de tamponamento cardíaco e instabilidade hemodinâmica, o que justifica um diagnóstico precoce e t ratamento urgente com manejo de descompressão. Objetivo: Este artigo tem como objetivo apresentar um caso de derrame pericárdico maligno, pois esta condição clínica implica um desafio diagnóstico. Apresentação e conclusões do caso: apresentamos o caso de um paciente do sexo masculino de 63 anos, com o quadro clínico de 1 mês de evolução, caracterizado pela presença de linfadenopatia cervical, que nos últimos 15 dias apresenta saciedade precoce, sudação noturna, distensão abdominal e deterioração da classe funcional até a dispnéia de pequenos esforços, motivo pelo qual consulta o serviço de emergência. Durante a observação médica, ele progride rapidamente para a instabilidade hemodinâmica, refratária ao manejo; Estudos de imagem são realizados, nos quais o derrame pericárdico grave é evidente, por isso é necessário realizar pericardiocentese descompressiva emergente e gerenciamento integral multidisciplinar. [Chilatra-Fonseca JM, Morales-Camacho WJ, Plata-Ortiz JE, Gómez-Mancilla YP, Villabona-Rosales SA. Derrame pericárdico maligno secundário ao adenocarcinoma pulmonar: relato de caso. MedUNAB 2017; 20 (1): 63-69].
Palavras-chave: Derrame Pericárdico, Neoplasias Pulmonares, Invasividade Neoplásica, Pericardiocentese, Tamponamento Cardíaco.
Introduction
Pericardial effusion (PE) is defined as the accumulation of fluid in the pericardial space secondary to an injury or inflammation. Its etiology has been associated with various conditions or events, among the most common are the infectious, traumatic, metabolic, autoimmune, neoplastic and induced by radiotherapy and chemotherapy origin (1). Also, depending on the etiology, the type of pericardial fluid may be transudate or exudate (2).
Malignant pericardial effusion (MPE) has a great impact on morbidity and mortality of patients, with a reported prevalence up to 21% associated with an advanced state of neoplastic diseases (3, 4). The primary malignancies of lung, breast and hematolymphoid, are the ones that most often associate with this pathology (5). In autopsies of patients with different types of cancer have been demonstrated a compromise of up to 20% of the pericardium (6). It should be noted that the MPE is an indicator of poor prognosis; it can show some signs of impending cardiac tamponade and is clinically characterized by a hemodynamic instability secondary to increased pressure due to a pericardial fluid accumulation that requires emergent decompression maneuvers (7, 8).
A chest x-ray is a diagnostic help which can show, in some cases, an enlarged and rounded cardiac silhouette; however, this finding can be limited by the presence of other thoracoabdominal entities. It presents a low sensibility and specificity. Transthoracic echocardiography is another diagnostic tool, which is the best diagnostic tool to evaluate a pericardial compromise, and followed by a computed tomography (CT) and a magnetic resonance imaging (MRI). These tools are useful in evaluating the presence of intrapericardial masses and pericardial effusion when ultrasonography is inconclusive (9,10). Another diagnostic tool is the biochemical and histopathological analysis of the pericardial effusion; it should be noted that there is the likelihood of false negatives due to a low concentration of tumor cells in the sample (11).
A pericardial effusion treatment aims to suppress its symptoms, restore hemodynamic stability and prevent recurrence (6).There has been evidence of a recurrence rate of 40% of MPE in patients who do not receive additional treatment such as continuous drainage catheter, performing a pericardial window or sclerosing therapy (12). The objective of this article is to present a malignant pericardial effusion case, since this clinical condition implies a diagnostic challenge.
Case report
A 63-year old male patient from Bucaramanga, Colombia; with one month of clinical evolution characterized by the presence of cervical lymphadenopathy initially painful, with progressive enlargement, associated with fatigue and adynamia. Over the past 15 days, he has been presenting early satiety, night sweats, feeling of abdominal distension and impaired functional class to dyspnea when doing small efforts; this was the reason why he consulted the emergency department at a tertiary institution in the metropolitan area of Bucaramanga (Colombia). Systems review referred oliguria, dark urine, and weight loss of approximately 3 kilograms in the last month. Personal history of importance showed arterial hypertension in treatment and exposure to organic material (straw) for 10 years.
The physical exam during his admission revealed that the patient is alert, oriented, and collaborative with vital signs of AP: 129/80 mmHg and CF: 93 per minute, oxygen saturation of 93%, and a temperature of 36.5C. His oral mucosa i s dried, r ight submaxillary cervical lymphadenopathies of approximately 3X4 cm, jugular ingurgitation grade I, cardiac rhythm veiled with a murmur, pulmonary sounds diminished with expiratory wheezing and moist rales in the left lung base. Abdomen distended with tympanic percussion, without masses or adenopathies. Left axillary region with an adenomegalia of 3X2 cm, not painful, of rubbery consistency, mobile; and a palpable mass in the right scapular region of approximately 6X3 cm, rubbery consistency, and painful during palpation. D uring the initial assessment, laboratories tests were requested and the results showed eight times, from its normal value, elevated transaminases, hyperbilirubinemia at the expense of direct, hyperlactatemia and impaired renal function; his chest radiography has an increased heart silhouette; also, retrocardial opacity was observed without the air bronchogram (Figure 1).
Moreover, hypotension, tachypnea, hypoventilation predominantly of left basal hemi thorax was documented during his clinical stay; the volume resuscitation maneuvers were initiated with a partial response; therefore, an ultrasound was performed with pericardial window, in which the presence of pericardial effusion was observed (approximately 400cc). A simple and contrasted thoracoabdominal CT was performed; it was identified an endobronchial lesion affecting one of the left lower lobe bronchus, apparently in the apical segment, mediastina lymphadenopathy and severe pericardial effusion (Figure 2); also, an osteolytic lesion in the right scapula suggestive of metastases (Figure 3). At the abdominal level, bilateral adrenal masses of probable metastatic origin and free liquid in abdominal cavity of moderate quantity were observed. The patient rapidly progresses to hemodynamic instability, persistent hypotension, tachycardia, veiled heart sounds, intolerance decubitus, and jugular grade II ingurgitation; in ECG monitoring, low voltage in all leads was observed with signs of early repolarization, reason why cardiac tamponade was suspected.
Figure 1. CHEST X-RAY. Widened mediastinum and retrocardiac opacity showing no air bronchogram.
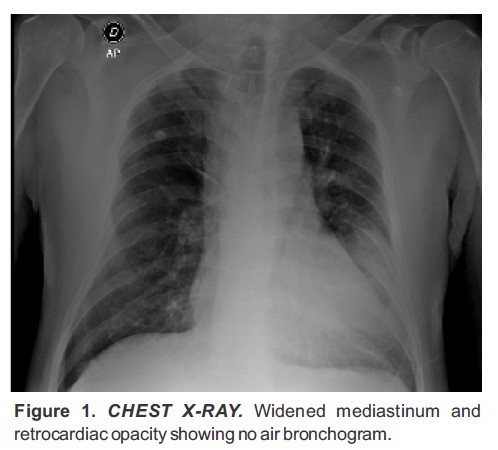
Figure 1
CHEST XRAY Widened mediastinum and retrocardiac opacity showing no air bronchogram
Figure 2. CHEST CT. (A) Endobronchial lesion involving one of the left lower lobe bronchus. (B) Important pericardial effusion, (C) Mediastinal adenopathy and left axillary adenopathy.
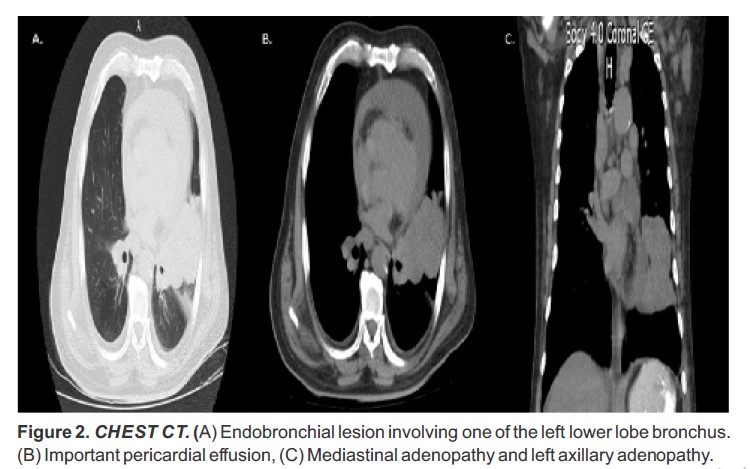
Figure 2.
CHEST CT. (A) Endobronchial lesion involving one of the left lower lobe bronchus. (B) Important pericardial effusion, (C) Mediastinal adenopathy and left axillary adenopathy.
Figure 3. CHEST CT. Osteolytic lesion in right scapula.

Figure 3
CHEST CT Osteolytic lesion in right scapula
A general surgery was performed. It was executed under ultrasound guidance and confirmation of a decompressive pericardiocentesis and pericardiotomy with catheter placement for drainage, draining a total of 300 mL of serohematic fluid, achieving hemodynamic compensation and electrocardiogram voltage increase, sinus rhythm, and wide QRS in cardiovisoscopy. The fluid was sent for biochemical and histopathology study. The cytology study showed positive for malignancy, suggestive of adenocarcinoma.
This was a study of the pericardial fluid cell block with adenocarcinoma compromise of micropapillary pattern. This immunohistochemistry was consistent with pulmonary origin. The patient was moved to intensive care unit, with evolution within management goals, hemodynamically stable without ventilator requirements or vasopressor support. Therefore, patient was transferred to continue his hospitalization out of the ICU. Once the patient was stable, a CT-guided lung biopsy performed by interventional radiology was requested; however, the patient and his family did not give their consent for the procedure, and requested voluntary discharge seeing that the patient has a stable condition.
On the second day after hospital discharge, the patient entered to the emergency department after approximately 48 hours. His clinical condition was characterized by pain in the right scapular region of 9/10 intensity according to the analog scale of pain radiating to the right arm, without response to analgesic management. He also refers that 12 hours ago, he started with a progressive dyspnea when doing small efforts. Upon physical examination the patient was alert, conscious, irritable, oriented, without oxygen support, with decreased peripheral pulses, blood pressure readings with a tendency to hypotension, decreased breath sounds in left part of the chest, veiled heart sounds without murmurs, and the rest of the examination is unchanged. Therefore, extension tests and a transthoracic echocardiogram, which showed ejection fraction between 55 and 60%, pericardial thickening and constriction and mild pericardial effusion were ordered, reason why cardiology ruled out the suspicion of cardiac tamponade. Close clinical surveillance was continued, with a favorable evolution. The family and patient agreed to perform the biopsy and the procedure was performed without any complications, pathology reports confirmed adenocarcinoma of micropapillary pattern, so an integrated management was continued.
Discussion
MPE is an indicator of poor prognosis and clinically, patients may present signs of impending cardiac tamponade which is associated with high mortality. Pathophysiologically, it is explained by the progressive accumulation of pericardial fluid, which leads to an alteration of ventricular filling, directly causing a decrease in cardiac output, and hemodynamic repercussions. That is why it was given importance and insisted on making use of semiology, since the MPE can be suspected with the presence of jugular ingurgitation, veiled heart sounds, and hypotension, which is known as Beck's triad or with the presence of a paradoxical pulse (13, 14).
Our patient initiated with a short clinical evolution with rapidly progressive symptoms, leading him to a state of marked functional class deterioration. Initially with stable vital signs, but during medical observation he showed hemodynamic decompensation of abrupt onset requiring an urgent treatment. This is the reason why doctors always insist on performing, in the emergency department, an early approximated diagnosis and start a subsequent comprehensive management to identify the source of the clinical problem; therefore, preventing disease progression and further complications is important, such as cardiac tamponade, which is an event that involves significantly hemodynamic parameters and if there is not an appropriate treatment plan, this will quickly lead to the death of the individual (15,16).
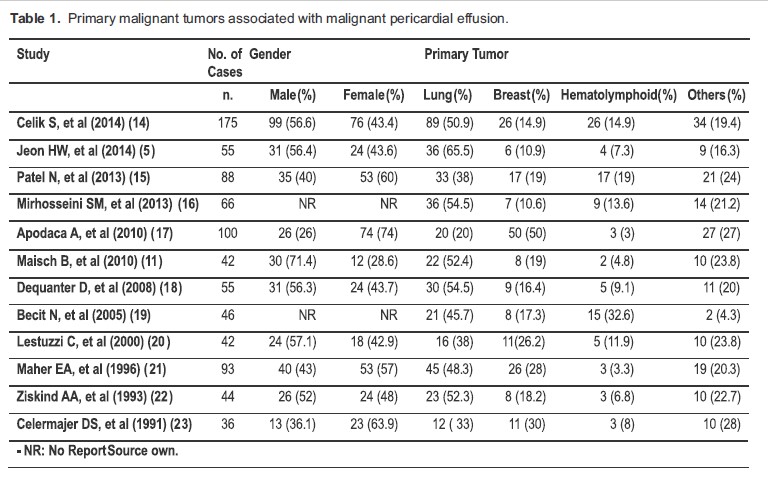
The prognosis of patients that present MPE is poor and is directly related to the primary source of the malignancy and sensitivity to the anticancer treatment. The tumors that frequently compromise the heart are those from pulmonary, breast, and hematolymphoid origin (table 1). It is important to remember that lung cancer has a higher rate of MPE recurrence and lower survival when compared to tumors of breast origin or hematolymphoid (9). In this case, the patient presents with advanced primary malignancy of pulmonary origin, although the prognosis of these patients in the short term is poor, deserves a comprehensive approach in order to prevent complications and improve the quality of life of patients.
Regarding to diagnostic tools, there is a wide range of tests and when they are used along with the clinical approach, are very useful in the emergency department of a health care center. In the case of suspected pericardial effusion or cardiac tamponade, the imaging tests should be considered as the first choice since it has been shown that the contribution of these generate a timely diagnosis of a life- threatening entity (17-20). Chest radiograph usually shows an increase in the size of the cardiac silhouette as a sign of pericardial effusion; however, it is important to note that there is a group of patients, who initially this radiographic feature is not evidenced of anything, so that this may be because they have little PE at the time of the exam (21-23). Some of these patients tend to quickly accumulate fluid in this space, generating an unexpected clinical setting of cardiac tamponade (24). As an example of this was the patient of this case, whose chest radiograph shows an increase in the cardiac silhouette associated with retrocardiac opacity without the air bronchograms.
In this case, the medical staff often gives more importance to certain findings; for example in this clinical case, the emphasis on the retrocardiac is the opacity and did not conduct a comprehensive approach with all the imaging and initial clinical findings that the patient presented, leading him to a decompensation and some complications for him.
Moreover, the transthoracic echocardiogram is considered as the frontline for the diagnostic study of pericardial effusion, given its cost-effectiveness and high sensitivity and specificity, and a low risk for the patient (10).In patients with suspected cardiac tamponade, the most characteristic echocardiographic findings are the presence of pericardial effusion associated with collapse of the walls of the right atrium and/or right ventricle in diastole (8). Although, in some patients the presence of DP without the collapse of the atrial or ventricular walls is evident; so the patients should be strictly monitored since much of this rapid progress to a hemodynamic instability is due to this monitoring. As this example showed if the patient had not done clinical monitoring and timely maneuvers decompression, the final outcome would have been his death. Also, the patient had a low voltage electrocardiogram (EKG), so it must be highlighted the importance of a proper performance and interpretation of EKG, since there is evidence of the association between cardiac tamponade and the low voltage in the electrocardiographic tracing, along with a considerable diagnostic accuracy (10, 25).
Table 1. Primary malignant tumors associated with malignant pericardial effusion.
The management and an ideal treatment of MPE still remains as a topic of controversy since there are minimally invasive techniques that are associated with a higher probability of recurrence. Although, there are techniques that need to be performed in a surgical area, but with a lower recurrence rate of effusion (16). That is why, it is very important to individualize management according to the clinical evolution and specific requirements of each clinical presentation.
Among the different procedures performed to drain a PE, pericardiocentesis is the fastest procedure that can be performed and carried out in the reanimation room. This procedure is indicated in patients with clinical signs and / or imaging of cardiac tamponade, or for those who are presenting an imminent risk of tamponade or as a diagnostic method in cases that pericardial effusion of malignant origin is suspected (9). Therefore, it is important to point out that if you are in a hospital that has the necessary elements for the pericardiocentesis and trained personnel, the procedure should be performed on time without any delays when making this decision; also, take into account the risk-benefit present in these patients in order to avoid complications in their health.
Nowadays, there is a triage strategy for the cardiac tamponade emergency management of the European Society of Cardiology. Members propose a step scoring system for the classification of the patient requiring urgent percutaneous drainage or surgery if the patient´s process is delayed. This classification is divided into three steps with their respective punctuations. The first step refers to the etiology. The second to the clinical manifestations; the third refers to the imaging findings, if the sum gives a greater or equal value to 6, so the performance of urgent pericardiocentesis is indicated (25). In this clinical case, the patient had a rating more than 6, indicating the performance of the method already described.
Other procedures to be performed are the subxiphoid pericardiotomy, thoracoscopic pericardiotomy, sternotomy pericardiotomy, and thoracotomy pericardiotomy. It is very important to evaluate the necessity and appropriateness of the procedure with a comprehensive approach to determine the risk and benefit for each particular case (26).
Conclusions
The malignant pericardial effusion is an event with imminent risk to patients' lives. In some cases, its clinical manifestations are of sudden onset. Therefore, it is very important to make an early diagnosis and initiate with all necessary measures to prevent fatal outcomes as a result of the progression of cardiac tamponade; although in some individuals, the prognosis is poor.
Conflict of interests
The authors declare that there is no conflict of interests regarding the publication of this paper.
Acknowledgments
Special thanks to the Department of Radiology and Research Center - FOSCAL, for their support.
References
1. Petrofsky M. Management of Malignant Pericardial Effusion. J Adv Pract Oncol. 2014 Jul-Aug; 5(4):281-9.
2. Kopcinovic LM, Culej J. Pleural, peritoneal and pericardial effusions - a biochemical approach. Biochem Med. 2014 Feb 15; 24(1):123-37.
3. Kim SH, Kwak MH, Park S, Kim HJ, Lee HS, Kim MS, et al. Clinical characteristics of malignant pericardial effusion associated with recurrence and survival. Cancer Res Treat. 2010 Dec;42(4):210-6.
4. El Haddad D, Iliescu C, Yusuf SW, William WN, Khair TH, Song J, et al. Outcomes of Cancer Patients Undergoing Percutaneous Pericardiocentesis for Pericardial Effusion. J Am Coll Cardiol. 2015 Sep 8;66(10):1119-28.
5. Jeon HW, Cho DG, Park JK, Hyun KY, Choi SY, Suh JH, et al. Prognostic factors affecting survival of patients with cancer-related pericardial effusion managed by surgery. World J Surg Oncol. 2014 Aug; 5(12):249.
6. Virk SA, Chandrakumar D, Villanueva C, Wolfenden H, Liou K, Cao C. Systematic review of percutaneous interventions for malignant pericardial effusion. Heart. 2015 Oct;101(20):1619-26.
7. Jama GM, Scarci M, Bowden J, Marciniak SJ. Palliative treatment for symptomatic malignant pericardial effusion. Interact Cardiovasc Thorac Surg. 2014 Dec;19(6):1019- 26.
8. Jung HO. Pericardial effusion and pericardiocentesis: role of echocardiography. Korean Circ J. 2 0 1 2 Nov;42(11):725-34.
9. Lestuzzi C, Berretta M, Tomkowski W. 2015 update on the diagnosis and management of neoplastic pericardial disease. Expert Rev Cardiovasc Ther. 2015 Apr;13(4):377-89.
10. Gumrukcuoglu HA, Odabasi D, Akdag S, Ekim H. Management of Cardiac Tamponade: A Comperative Study between Echo-Guided Pericardiocentesis and Surgery-A Report of 100 Patients. Cardiol Res Pract. 2011;(11):19783-8.
11. Maisch B, Ristic A, Pankuweit S. Evaluation and management of pericardial effusion in patients with neoplastic disease. Prog Cardiovasc Dis 2010;(53):157- 63
12. Oida T, Mimatsu K, Kano H, Kawasaki A, Kuboi Y, Fukino N, et al. Pericardiocentesis with cisplatin for malignant pericardial effusion and tamponade. World J Gastroenterol. 2010 Feb 14;16(6):740-4.
13. Li BT, Pearson A, Pavlakis N, Bell D, Lee A, Chan D, et al. Malignant Cardiac Tamponade from Non-Small Cell Lung Cancer: Case Series from the Era of Molecular TargetedTherapy. J Clin Med. 2014 Dec 30;4(1):75-84.
14. Celik S, Lestuzzi C, Cervesato E, et al. Systemic chemotherapy in combination with pericardial window has better outcomes in malignant pericardial effusions. J Thorac Cardiovasc Surg 2014; 148:2288-93
15. Patel N, Rafique AM, Eshaghian S, Mendoza F, Biner S, Cercek B, et al. Retrospective comparison of outcomes, diagnostic value, and complications of percutaneous prolongeddrainage versus surgical pericardiotomy of pericardial effusion associated with malignancy. Am J Cardiol. 2013 Oct 15;112(8):1235-9.
16. Mirhosseini SM, Fakhri M, Mozaffary A, Lotfaliany M, Behzadnia N, Ansari Aval Z, et al. Risk factors affecting the survival rate in patients with symptomatic pericardial effusion undergoing surgical intervention. Interact Cardiovasc Thorac Surg. 2013 Apr; 16(4):495-500.
17. Apodaca A, Villarreal C, Torres B, Torres J, Meneses A, Flores D, et al. Effectiveness and prognosis of initial pericardiocentesis in the primary management of malignant pericardial effusion. Interact Cardiovasc Thorac Surg. 2010 Aug; 11(2):154-61.
18. Dequanter D, Lothaire P, Berghmans T, Sculier JP. Severe pericardial effusion in patients with concurrent malignancy: a retrospective analysis of prognostic factors influencing survival. Ann Surg Oncol. 2008 Nov; 15(11):3268-71.
19. Becit N, Unlü Y, Ceviz M, Koçogullari CU, Koçak H, Gürlertop Y. Subxiphoid pericardiotomy in the management of pericardial effusions: case series analysis of 368 patients. Heart. 2005;91(6):785–790.
20. Lestuzzi C, Viel E, Sorio R, Meneguzzo N. Local chemotherapy for neoplastic pericardial effusion. Am J Cardiol. 2000 Dec 1;86(11):1292.
21. Maher EA, Pastor FA, Todd TJ. Pericárdico esclerosis como la gestión principal de derrame pericárdico maligno y taponamiento cardíaco. J Thorac Cardiovasc Surg 1996 Sep; 112 (3): 637 - 43.
22. Ziskind AA, Pearce AC, Lemmon CC, Burstein S, Gimple LW, Herrmann HC, et al. Percutaneous balloon pericardiotomy for the treatment of cardiac tamponade and large pericardial effusions: description of technique and report of the first 50 cases. J Am Coll Cardiol. 1993 Jan; 21(1):1-5.
23. Celermajer DS, Boyer MJ, Bailey BP, Tattersall MH. Pericardiocentesis for symptomatic malignant pericardial effusion: a study of 36 patients. Med J Aust. 1991 Jan 7; 154(1):19-22.
24. LeWinter MM. Clinical practice. Acute pericarditis. N Engl J Med. 2014 Dec 18; 371(25):2410-6
25. Ristić AD, Imazio M, Adler Y, Anastasakis A, Badano LP, Brucato A, et al. Triage strategy for urgent management of cardiac tamponade: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2014 Sep 7; 35(34):2279-84.
26. Saltzman AJ, Paz YE, Rene AG, Green P, Hassanin A, Argenziano MG, et al. Comparison of Surgical Pericardial Drainage With Percutaneous Catheter Drainage for Pericardial Effusion. J Invasive Cardiol. 2012 Nov; 24(11):590-3.
Author notes
José Mauricio Chilatra Fonseca. Universidad Autónoma de Bucaramanga, Calle 157 No. 19-55 Cañaveral Parque Floridablanca, Santander, Colombia. Telephone: +57 317 625 9367. Email: jchilatra@unab.edu.co
Alternative link
https://revistas.unab.edu.co/index.php/medunab/article/view/2298/2343 (pdf)