Article
A feasibility study for a new one-day protocol for [99mTc]TcDTPA2- and [99mTc]TcDMSA2- renal scintigraphy on dilated and non-dilated pediatric patients: underlying rationale
A feasibility study for a new one-day protocol for [99mTc]TcDTPA2- and [99mTc]TcDMSA2- renal scintigraphy on dilated and non-dilated pediatric patients: underlying rationale
Brazilian Journal of Radiation Sciences, vol. 11, no. 1, e2158, 2023
Sociedade Brasileira de Proteção Radiológica
Received: 22 November 2022
Accepted: 28 February 2023
Published: 14 March 2023
Abstract: Purpose. This work aimed at evaluating the possibility of performing renal exams of dynamic renal (DRS) and static renal (SRS) scintigraphy on the same day (one-day protocol, ODP), exams that are currently performed in two days. Approach. 25 infants (50 kidneys) of both genders, aged 8.4 ± 5.9 years, underwent an F+20 DRS protocol with [99mTc]TcDTPA2- followed by [99mTc]TcDMSA2- administration for the performance of SRS images at 3, 6 and 24 h. Dynamic images (DRS) were classified as dilated (D), undetermined (U), and non-dilated (P). Static images (SRS) were classified as: depressed in accented degree (DA); depressed in moderate degree (DM); depressed in mild degree (DL) and normal (NL). Results. Out of the 25 patients (50 kidneys), 7 (14 kidneys) were excluded by functional exclusion, hence 18 patients (36 kidneys) were clinically compared regarding their static images after 3, 6 and 24 h, resulting in 33.0% of dilated and 66.7% non-dilated. Only two patients of the dilated group were classified as obstructed. At the group with non-dilated and dilated but non-obstructed kidneys, 100% of them had the same clinical classification at 6 and 24 h images. Conclusions. Performance of both DRS and SRS exams in a single day for pediatric patients, when medical requests are carried out jointly, is feasible in a population with or without dilatation, when the difference between dynamic and static images is of at least 6 h. Due to the small number of obstructed kidneys in this study, further evaluation in this population is needed.
Keywords: Radionuclide Imaging, Pediatric Nephrology, Renal cortical scintigraphy.
1. INTRODUCTION
The prevention, diagnosis and therapy of pathologies involving the urinary system are of great importance in the clinical practice, as the incidence of renal replacement therapy in children aged from 0-18 years-old in 2008 was 9 per million and the congenital abnormalities respond from two thirds of renal failure in developed countries. Hydronephrosis is a common finding on antenatal ultrasound, that ranges from 1% to 5% of all pregnancies, and is defined as dilatation of the renal pelvis with or without calyces dilatation being the most frequently causes: transient dilatation and Congenital Anomalies of the Kidney and Urinary Tract (CAKUT) [1]. Renal scintigraphies are aimed at evaluating the anatomy and metabolism of the kidneys. The formation of the image occurs through the use of radiopharmaceuticals and their passage and/or fixation in the target organ [2,3]. Imaging tests using radiopharmaceuticals for renal evaluation obey the physiological renal glomerulus-tubular principle (Figure 1).
![Illustration of a nephron and distribution of each tracer. [99mTc]TcDTPA2- glomerular filtration at the glomerulus; [99mTc]TcMAG32 proximal tubule secretion; and [99mTc]TcDMSA2- proximal and distal tubular uptake. Image prepared using the web-based software BIODIGITAL - The BioDigital Human Platform, version 4.0 (available at: https://human.biodigital.com/explore).](../2158-figure1.jpg)
Figure 1
Illustration of a nephron and distribution of each tracer. [99mTc]TcDTPA2- glomerular filtration at the glomerulus; [99mTc]TcMAG32 proximal tubule secretion; and [99mTc]TcDMSA2- proximal and distal tubular uptake. Image prepared using the web-based software BIODIGITAL - The BioDigital Human Platform, version 4.0 (available at: https://human.biodigital.com/explore).
99mTc-labeled mercaptoacetyltriglycine, [99mTc]TcMAG32-, is the most widely used in the United States. [99mTc]TcMAG32- has a few advantages over [99mTc]TcDTPA2-, especially because of the extensive clinical experience with this tracer and for its characteristics of tubular absorption that can give information about kidney flow and relative kidney function at the same study with good accuracy [4,5]. Unfortunately [99mTc]TcMAG32- is not available in Brazil, being the combination of [99mTc]TcDTPA2- (99m-technetium diethylenetriamine penta-acetic acid) and [99mTc]TcDMSA2- (99m-technetium 2,3-dimercaptosuccinic acid) used at this country [6,7] for dynamic renal scintigraphy (DRS) and static renal imaging (SRS), respectively, based on the European Society of Nuclear Medicine (EANM) determined guidelines for renal scintigraphy [8,9]. [99mTc]TcDTPA2- is similar to inulin, circulates in the blood with insignificant binding to plasma proteins and does not penetrate into red blood cells, being simply filtered into the glomerulus [10,11], with the curve of disappearance of [99mTc]TcDTPA2- from the plasma showing that in 24 h the remainder is only 5-10% of the injected dose and, after 6 h, 80% of the injected dose passed through the urinary bladder [12,13]. Dynamic Renal Scintigraphy (DRS) includes the administration of Furosemide, being a well-accepted technique for differentiating obstructive from non-obstructive uropathy, by the increase of urinary flow and to reduce the amount of tracer at the renal pelvis that can overestimate the relative kidney function [7,9,14]. The DRS with the radiopharmaceutical [99mTc]TcDTPA2- is extremely important for surgical planning in patients with pyeloureteral junction stenosis, assessing the need for pyeloplasty and ureteroplasty, i.e., for assessment of renal obstruction states [15,16].
The radiopharmaceutical [99mTc]TcDMSA2- is preferentially accumulated in the renal cortex, allowing to obtain well-defined images of the renal parenchyma by its characteristics of having a slower plasma disappearance when compared to other radiopharmaceuticals used for renal scans [10]. By determining the presence of scars, determined by infection or by increased pressure on collector system, and the tubular relative function, it is the radiopharmaceutical of choice for Static Renal Scintigraphy (SRS) [8,16,17]. As described before, hydronephrosis has a high impact on pediatric population, and the currently available protocols (separate days), aiming to reduce the impact of pelvis radiotracer retention, and overestimation of relative kidney function, especially in patients with high degree of renal obstruction, brings with it the need of two peripheral venous punctures, becoming a major challenge for healthcare providers [18–21].
It is common for DRS and SRS to be jointly requested by nephrologists, to assess urinary tract patency via DRS and its morphological status via SRS [18,19,22–25]. In the currently available protocols, these tests should be performed on separate days [26], since the images obtained via DRS in patients with high degrees of renal obstruction could interfere with the cortical images obtained via SRS [9,20]. The largest public that uses these tests is the pediatric one, displaying the highest rate of complications derived from peripheral venous puncture [27]. Adding to this, in the current gold standard protocol, patients are required to perform the renal exams in two days [11,16,28,29], DRS being the first one to be performed and image acquisition initiated immediately after administration of the radiopharmaceutical [99mTc]TcDTPA2-, with an approximate duration of 1 h. Approximately 24 h after performing DRS, SRS is started using the radiopharmaceutical Tc-99m DMSA. Following administration of [99mTc]TcDMSA2-, a time period of ca. 2-3 h is expected for the radiopharmaceutical to be metabolized (due to its biodistribution) and image acquisition is initiated, with an average duration of 40 min. This is the protocol used in most Brazilian clinics, including the Institute of Diagnosis of Sorocaba (IDS) (Sorocaba/SP, Brazil), where this study took place. The nuclear medicine sector of the philanthropic institution Santa Marcelina (São Paulo/SP, Brazil) also follows the two-day protocol, however, due to the outsourced service and availability of days when the sector works, the exams end up being carried out with an interval of seven days.
As studies reported in the literature indicate that the radiopharmaceutical used in DRS is totally released after a period of 24 h following administration, thus ensuring non-interference in the SRS test [26,28,29]. However, in the two-day protocol there is the need for patients to be available for a longer time, which may have an impact on both the adult and pediatric populations, in addition to the aggravating factor of the inevitability of two peripheral venous accesses, something that can be particularly harmful to children [30]. No arguments were found in the literature against carrying out the one-day protocol [9,11,12,20]. Aiming at both convenience and comfort for the patient, by reducing the number of venous punctures required, the study reported herein aims to evaluate the feasibility of a "one-day protocol" with [99mTc]TcDTPA2- and [99mTc]TcDMSA2- scintigraphy on dilated and non-dilated pediatric population.
2. MATERIALS AND METHODS
The prospective research work reported herein was approved by the Research Ethics Committee of the University of Sorocaba (authorization nº 2.328.023, of October 2017). All patients gave written informed consent before enrollment. No patients were sedated in this study. Patients aged between 7-12 y-old were presented with a free and informed consent term (accompanying a cartoon especially developed to allow an easy understanding of the procedure), in adequate language, according to the requirements indicated in Resolution nº 466 of December 12th, 2012, of the Brazilian National Health Council [31].
A total of 25 patients from both genders (9 males and 16 females, aged 8.4 ± 5.9 years-old) with medical indication for static (SRS) and dynamic renal scintigraphy (DRS) from the Brazilian Public Health Network (SUS), were selected and enrolled in the prospective study only after approval by the Research Ethics Committee of the University of Sorocaba. The renal imaging examinations were carried out at the Nuclear Medicine Institute of Diagnosis of Sorocaba (IDS) (Sorocaba/SP, Brazil) at no costs to them.
The distribution of diagnosis or clinical indication of patients that entered the study reported herein is displayed in Table 1.
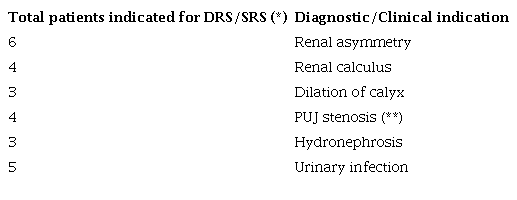
Notes: (*) DRS - Dynamic Renal Scintigraphy; SRS- Static Renal Scintigraphy (SRS); (**) PUJ stenosis - Pelviureteric junction (PUJ) stenosis.
Figure 2 displays the groups of analyzes that were undertaken.
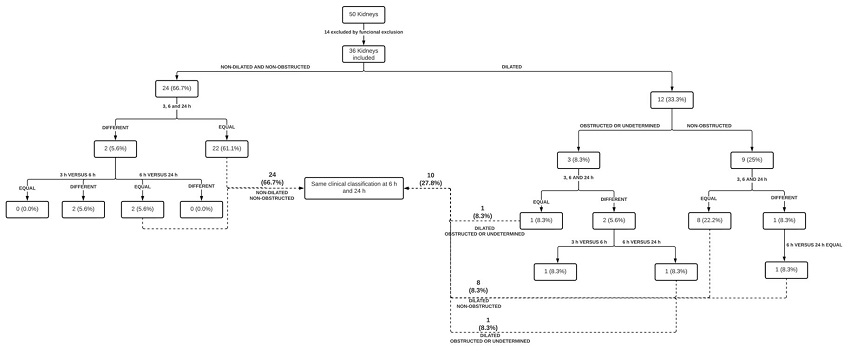
Figure 2
Schematic representation of the groups of analyzes that were undertaken in the research work reported herein.
The exclusion criteria were (i) no medical indication for both renal exams (DRS and SRS), (ii) patients younger than 2 y-old or older than two years old with inability to understand the informed consent, (iii) patients older than 18 y-old, (iv) pregnant women, (v) Functional exclusion at 3 h DMSA images, and (vi) patients with a single kidney. Hence, inclusion criteria were (i) medical indication for both exams (SRS and DRS), (ii) patients older than 2 y-old with ability to understand the informed consent, and (iii) patients younger than 18 y-old.
Dynamic and Static Renal scintigraphy imaging acquisition, evaluation, and classification. The DRS exam with [99mTc]TcDTPA2- (radiation activity: 3.7 MBq/kg (3.7 million Becquerels/kg), observing the maximum radiation activity of 200 MBq) was initiated after 30 min of administration of 3 cups of 200 mL of water, being performed in two phases: pre- and post-diuretic dynamics. Initial images: flow acquisition (1 image every 2 s during 1 min, matrix 64 x 64), followed by dynamic acquisition (1 image every 15 s during 20 min, matrix 256 x 256). Diuretic images: After 20 min of pre-diuretic images, furosemide with a dosage of 1 mg/kg, at a maximum dose of 20 mg [9], was administered followed by 20 min of dynamic acquisition (F+20 protocol [8]). After completion of the DRS exam, Static Renal Scintigraphy was initiated with administration of [99mTc]TcDMSA2- (radiation activity: 1.5 MBq/kg, observing the maximum radiation activity of 200 MBq), with acquisition of static images in the anterior, posterior, anterior oblique and posterior oblique projections at time intervals of 3 h, 6 h and 24 h following administration of [99mTc]TcDMSA2-, matrix 256x256 during 10 min or 1000 ktcs. Figure 3 illustrates the phases of the "one-day" protocol evaluated in this study.
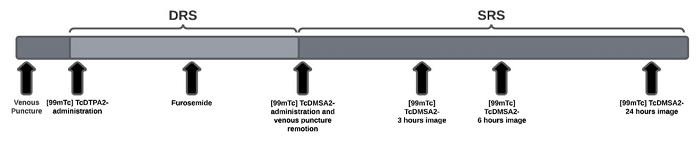
Figure 3
Schematics of the phases encompassing the "one-day" protocol evaluated in this study.
Image acquisition and Quality control. Image acquisition was performed in a Siemens Symbia T2 SPECT CT gamma camera (Siemens, Munich, Germany), using low energy, high resolution (LEHR) collimator, with a 20% energy window set at an energy peak of 140 keV. All radiochemical and radiophysical quality controls were performed according to the requirements of the Resolution of the Collegiate Board of Directors of the Brazilian Health Regulatory Agency (Resolução de Diretoria Colegiada - RDC Nº 38) [32]. The DTPA and DMSA used were reconstituted using a Tc-99m generator (Technetium-99m Generator, model IPEN-TEC, Cidade Universitária, São Paulo/SP, Brazil) [33], yielding [99mTc]TcDTPA2- and [99mTc]TcDMSA2-, respectively. The image matrix was set at 64x64 (2 s/frame) or 256x256 (15 s/frame) for SRD, and 256x256 (1000 ktcs or 10 min) for SRS, respectively.
Image processing. The images were processed in a Symbia.net™ Clinical Workflow Server (Siemens Medical Solutions Inc., Malvern PA, U.S.A.), with the contours of each kidney (regions of interest, ROI) and the corresponding backgrounds being drawn automatically via Symbian software and by four other operators, in order to obtain the final value of the count rates of the regions of interest (ROI), by calculating the average of these five measures. The average images gathered after 3h, 6h and 24h, for SRS, were compared via statistical analysis of variance (ANOVA), and comparison of the average images obtained after 3h with the images obtained after 6h and the images obtained after 6h with the images obtained after 24h via statistical t-student test. All statistical analyses were carried out with the software Origin® 8 (OriginLab Corporation, Northampton MA, U.S.A.), considering a statistical level of significance of 5%.
There was, however, no comparison between the two-days protocol and the proposed one-day protocol, since unnecessary exposure of pediatric patients to ionizing radiation would not be justified due to the need to perform four examinations in a short period of time. Hence, one decided to discuss the findings of the study entertained herein through the analysis of the static images after 24 h following administration of the radiopharmaceutical [99mTc]TcDMSA2-, considered as the gold standard protocol in the current study.
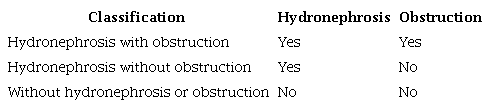
For analysis of the results, dynamic images were classified according to hydronephrosis and obstruction, as described in Table 2.
Static images were classified according to relative tubular function as normal, depressed in mild degree, depressed in moderate degree, depressed in accented degree, and as functional exclusion (Table 3).
Statistical analysis. The results of the average values obtained from the ROIs of the renal images acquired after 3 h, 6 h and 24 h following administration of the radiopharmaceutical [99mTc]TcDMSA2- were statistically compared. The most robust hypothesis that would allow the adoption of the one-day protocol would be accepted if all the averages of the ROIs of the renal images obtained after 3 h, 6 h, and 24 h were statistically the same, considering a significance level of 5%. However, we also considered that the one-day protocol could be adopted if the mean values obtained from the renal imaging counts for timeframes 6 h and 24 h were the same. To reduce the likelihood of operator interference in the image analysis, we used five data sets of ROIs, being one gathered automatically and four gathered by different operators. The statistical analyses were performed using the mean values obtained and their respective standard deviations. To compare the mean ROI values obtained after 3 h, 6 h, and 24 h in a single test, the data was statistically analyzed via analysis of variance (ANOVA). Comparison of the ROI averages after 3 h with the ROI averages after 6h and the ROI averages after 6 h with the ROI averages after 24 h was performed using the statistical t-student test. The statistical ANOVA test of Repeated Measures (within-subjects) was chosen, together with paired t-student test for multiple samples.
3. RESULTS AND DISCUSSION
All the kidney injuries listed in Table 1 can lead to a decrease in kidney function, which can be verified and diagnosed by static kidney scintigraphy, in addition to checking whether or not there are kidney scars.
Hydronephrosis is a common finding on antenatal ultrasound, that ranges from 1% to 5% of all pregnancies, and is defined as dilatation of the renal pelvis with or without calyces dilatation being the most frequently causes: transient dilatation and Congenital Anomalies of the Kidney and Urinary Tract (CAKUT) [1]. The Congenital anomalies are related to the fetal development and represented by Kidney Agenesis, Kidney hypoplasia, Ectopic Kidney / Horseshoe kidney, Vesico-ureteric reflux, Kidney dysplasia and Posterior urethral valves [34].
There is a relationship between CAKUT and the distribution of clinical indication of patients included in this study (Table 1).
Fifty kidneys were analyzed and 14 were excluded of the study because of functional exclusion (FE); hence, 36 kidneys were included in the study, and were initially classified on [99mTc] TcDTPA2-scintigraphy as dilated (12) and non-dilated (24), representing 33 and 66.7% of them. All of patients classified as non-dilated had the same [99mTc]TcDMSA2- clinical classification at 6 h versus 24 h but 2 (5.6%) had a different classification at 3 h versus 6 h. All the 9 patients (25%) considered as dilated but non-obstructed, had the same clinical classification at 6 h versus 24 h, but 1 (8.3%) had different images at 3 h versus 6 h images. These findings are in clear agreement with the current scientific literature, as the curve of disappearance of [99mTc]TcDTPA2- from the plasma shows that in 24 h the remainder is only 5-10% of the injected dose and, after 6 h, 80% of the injected dose passed through the urinary bladder [16].
For the sake of comparison, Figure 4 displays the results of a dynamic renal scintigraphy using [99mTc]TcDTPA2-, with total elimination of the tracer from the renal cortex into the urinary bladder along the timeframe of the assay.
![Results of a dynamic renal scintigraphy (DRS) using [99mTc]TcDTPA2-, with total elimination of the tracer from the renal cortex into the urinary bladder along time (A), together with associated normal renogram to determine if the kidney is dilated and/or obstructed (red line: left kidney; green line: right kidney; quantification was performed on posterior view) (B) and static renal scintigraphy (SRS) images demonstrating the absence of remnant material in the kidneys in the 24 h image (C).](../2158-figure4.jpg)
Figure 4
Results of a dynamic renal scintigraphy (DRS) using [99mTc]TcDTPA2-, with total elimination of the tracer from the renal cortex into the urinary bladder along time (A), together with associated normal renogram to determine if the kidney is dilated and/or obstructed (red line: left kidney; green line: right kidney; quantification was performed on posterior view) (B) and static renal scintigraphy (SRS) images demonstrating the absence of remnant material in the kidneys in the 24 h image (C).
In Figure 5 one can observe the results of a static renal scintigraphy using [99mTc]TcDMSA2-, considered without alterations (i.e. normal).
![Results of a [99mTc]TcDMSA2- image demonstrating the automatic contour of each kidney and corresponding backgrounds, considered without alterations (i.e. normal).](../2158-figure5.jpg)
Figure 5
Results of a [99mTc]TcDMSA2- image demonstrating the automatic contour of each kidney and corresponding backgrounds, considered without alterations (i.e. normal).
Data obtained via SRS, via analysis of the images gathered after 3h, 6h and 24h following administration of [99mTc]TcDMSA2-, allowed to classify the kidneys clinically according to the Relative Tubular Function (RTF) [35–39]. The RTF consists in determining the percentage of [99mTc]TcDMSA2- uptake by each kidney relative to the total amount of [99mTc]TcDMSA2- taken up by both kidneys, since the main theory explaining DMSA uptake implies in the initial filtration before its tubular reabsorption [40]. Therefore, the sum of the scintigraphy uptakes of both kidneys is always equal to 100%, with a maximum difference of 10% between the two kidneys (45% to 55%) being accepted as normal (Figure 5). Hence, the RTF system allows to classify the kidneys as 0-15% (functional exclusion, FE), 16-25% (depressed in accented degree, DA), 26-35% (depressed in moderate degree, DM), 36-45% (depressed in mild degree, DL), and >45 % (normal, NL) [41,42].
In this study, it was not possible to statistically analyze the kidneys that were classified as functional exclusion (FE). Clinical indication and findings obtained using DRS and SRS together with the results of the statistical analyses performed to the data are displayed in Table 4 and Table 5 for the right and left kidneys, respectively.
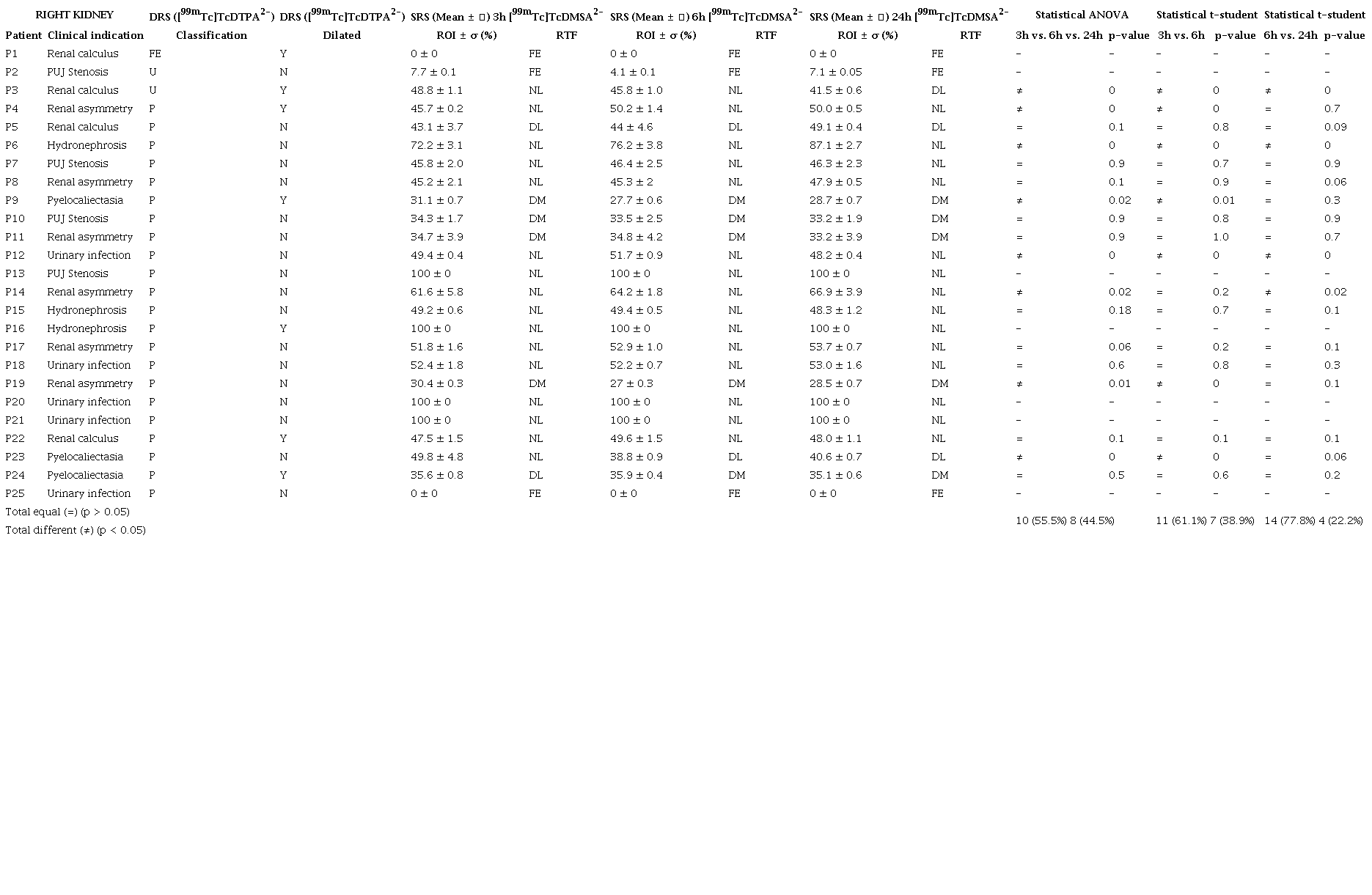
Legend: ROI, region of interest; RTF, Relative Tubular Function; O, obstructed; P, patent; FE, functional exclusion; U, undetermined; DA, depressed in accented degree; DM, depressed in moderate degree; DL, depressed in mild degree; NL, normal; Y, yes; N, no; , standard deviation.
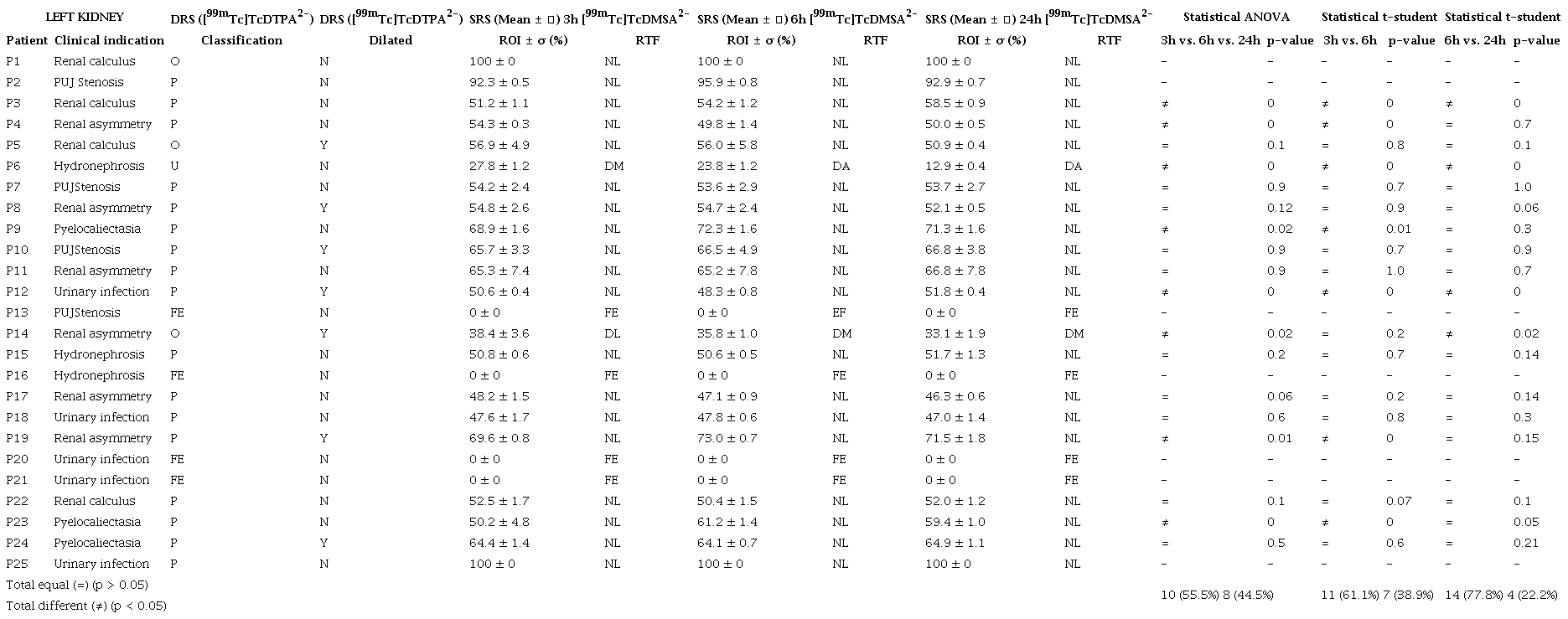
Legend: ROI, region of interest; RTF, Relative Tubular Function; O, obstructed; P, patent; FE, functional exclusion; U, undetermined; DA, depressed in accented degree; DM, depressed in moderate degree; DL, depressed in mild degree; NL, normal; Y, yes; N, no; , standard deviation.
The columns labeled with DRS (Table 4 and Table 5) bring, to each patient, the classification received by each kidney and whether or not the kidneys were dilated at the moment of the image analysis from DRS. The columns labeled with SRS (means 3h, means 6h and means 24) bring, to each patient, the classification received by each kidney at the moment of the SRS image analysis together with the RTF function.
In the columns labeled with Statistical ANOVA, the average ROI was compared for the images gathered after 3h, 6h, and 24h following administration of the radiopharmaceutical. The average ROI of the images obtained after those three time periods was classified with the symbol (=) when the statistical ANOVA provided a p-value > 0.05, considering a significance level of 5%. On the other hand, when the statistical ANOVA provided a p-value < 0.05, considering a significance level of 5%, the average ROI of the images obtained after those three time periods was classified with the symbol (≠). In the columns labeled with Statistical t-student, only two averages were compared, viz. the average value of ROI obtained after 3h was compared with the average value of ROI obtained after 6h, and the average value of ROI obtained after 6h was compared with the average value of ROI obtained after 24h, and the same symbols were attributed when p-value > 0.05 (=) or p-value < 0.05 (≠), considering a significance level of 5%.
One found, in the SRS image of patient P23, the presence of remnant material ([99mTc]TcDTPA2-) used in the DRS examination. This was observed in the image acquired after 3h following administration of the [99mTc]TcDMSA2-, as shown in Figure 6A and Figure 6B (inserted arrow). Figure 6 demonstrates the kidney pelvis tracer retention at 3 h images, but this pattern is not observed in the 6 h and 24 h imaging.
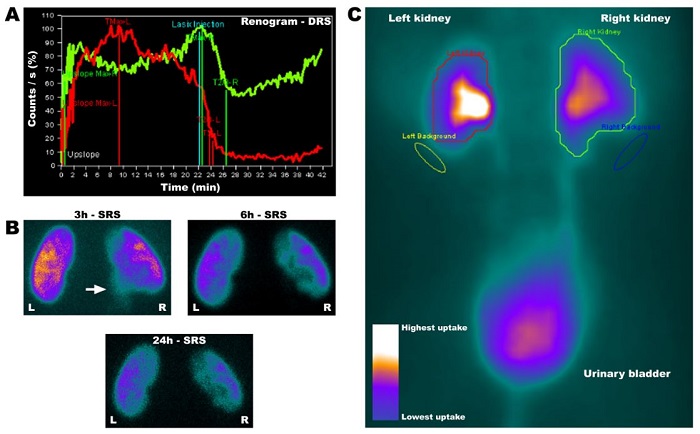
Figure 6
Renogram (DRS) of patient 23 (P23) evidencing the dilation and delay of elimination in the right kidney (green line), demonstrating retention of the radiotracer until the 20th min, with a decrease followed by increase of tracer retention after furosemide administration, resulting in an undetermined pattern (A); SRS images demonstrating the presence of remnant radiotracer in the right ureter in the 3 h image (B, inserted arrow) allowing to observe a retention of the tracer at renal pelvis on 3 h imaging, a pattern that is not demonstrated in the 6 h and 24 h images; and composed image integrating all images acquired during the 40 min exam, with a colorimetric scale (C).
In Figure 6C, one can observe the composed image integrating all images acquired during the 40 min exam, displaying the kidneys and urinary bladder. Departing from the ROIs, the plot displayed in Figure 6A is produced. The higher the uptake of radiotracer, the higher the accumulation of radioactive material. The higher uptake by the renal cortex is normal, since the radiotracer will pass into the ureters. In Figure 6C it is evident the color gradient produced in the image, with purple meaning the basal (normal), and the white meaning the higher uptake. The whiter region in Figure 6C corresponds to the renal cortex, meaning the largest uptake of radiotracer in that region.
Studies demonstrating the ideal moment for DMSA imaging on obstructed patients are controversy between 3 h, 5 h and 6 h, but there is a consensus that quantification after a period of 24 h following administration ensures non-interference in the SRS tests [43–45]. The study reported herein has only 3 (8.3%) of the kidneys with undetermined or urinary obstruction, what makes necessary a new investigation in this specific population; on the other hand, 32 patients (88.9%) presenting dilated or non-dilated but with non-obstructive pattern, had the same clinical classification at 6 h versus 24 h images.
Although [99mTc]TcMAG32- (mercaptoacetyltriglycine) is the standard of care for evaluation of renal obstruction, and in particular those listed in Table 1, unfortunately in Brazil there is only available [99mTc]TcDTPA2- for the evaluation of dynamic renal function. The reason for this is the lack of suppliers for [99mTc]TcMAG32- derived from the lack of authorization to import from abroad by ANVISA.
[99mTc]TcDTPA2- is a small molecule that freely diffuses in the extracellular space, without significantly binding to plasma proteins and, in this way, allows an excellent evaluation of glomerular filtration in addition to renal blood flow and function of the parenchyma, being indicated for DRS examination. There is a great (linear) correlation between the clearance of [99mTc]TcDTPA2- and inulin [46] and, in normal individuals, by the end of a maximum time of 1 h following administration of [99mTc]TcDTPA2-, there should be no remnants of the radiopharmaceutical in the renal cortex, with the radiopharmaceutical being primarily in the urinary bladder [38,47], as can be observed in Figure 4. The use of diuretics, especially furosemide, is recommended in order to eliminate the suspicion of functional stasis and renal obstructive states. On the other hand, [99mTc]TcDMSA2- is indicated for evaluating renal obstructive conditions and the impact of these conditions in renal function via SRS examination [18,23–25]. Following intravenous administration of [99mTc]TcDMSA2-, this radiopharmaceutical binds mainly in the proximal tubule of the renal cortex, without significant interference of the urinary flow in this mechanism of capture and, 2-3 h after administration, it reaches maximum tubular concentration. The preferential accumulation of [99mTc]TcDMSA2- in the renal cortex allows this tracer to remain for several hours in that region, making it possible to gather well-defined images in the SRS examination by associating functional characterization with morphological evaluation of the renal parenchyma ([99mTc]TcDMSA2- allows verification not only of the presence or absence of renal scars, but also allows quantification of the renal function). It is known that [99mTc]TcDMSA2- highly accumulates in the renal cortex [35,47]. Cortical scintigraphy (SRS) is usually performed upon indication of renal scars following recurrent episodes of renal infection, typically ascending Urinary Tract Infections (UTIs) from Vesicoureteral Reflux (VUR) or secondary to urinary anomalies such as calyceal diverticulum [25]. The proposal arising from the present research study could, with advantage, be implemented in locations without access to MAG3.
In this study, according to the classification obtained from Relative Tubular Function (RTF) [38,39,41,48], 10% of the kidneys were classified as "functional exclusion" and, therefore, did not enter the statistical tests performed to the experimental data.
Renal extraction of [99mTc]TcDMSA2- is ca. 4-5% per renal passage, with the kidneys concentrating approximately 50% of the [99mTc]TcDMSA2- dose injected after 1 h [10]. Urinary excretion of [99mTc]TcDMSA2- ranges from 4% to 8% of the dose injected after 1 h, from 8% to 17% after 2 h and from 26% to 30 % after 14 h. Hence, one observes that 6 h following administration of [99mTc]TcDMSA2- there is sufficient radiopharmaceutical in the renal parenchyma for good image acquisition. On the other hand, at the same time (6 h following its administration), more than 80% of the injected radiopharmaceutical [99mTc]TcDTPA2- dose has passed into the urinary bladder being rapidly eliminated [16,49].
This two-day protocol is usually requested by urologists specialized in pediatrics, on a regular basis. Nuclear medicine (NM) services routinely receive simultaneous requests for DRS (for evaluation of urinary tract patency) and SRS (for evaluation of renal morphology) examinations for the same patient. The first protocols proposed for these examinations date back from 1970-1980, having undergone few modifications since then. The American, European and Brazilian Societies of Nuclear Medicine have their own recommendation guidelines pertaining to these tests, with some variations regarding the radiopharmaceutical dose to be administered, time for acquiring the images, use of diuretics and the best time of patient return for image acquisition [20].
Currently, these tests are performed in two days. First, the DRS exam is carried out and, on another day, the SRS. In this two-day protocol, there is therefore the need not only for the patient to travel into the NM service to perform tests on separate days, but also to be subjected to at least two intravenous punctures. This practice is quite limiting, especially for pediatric patients. Historically, it has been performed this way to avoid remnants of [99mTc]TcDTPA2- in SRS images, such as those shown in Figure 6B (inserted arrow). As the indications relate to diagnosis of obstructive renal pathologies, this type of imaging artifact may occur, since patients who do not use the diuretic furosemide may have tracer accumulation in the kidneys due to renal obstructions. The use of furosemide enhances renal elimination of the tracer [99mTc]TcDTPA2-. Nevertheless, diuretics are used in SRS, which will promote greater renal diuresis, reducing the chances of interference in renal morphology images [11,12]. The proposed one-day protocol actually contributes to improving the quality of the service and, considering that a single peripheral puncture reduces the risks of accidents related to access, the hospital would save the daily costs of the procedures in pediatric patients. In addition, the one-day protocol would reduce the stress of the child and those responsible for returning to the hospital for two days in a row to perform DRS and SRS examinations that could be performed in a single day without much less discomfort, considering that the majority of the population served is of low income and the cost of transportation and the need to miss school and work makes it quite difficult for them to show up on the exam days. Indirectly, the one-day protocol proposed herein will increase throughput and efficiency in the NM department, since a patient would no longer occupy an extra examination day in the sector. The study entertained herein arose from the daily clinical need to perform both DRS and SRS in a single day. Pediatric patients are not collaborative when intravenous puncture is to be performed, and in many situations playful interventions are needed. Puncture failure is common, increasing the risk related to development of phlebitis [50], and this was the driving force for proposing the possibility of performing DRS and SRS in a single day. However, the main impediment for the implementation of the proposed one-day protocol would be the potential retention of the radiotracer in the pelvis of obstructed or dilated patients. However, based on pharmacokinetic and pharmacodynamic studies, it is believed that [99mTc]TcDTPA2- would have 80% of its activity in the bladder and no longer in the renal pelvis [10,20]. Currently, 24 h-images are used for those patients with suspicion of tracer retention in the renal pelvis, since it is believed that after 24 h there is no more pelvic remnants of the radiopharmaceutical. For this reason, the 24 h-images were chosen as the gold standard in the present study.
The use of diuretics in the proposed protocol would accelerate the elimination of [99mTc]TcDTPA2-, even in those patients with renal obstruction. With higher degrees of obstruction, however, clearance of the radiotracer would become more unpredictable. In addition, furosemide may not help in patients with severe renal obstruction displaying no improvement (flat curve) with post-furosemide curve. This would imply a higher probability of errors in the overall study from retention of initial radiotracer in the renal cortex. One way to avoid this confounding factor could be to control the data from ROI counts for degree of obstruction, but this approach was not followed in the present study.
Despite accelerating the elimination of tracer, the residence time of the radiotracers used and the results obtained in the imaging exams met the objectives of the DRS and SRS examinations for clarifying diagnosis and therapeutic indications. In addition, considering that the patients undergoing these examinations have some kidney disorder(s) to be studied and that some health professionals and children's parents fear the use of contrast reagents or radioactive agents, the use of furosemide in patients within the age group that entered the study is very well indicated and becomes more of a safety factor for the performance of the one-day protocol. Therefore, one gathered images after timeframes of 3 h following administration of [99mTc]TcDMSA2- (since after this timeframe the concentration of the radiotracer in the renal tubules reaches its maximum), 6 h following administration of [99mTc]TcDMSA2- (because the radiotracer still exhibits a high fixation in the renal cortex and studies indicate that more than 80% of the glomerular filtration tracer ([99mTc]TcDTPA2-) was previously eliminated), and 24 h following administration of [99mTc]TcDMSA2- (which would be free from any interference of [99mTc]TcDTPA2-, since it is known that more than 95% of this radiotracer is eliminated within said time (gold standard)) [10].
The results displayed in Table 4 and Table 5 considered the right and left kidneys, respectively, without functional exclusion. When we compare the means of the ROIs obtained after 3h, 6 h and 24 h, we have 55.5% of equal images, indicating that the one-day protocol could be adopted, but with a small margin of safety. This result was not better because the images acquired after 3 h following administration of the radiopharmaceutical [99mTc]TcDMSA2- still seemed to have the influence of the radiopharmaceutical [99mTc]TcDTPA2-, as was observed when comparing the averages of the images of the ROIs obtained after 3h with those obtained after 6h, still indicating a little similarity between them, viz. only 61.1%. However, when comparing the ROIs of the averages of the images obtained after 6 h with those obtained after 24h (gold standard) we found out that 77.8% of the images had no statistical difference (p > 0.05). The statistical difference did not exceed 15%, even with a little renal retention. In these cases, later images could be gathered, not requiring a new venipuncture.
Hence, we may conclude that if we take the image obtained after 6 h of administration of the radiopharmaceutical [99mTc]TcDMSA2- as reference for SRS, the one-day protocol can be used with absolute safety. Although the results obtained when performing both DRS and SRS exams in just one day were satisfactory and safe, it is important to establish which patients with kidney disorders would benefit the most from such a one-day protocol, since chronic kidneys with major dysfunction may have greater difficulty in eliminating the radioactive tracer. Patients with renal exclusion or younger than 2 years-old could not be analyzed by this study. In spite of this, we strongly believe that this new proposed protocol is promising for implementation in other NM services that use the two-day protocol, while promoting improvements in both quality and safety for pediatric patients. In spite of appearing as a long day for the families and children, in fact the proposed one-day protocol would simplify the life of the childrens' parents and would be more appealing for the children themselves.
The analysis can be extended to the entire population, since the patients who have the obstruction are the critical ones, that is, they are those in whom there could be retention of radioactive material in the kidneys, at the end of the study. Our work demonstrated that even in obstructed patients, renal retention was minimal and did not impair the analyses. For patients who do not have renal obstruction, in this way, they will also benefit from the one-day protocol, where they will not have material retention in the kidneys.
One day protocol for [99mTc]TcDTPA2- has been already described on kidney donors, but with blood sampling and [99mTc]TcMAG32- complementary images but, as this tracer is not available in Brazil, an alternative protocol is needed [51].
4. CONCLUSION
The performance of both DRS and SRS exams in a single day for pediatric patients, when medical requests are carried out jointly, is feasible in those patients with or without dilation, when the difference between dynamic and static images is of at least 6 h. Due to the small number of obstructed kidneys that entered the study reported herein, further evaluation in this population is needed. In spite of this, aiming at both convenience and comfort for the patient, by reducing the time of the examinations and the number of venous punctures required, the "one-day protocol" proposed herein could, without any harm whatsoever to those patients, replace the current gold standard protocol.
ACKNOWLEDGMENT
The authors acknowledge CAPES for the Postgraduate Support Program of Community Institutions of Higher Education (Prosuc) in the form of an MSc fellowship granted to Fabiana Trevisan. Funding for Victor M. Balcão through a BPE grant from FAPESP (São Paulo, Brazil) (Ref. No. 2018/05522-9, Project PsaPhageKill) is hereby gratefully acknowledged. This work also received support from CNPq, National Council for Scientific and Technological Development Brazil, in the form of Research Productivity (PQ) fellowships granted to Victor M. Balcão (Refs. No. 306113/2014-7 and 308208/2017-0). All freeze-dried kits used in this study were kindly donated by RPH Pharmaceuticals AB (Lagervagen, Sweden). The authors have no conflicts of interest whatsoever to declare.
REFERENCES
LEE, R.S.; CENDRON, M.; KINNAMON, D.D.; NGUYEN, H.T. Antenatal hydronephrosis as a predictor of postnatal outcome: a meta-analysis. Pediatrics, v. 118, p. 586-593, 2006.
ZANZONICO, P. Principles of nuclear medicine imaging: planar, SPECT, PET, multi-modality, and autoradiography systems. Radiat Res, v. 177, p. 349-364, 2012.
KHARFI, F. Principles and Applications of Nuclear Medical Imaging: A Survey on Recent Developments. In: KHARFI, F. Imaging Radioanal Tech Interdiscip Res - Fundam Cut Edge Appl [Internet], London: IntechOpen; Available from: https://www.intechopen.com/chapters/43519, 2013.
ARCHER, K.D.; BOLUS, N.E. Survey on the Use of Nuclear Renal Imaging in the United States. J Nucl Med Technol, v. 44, p. 223-226, 2016.
DURAND, E.; PRIGENT, A. The basics of renal imaging and function studies. Q J Nucl Med, v. 46, p. 249-267, 2002.
HAUSER, W.; ATKINS. H.L.; NELSON, K.G.; RICHARDS, P. Technetium-99m DTPA: a new radiopharmaceutical for brain and kidney scanning. Radiology, v. 94, p. 679-684, 1970.
LIN, C.C.; SHIH, B.F.; SHIH, S.L.; TSAI, J.D. Potential Role of Tc-99m DTPA Diuretic Renal Scan in the Diagnosis of Calyceal Diverticulum in Children. Medicine (Baltimore), v. 94, p. e985, 2015.
PIEPSZ, A.; COLARINHA, P.; GORDON, I.; HAHN, K.; OLIVIER, P.; ROCA, I.; SIXT, R.; VAN VELZEN, J.; Guidelines on 99mTc-DMSA scintigraphy in children. Eur J Nucl Med [Internet], v. 28, p. BP37-BP41, 2001.
GORDON, I.; PIEPSZ, A.; SIXT, R. Auspices of Paediatric Committee of European Association of Nuclear Medicine. Guidelines for standard and diuretic renogram in children. Eur J Nucl Med Mol Imaging, v. 38, p. 1175-1188, 2011.
ARNOLD, R.W.; SUBRAMANIAN, G.; MCAFEE, J.G.; BLAIR, R.J.; THOMAS, F.D. Comparison of 99mTc complexes for renal imaging. J Nucl Med, v. 16, p. 357-367, 1975.
KANE, S.M.; DAVIS, D.D. Technetium-99m. [Updated 2022 Sep 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559013/, 2022.
HUANG, S.H.; ELIASZIW, M.; SPENCE, J.D.; FILLER, G.; VEZINA, W.C.; CHURCHILL, D.N.; CATTRAN, D.C.; RICHARDSON, B.; HOUSE, A.A. The (99m)Tc-DTPA urinary clearance method may be preferable to the plasma disappearance method for assessing glomerular filtration rate in diabetic nephropathy. Nephron Clin Pract, v. 128, p. 367-372, 2014.
COMET, M.; VIDAL, M. Radiopharmaceutiques: chimie des radiotraceurs et applications biologiques. Grenoble: Presses Universitaires de Grenoble; 1998.
LEE, K.W.; BIN, K.T.; JEONG, M.S.; SHONG, M.H.; SHIN, Y.T.; RO, H.K. Tc-99m dimercaptosuccinic acid(DMSA) renal scintigraphy in patients with acute pyelonephritis. Korean J Intern Med, v. 10, p. 43-47, 1995.
WANG, Y.; LI, M.; DAI, S.; LI, Y. The Role of Tc-99m DTPA Renal Dynamic Scintigraphy in Retroperitoneal Liposarcoma. Biomed Res Int, v. 2020, p. 9765162, 2020.
DEMIR, F.; DEMIR, M. Comparison of 99mTc-DMSA, 99mTc-DTPA and 99mTc-MAG3 Renal Scintigraphy in the Calculation of Relative Renal Function. J Urol Surg, v. 7, p. 130-133, 2020.
ONEN, A. Grading of Hydronephrosis: An Ongoing Challenge. Front Pediatr, v. 8, p. 458, 2020.
DJEKIDEL, M.; GOVINDARAJAN, K.K. Nuclear Medicine Pediatric Assessment, Protocols, And Interpretation [Internet]. StatPearls [Internet], Available from: https://www.ncbi.nlm.nih.gov/books/NBK572132/, 2022.
ALSABEA, H. Types of Renal Scintigraphy. J Nucl Med Radiat Ther, v. 8, p. 347, 2017.
DE MAN, K.E.; TROCH, M.E.; DOBBELEIR, A.A.; DUONG, H.P.; GOETHALS, I.M. Comparison of the EANM and SNM guidelines on diuretic renography in children. Nucl Med Commun, v. 36, p. 486-448, 2015.
CHURCH, J.T.; JARBOE, M.D. Vascular Access in the Pediatric Population. Surg Clin North Am, v. 97, p. 113-128, 2017.
DOMINGUES, F.C.; FUJIKAWA, G.Y.; DECKER, H.; ALONSO, G.; PEREIRA, J.C.; DUARTE, P.S. Comparison of Relative Renal Function Measured with Either 99mTc-DTPA or 99mTc-EC Dynamic Scintigraphies with that Measured with 99mTc-DMSA Static Scintigraphy. Int Braz J Urol, v. 32, p. 405-409, 2006.
RAMBALDI, P.F.; ZUCCHETTA, P. Nuclear Medicine in Pediatric Nephro-urology. In: MANSI, L.; LOPCI, E.; CUCCURULLO, V.; CHITI, A. Clinical Nuclear Medicine in Pediatrics. Springer, Cham.; 2016.
SFAKIANAKIS, G.N.; SFAKIANAKI, E.D. Nuclear medicine in pediatric urology and nephrology. J Nucl Med, v. 29, p. 1287-1300, 1988.
FELD, L.G.; MATTOO, T.K. Urinary Tract Infections and Vesicoureteral Reflux in Infants and Children. Pediatr Rev, v. 31, p. 451-463, 2010.
BIASSONI, L. Pitfalls and Limitations of Radionuclide Renal Imaging in Pediatrics. Semin Nucl Med, v. 45, p. 411-427, 2015.
MORENO, E.A.C.; CARVALHO, A.A.S.; PAZ, E.P.A. Pain in child undergoing venipuncture: effects of an anesthetic cream. Esc Anna Nery, v. 18, p. 392-399, 2014.
SEBASTIANO, B.; SERENA, P.; LUANA, P. Nuclear medicine in the pediatric field. Journal of Advanced Health Care, v. 3, p. 36-65, 2021.
JANG, S.J. Nuclear Medicine in Pediatric Urology. Child Kidney Dis - Korean Soc Pediatr Nephrol, v. 19, p. 14-22, 2015.
ABDUL-HAK, C.K.; BARROS, Â.F. The incidence of phlebitis in a Medical Clinical Unit. Texto Context - Enferm, v. 23, p. 1-6, 2014.
CNS - Brazilian National Health Council. Resolution no 466, of December 12th, 2012, CNS - Brazilian National Health Council, 2012.
ANVISA - Agência Nacional de Vigilância Sanitária. Resolução de Diretoria Colegiada (RDC) no 38, de 4 de Junho de 2008. Anvisa, Brasília DF; 2008.
IPEN - Instituto de Pesquisas Energéticas e Nucleares. Gerador IPEN-TEC pertecnetato de sódio (99m Tc) [Internet]. IPEN - Inst Pesqui Energéticas Nucl, Available from: https://www.ipen.br/portal_por/portal/produtos.php?secao_id=35, 2022.
MURUGAPOOPATHY, V.; GUPTA, I.R. A primer on congenital anomalies of the kidneys and urinary tracts (CAKUT). Clin J Am Soc Nephrol, v. 15, p. 723-731, 2020.
ONO, C.R.; SAPIENZA, M.T.; MACHADO, B.M.; PAHL, M.M.C.; LIBERATO JR, W.P.; OKAMOTO, M.R.Y.; GARCEZ, A.T.; WATANABE, T.; COSTA, P.L.A.; BUCHPIGUEL, C.A. Standardization of a method to calculate absolute renal uptake of 99mTc-DMSA in children. Radiol Bras, v. 39, p. 33-38, 2006.
MORRIS, S.C.; CHITTENDEN, S.J.; RIVENS, I.; HEARY, T.A.; VANSTONE, C.; MELLER, S.T. Absolute 99Tcm-DMSA renal uptake in children: a study of 321 kidneys. Nucl Med Commun, v. 16, p. 566-571, 1995.
MOORIN, R. 99mTc-DMSA absolute uptake: normal pediatric values at 2-4 hours. J Nucl Med Technol, v. 29, p. 22-29, 2001.
MAJD, M.; BAR-SEVER, Z.; SANTOS, A.I.; DE PALMA, D. The SNMMI and EANM Procedural Guidelines for Diuresis Renography in Infants and Children. J Nucl Med, v. 59, p. 1636-1640, 2018.
VALI, R.; ARMSTRONG, I.S.; BAR-SEVER, Z.; BIASSONI, L.; BORGWARDT, L.; BROWN, J.; GRANT, F.D.; MANDELL, G.A.; MAJD, M.; NADEL, H.R.; NG, T.S.C.; ROCA-BIELSA, I.; ROHRINGER, T.J.; SANTOS, A.I.; SEGHERS, V.; SHAIKH, N.; TREVES, S.T.; ZAFFINO-NEVROTSKI, T.; ZUCCHETTA, P.; LIM, R. SNMMI procedure standard/EANM practice guideline on pediatric [99mTc]Tc-DMSA renal cortical scintigraphy: an update. Clin Transl Imaging, v. 10, p. 173-184, 2022.
WEYER, K.; NIELSEN, R.; PETERSEN, S.V.; CHRISTENSEN, E.I.; REHLING, M.; BIRN, H. Renal uptake of 99mTc-dimercaptosuccinic acid is dependent on normal proximal tubule receptor-mediated endocytosis. J Nucl Med, v. 54, p. 159-165, 2013.
GOUNDEN, V.; BHATT, H.; JIALAL, I. Renal Function Tests [Internet]. StatPearls [Internet], Available from: https://www.ncbi.nlm.nih.gov/books/NBK507821/, 2021.
LOWENSTEIN, J.; GRANTHAM, J.J. The rebirth of interest in renal tubular function. Am J Physiol Renal Physiol, v. 310, p. F1351-F1355, 2016.
VERBOVEN, M.; HAM, H.R.; JOSEPHSON, S.; COLLIER, F.; HALL, M.; PIEPSZ, A. 99Tcm-DMSA uptake in obstructed kidneys. How inaccurate are the 5 h measurements? Nucl Med Commun, v. 8, p. 45-48, 1987.
ZANANIRI, M.C.; JARRITT, P.H.; SARFARAZI, M.; ELL, P.J. Relative and absolute 99Tcm-DMSA uptake measurements in normal and obstructed kidneys. Nucl Med Commun, v. 8, p. 869-880, 1987.
PAUWELS, E.K.; LYCKLAMA À NIJEHOLT, A.A.; ARNDT, J.W.; JONAS, U. The determination of relative kidney function in obstructive uropathy with 99Tcm-DMSA. Nucl Med Commun, v. 8, p. 865-867, 1987.
HOLNESS, J.; FLEMING, J.; WARWICK, J. Measuring GFR Using the Plasma Clearance of 99mTc-DTPA. Am J Kidney Dis, v. 65, p. 806-809, 2015.
VADIVELU, K.; HILLER, J.; BRANNON, D.; REHMAN, B. Common pediatric nuclear medicine imaging studies: a comprehensive review, J Nucl Med, v. 63, p. 2664, 2022.
AGRICOLA, E.; MARINI, C.; STELLA, S.; MONELLO, A.; FISICARO, A.; TUFARO, V.; SLAVICH, M.; OPPIZZI, M.; CASTIGLIONI, A.; CAPPELLETTI, A.; MARGONATO, A. Effects of functional tricuspid regurgitation on renal function and long-term prognosis in patients with heart failure. J Cardiovasc Med (Hagerstown), v. 18, p. 60-68, 2017.
CHARYTAN, D.; KUNTZ, R.E. The exclusion of patients with chronic kidney disease from clinical trials in coronary artery disease. Kidney Int, v. 70, p. 2021-2030, 2006.
DE NEGRI, D.C.; AVELAR, A.F.M.; ANDREONI, S.; PEDREIRA, M.L.G. Predisposing factors for peripheral intravenous puncture failure in children. Rev Lat Am Enfermagem, v. 20, p. 1072-1080, 2012.
ROGASCH, J.M.M.; BAMM, M.; BÄDER, M.; JAESCHKE, E.; BRENNER, W.; VAN DER GIET, M.; AMTHAUER, H.; SCHATKA, I. Comparison of glomerular filtration rate (GFR) with Tc-99m-DTPA and tubular extraction rate (TER) with Tc-99m-MAG3 in potential living kidney donors: Feasibility of a one-day protocol. Nuklearmedizin, v. 58, p. 460-469, 2019.
Author notes
*victor.balcao@prof.uniso.br**jose.oliveira@prof.uniso.br
Conflict of interest declaration