TREATING ANXIETY AND DEPRESSION OF CANCER SURVIVORS: BEHAVIORAL ACTIVATION VERSUS ACCEPTANCE AND COMMITMENT THERAPY.
Tratamiento de ansiedad y depresión en supervivientes de cáncer: activación conductual versus terapia de aceptación.
TREATING ANXIETY AND DEPRESSION OF CANCER SURVIVORS: BEHAVIORAL ACTIVATION VERSUS ACCEPTANCE AND COMMITMENT THERAPY.
Psicothema, vol. 30, no. 1, pp. 14-20, 2018
Colegio Oficial de Psicólogos del Principado de Asturias
Received: 02 October 2017
Accepted: 27 December 2017
Abstract: Background: Behavioral activation (BA) and acceptance and commitment therapy (ACT) are considered particularly useful treatments when dealing with emotional problems of cancer survivors. The efficacy of these two treatments, applied on a group basis, were evaluated and compared. Method: An analysis was carried out of pre-post treatment changes in the emotional state and patterns of activation/avoidance of 52 cancer patients, with anxiety and/or depression, randomly assigned to three groups (BA/ ACT/waiting list control). Results: Both therapies were superior to no treatment in all the variables evaluated. Significant differences were found between the two treatments in favor of ACT in social impairment and avoidance/rumination. Conclusions: BA and ACT, applied on a group basis, are efficacious in the treatment of those emotional difficulties most prevalent in cancer survivors. Results suggest that activation and avoidance are the mechanisms responsible for the changes.
Keywords: Randomized controlled trial, depression, anxiety, psychotherapy.
Resumen: Antecedentes: la activación conductual (AC) y la terapia de aceptación y compromiso (ACT) se plantean como tratamientos especialmente útiles para los problemas emocionales de los supervivientes de cáncer. Se evaluó y comparó la eficacia de ambas terapias aplicadas en formato grupal. Método: se analizaron los cambios pre-post tratamiento en el estado emocional y los patrones de activación/evitación de 52 supervivientes de cáncer con ansiedad y/o depresión que se asignaron aleatoriamente a tres grupos (AC/ACT/control de lista de espera). Resultados: ambas terapias fueron superiores al no tratamiento en todas las variables evaluadas. Se encontraron diferencias significativas entre tratamientos a favor de la ACT en deterioro social y evitación/rumia. Conclusiones: la AC y la ACT, en formato grupal, son eficaces para el tratamiento de las dificultades emocionales más prevalentes en supervivientes de cáncer. Los resultados apuntan a la activación y la evitación como mecanismos responsables de los cambios.
Palabras clave: ensayo controlado aleatorizado, depresión, ansiedad, psicoterapia.
Different studies have shown the high prevalence of emotional difficulties in cancer survivors. Anxiety and depression are the most frequent problems (Kuhnt et al., 2016), with a prevalence of 17.9% and 11.6% respectively, both superior to those found in healthy control groups (Mitchell, Ferguson, Gill, Paul, & Symonds, 2013). In order to understand this high prevalence, it is important to bear in mind the implications of cancer.
The disease and diagnosis mark the beginning of a process which will involve many adverse experiences. The disease, the tests and medical treatments frequently include unpleasant and impeding experiences such as pain and fatigue. Furthermore, the disease requires frequent visits to the hospital for check-ups and treatment. These experiences and conditions frequently lead to patients reducing their involvement in relevant and/or pleasant activities. In some cases, health workers and those close to the patient also encourage this reduction in involvement, or even abandonment of activities, as a means to enabling the patient to better care for his/her health.
The abandonment of tasks and responsibilities may produce relief in the short term. However, distancing oneself from day-to- day activities reduces the chances of maintaining contact with the rewarding situations and valuable conditions of life. In particular, changes in relationships with friends and in leisure have been related to a depressed state of mind, lower quality of life, tiredness, insomnia and pain. When treatment finishes, although a gradual recovery of the majority of day-to-day activities is observed, this is always smaller amongst patients with a greater degree of depression (Cataldo & Brodsky, 2013).
Having finished their oncological treatment, patients frequently suffer from physical complaints and tiredness, attention and concentration difficulties and have to adapt to living with physical changes. These after-effects, some permanent, can interfere with the maintenance or recovery of roles important to them (Fernández et al., 2011).
When faced with these problems and limitations, together with the experience of receiving the diagnosis and treatment of cancer, patients frequently experience unpleasant thoughts, feelings and memories. A common reaction to these experiences, encouraged and reinforced by the cultural context, is to try to avoid them. However, attempting to control thoughts and unpleasant emotions is associated with emotional problems (Berrocal, Rivas, Venditti, & Bernini, 2016; Nieto & Barraca, 2017). These attempts not only do not achieve the desired relief but generate more discomfort, contribute to perpetuating it, and limit involvement in important areas of life. Consequently, behavioral inhibition, which reduces opportunities to maintain contact with the rewarding and valuable situations of life, together with the increase in adverse experiences related to the disease and its treatment and the strategy of avoiding such experiences may be related to the emotional problems of oncological patients.
Psychological intervention, particularly cognitive behavioral therapy, has been shown to achieve positive results in the treatment of oncological patients. However, its effectiveness has only been proven with regard to short term benefits in specific areas. The majority of studies have used supportive expressive or cognitive behavioral therapy approaches. This fact may have been responsible for the limited results. It is believed that interventions that are holistic and context-based, as in the case of the third- generation therapies, rather than symptom-based, may achieve better results since they adapt better to the needs of oncological patients (Hulbert-Williams, Storey, & Wilson, 2015).
Of the third-generation therapies, behavioral activation(BA) and acceptance and commitment therapy (ACT), due to the emphasis they place on eliminating avoidance and encouraging activation (Hulbert-Williams et al., 2015; Kanter, Baruch, & Gaynor, 2006), may be particularly useful in the treatment of emotional difficulties in cancer survivors. The goals of these therapies comply with the previously described situation, characterized by the avoidance of unpleasant private events related to the disease and a reduction in involvement in relevant activities.
Both therapies have shown good results in the psychological treatment of cancer survivors. BA has been shown to be useful both in the prevention and treatment of emotional problems in studies which were rigorous in terms of their methodology (González, Fernández, Padierna, Besteiro, & Pérez, in press). Similarly, all the studies using ACT, despite the heterogeneity of the experiment designs, show improvements in the emotional state and quality of life of the participants (e.g., Rost, Wilson, Buchanan, Hildebrant, & Mutch, 2012).
The aim of the present study is to analyze the efficacy of BA and ACT, applied on a group basis, in the treatment of emotional difficulties in cancer survivors. The importance of carrying out such a study lies, firstly, in the fact that only ACT has been studied in cancer survivors on a group basis, and only in a limited number of studies, and secondly, as far as we are aware, it has never been compared to BA. The first aspect is important with regard to improving the efficiency of the psychological treatments. The second is particularly relevant with regard to the objective of identifying responsible factors for the clinical change.
Method
Participants
The sample was composed of 52 subjects of between 34 and 62 years of age (M=51.66; SD=6.76). The 92.3% were women and 7.7% men, 88.2% had received a diagnosis of breast cancer and 11.8% had been diagnosed with other types of cancer. The inclusion criteria for the study were to be between 18 and 65 years of age, to have finished oncological treatment with surgery, chemotherapy and/or radiotherapy for any type of malignant tumor, to currently be free of any type of oncological disease and to suffer clinically significant emotional distress (score≥8 in at least one of the subscales of the Hospital Anxiety and Depression Scale). The exclusion criteria were to be receiving another type of psychological therapy, to suffer physical deterioration which might hinder participation in the therapy, cognitive deterioration and when participation in group therapy was not considered to be appropriate.
Instruments
Hospital Anxiety and Depression Scale (HADS; Zigmond & Snaith, 1983) is a 14-item scale with 2 subscales, Anxiety and Depression. The total HADS score ranges from 0 to 42 while the subscales range from 0 to 21. In depression and anxiety subscales, scores of 8-10 indicate probable and scores over 10 indicate clinical cases. In psycho-oncology, the HADS score has been proven to be an accurate instrument in identifying cancer patients with depression (Katz, Kopek, Waldron, Devins, & Tomlinson, 2004) and anxiety (Walker et al., 2007).
Environmental Reward Observation Scale (EROS; Armento & Hopko, 2007). A self-administered questionnaire which supplies information regarding the quantity and availability of reinforcement received from the patient’s environment. It consists of 10 items, answered using a 4-option Likert scale. Higher scores indicate a greater quantity and availability of reinforcement. The Spanish adaptation was used (Barraca & Pérez-Álvarez, 2010) whose reliability and validity has been shown.
Acceptance and Action Questionnaire-II (AAQ-II; Bond et al., 2011). This is a self-rating questionnaire designed to measure experiential avoidance and psychological inflexibility. It consists of 7 items, answered using a 7-point Likert scale. High scores indicate a greater degree of experiential avoidance and psychological inflexibility. The Spanish translation showed good internal consistency and scores showed significant relationships with general scales measuring psychopathological state and quality of life (Ruiz, Langer, Luciano, Cangas, & Beltrán, 2013).
Behavioral Activation for Depression Scale (BADS; Kanter, Mulick, Busch, Berlin, & Martell, 2007). Consists of 25 items measuring four dimensions: Activation, Avoidance/Rumination, Work/School Impairment and Social Impairment. A 7-point Likert scale is used. The scale provides scores for each of the dimensions and also a total score. High scores in Activation and in the total score show a higher level of activation, whilst higher scores in the other dimensions indicate a greater degree of impairment. The Spanish adaptation (Barraca, Pérez-Álvarez, & Lozano, 2011) proved to be valid and had internal consistency. Factor analysis confirmed the four dimensions of the original instrument.
Procedure
In order to obtain participants for the study, Primary Care and Oncology healthcare professionals, associations of cancer patients and the general population were informed about the study. Those people who contacted the research team interested in participating in the study were assessed using a clinical interview and standardized self-report instruments. All participants signed a written consent.
Those participants who fulfilled the inclusion criteria were assigned at random to two experimental groups and a waiting list control group. The people assigned to the experimental groups participated in one of the therapies being studied (BA/ACT), which were applied on a group basis (maximum 6 people) over 12 weekly sessions of 90 minutes. The interventions were led by two clinical psychologists, each with relevant training and experience in both of the therapies being studied. Supervision sessions were held in order to ensure adhesion to therapeutic protocols. Following completion of the intervention, the evaluation instruments were again applied to all participants. Details of the study process are shown in Figure 1.

Figure 1.
Study flow diagram
Both therapies were applied following protocols designed ad hoc for the study. These protocols were based on reference manuals for each of the therapies (Hayes, Strosahl, & Wilson, 2014; Hopko & Lejuez, 2007; Martell, Dimidjian, & Herman-Dunn, 2013). The sessions were structured as follows: review of work done between sessions, work on those aspects programmed for the session, planning of work for the following week. The objectives and procedures of each of the interventions are described below.
The BA was aimed at reestablishing relevant day-to-day routines and activities, increasing rewarding activities, eliminating illness behavior and modifying patterns of experiential avoidance. The targets and tasks for each case and in each session of the intervention were determined using functional behavioral analysis. This allowed participants to learn to observe the relationship between what they did, felt and thought and what happened around them. The principal techniques employed were self-observation and self-report, rehearsal and behavior modeling, elaboration of activity hierarchies, behavior programming, contingency management and use of metaphors and experiential exercises to facilitate acceptance of and distancing from emotions and thoughts. When necessary, problem solving and training in social skills was also used.
The objective of the ACT was to invert all the processes involved in psychological inflexibility. In the first sessions, the main topics dealt with were experiential avoidance, inflexible attention, attachment to the conceptualized self and cognitive fusion. As from the eighth session, work focused mainly on the connection with values and commitment to rewarding actions. The techniques used most widely throughout the therapy to achieve the different objectives were metaphors and experiential exercises. With a view to promoting commitment to rewarding experiences, the following techniques were used: rehearsal and behavior modeling, behavioral programming, contingency management and, when necessary, training in how to act in order to achieve relevant objectives.
The study was conducted in accordance with codes of ethics and conduct specified by the American Psychologist Association and was approved by the Research Ethics Committee of the Principality of Asturias, Spain (Ref. 45/14).
Data analysis
In order to compare groups regarding sociodemographic and disease-related variables, the chi-square test was used for the categorical variables (sex, marital status, profession, work situation, level of studies, location of the tumor, oncological treatment received) and the Kruskal-Wallis test for quantitative variables with important asymmetry (age, number of children, number of people in the household). The equivalence between the groups for the pre-measures of all the dependent variables was tested using one-way ANOVAs, followed by a Scheffé test (or Dunnett’s T3 in the case of heteroscedasticity) for post-hoc comparisons.
In order to compare pre- and post-treatment measures, repeated-measures ANOVAs were used, taking the group as the inter-factor. In the case of instruments made up of various subscales, repeated-measures multivariate analyses were carried out previously (Wilks’ lambda) taking the subscales as different dependent variables. In order to carry out the ANOVAs, it was first confirmed that all the dependent variables had normal (Shapiro- Wilk’s test) or approximately normal distribution (asymmetry and kurtosis indexes less than 1). The effect size was quantified by partial eta2.
Results
Before starting the treatment, there were no differences between the groups with regard to sociodemographic and disease-related variables. In the pre-treatment measures of the dependent variables, significant differences were found between the groups in the AAQ- II (F2,48=5.03, p=.010) and in the Work/School Impairment subscale of the BADS (F2,49=4.83, p=.012). In both cases, the scores of the ACT group were significantly higher than those of the control group. The levels of significance were p=.020 in the Work/ School Impairment subscale and p=.012 in the AAQ-II.
The mean scores of the groups in the pre- and post-treatment measures of the dependent variables are shown in Table 1. All variables had normal or approximately normal distribution.
The results of the univariate and multivariate analyses to compare the pre- and post-measures of the groups are shown below. In all the analyses, the multivariate homoscedasticity (Box’s M) and the normal distribution of the residues were tested. The first criterion was not fulfilled in the HADS, AAQ-II and EROS. The distribution of the standardized residues conformed to the normal curve in all variables except the Work/School Impairment subscale of the BADS (K-S test).
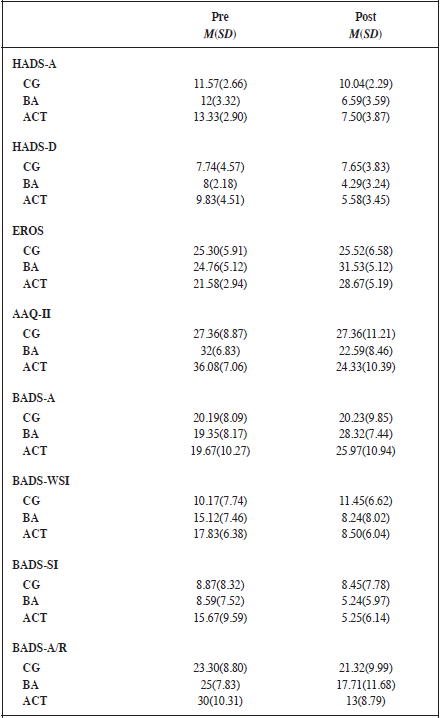
Note: CG: Control Group. BA: Behavioral Activation. ACT: Acceptance and Commitment Therapy. Pre: Pretreatment. Post: Posttreatment. HADS-A: Anxiety subscale of HADS. HADS-D: Depression subscale of HADS. EROS: Environmental Reward Observation Scale. AAQ-II: Acceptance and Action Questionnaire–II. Dimensions BADS: A: Activation. WSI: Work/School Impairment. SI: Social Impairment. A/R: Avoidance/Rumination
HADS. The intra-factor effect was significant when the two scales were considered jointly (F2,48=47.25, p<.001, ηP2=.663) as was its interaction with the group (F4,98=5.33, p=.001, ηP2=.182). When each scale was considered separately, interaction with the group was significant, both in Anxiety (F2,49= 11.62, p<.001, ηP2=.322) and Depression scales (F2,49=.98, p=.005, ηP2=.196). In both cases, the differences between pre- and post-measures were significantly larger for the experimental groups than for the control group. There were no differences between the slopes of the experimental groups.
EROS. The effect of the intra-factor was significant (F1,48=29.09, p<.001, ηP2=.377) as was its interaction with the group (F2,48=7.16, p=.002, ηP2=.230). The increase in the scores from the pre- to the post- only occurred in the experimental groups and to a similar degree in both.
AAQ-II. The interaction between the intra-factor and the group was significant (F2,48=8.21, p=.001; ηP2=.255). There were no pre-post differences in the control group whilst a similar decrease was observed in the two experimental groups.
BADS. Pre-post differences were only observed in the experimental groups. When the four scales were considered jointly, the multivariate contrasts for the intra-factor and its interaction with the group were significant (F8,92=3.56, p=.001; ηP2=.24). When each scale was considered separately, interaction of the intra- factor with the group was significant in Activation (F2,48=4.065, p=.002; ηP2=.145), Work/School Impairment (F2,48=8.85, p=.001; ηP2=.269), Social Impairment (F2,48=6.70, p=.003; ηP2=.218) and Avoidance/Rumination (F2,48=7.135, p=.002; ηp2=.229). When the two experimental groups were compared with each other, there was significant interaction with the intra-factor in the variables of Social Impairment (F1,27=5.38, p=.028; ηp2=.166) and Avoidance/Rumination (F1,27=4.14, p=.050). In both cases, the pre-post decrease was significantly larger in the ACT group.
Discussion
The objective of this study was to analyse the efficacy of BA and ACT, applied on a group basis, in the treatment of emotional difficulties in cancer survivors. The design of the study, the psychometric guarantees of the evaluation instruments and safeguards of the statistical tests used guarantee the validity of the results obtained.
The sample consisted of survivors of different types of cancer. However, the fact that the participants had received different oncological diagnoses and different treatments certainly does not mean that the results cannot be generalized. It must be remembered that, as survivors, they all shared the same clinical condition, that is, they were all free of oncological disease at the time of the study. Furthermore, their emotional distress was potentially related to the same condition, that of having received a diagnosis of, and treatment for, cancer. Samples of patients with different types of cancer are common in other studies investigating the efficacy of the same therapies studied here (Arch & Mitchell, 2016; Hopko et al., 2008). It is true that the fact that a high percentage of the sample had suffered from breast cancer meant a higher presence of women in the study and this fact may have had an influence on the emotional state of the sample. It is known that emotional disorders are more prevalent amongst women and also that women are more willing than men to seek professional help for such disorders (Steel et al., 2014). Although this, together with the high prevalence of breast cancer, would explain the unequal composition of the sample in terms of gender, this condition must be taken into account when generalizing the results.
In general, the participants showed more anxiety than depression in the pre-treatment. This result coincides with those of numerous studies, which show a greater prevalence of anxiety than depression in cancer survivors (Mitchell et al., 2013).
In the pre-treatment, differences were found between the ACT group and the control group in the AAQ-II and in the Work/ School Impairment subscale of the BADS. Despite the fact that the participants in the ACT group showed a higher degree of experiential avoidance and greater work/school impairment, no differences were found between the groups in the measures of emotional distress in the pre-treatment. Consequently, the initial differences do not affect the value of the results obtained regarding the post-treatment emotional changes observed. It is, however, important to bear in mind the differences in the pattern of psychological inflexibility when evaluating the results, firstly as a mediator in the emotional distress of the participants in the study and, secondly, as a modulator of the effects of each of the interventions. On this point, it should be remembered that both interventions aim to modify the pattern of psychological inflexibility, although each uses different strategies.
The AC and the ACT were superior to no treatment in all the variables studied. The subjects who participated in the therapies showed a reduction in anxiety and depression (HADS), an increase in activation (EROS, BADS: Activation, Work/School Impairment, Social Impairment) and a reduction in avoidance (AAQ-II; BADS: Avoidance/Rumination). These results demonstrate that the therapies provoked the desired changes. The fact that both therapies, aimed at increasing activation and reducing avoidance, achieved improvements, not only in these patterns but also in the emotional distress of the participants, supports the idea that both patterns play a key role in the onset, maintenance and treatment of emotional problems in this population. Previous studies of BA (Fernández et al., in press; 2011) and of ACT (Arch & Mitchell, 2016; Rost et al., 2012) found similar changes when treating oncological patients, reporting changes in activation and avoidance as well as an improvement in emotional state and quality of life.
Regarding the comparison between the experimental groups, significant differences were found in favour of ACT in the Social Impairment and Avoidance/Rumination variables (BADS). According to these results, ACT appears to be more efficacious than BA. However, it is important to bear in mind that, although the differences were not statistically significant, in the pre-treatment the participants in the ACT group showed greater affectation than the participants in the BA group in both aspects. What is more, the ACT group showed greater Work/School Impairment (BADS) and greater avoidance (AAQ-II) than the control group in the pre-treatment. In this case the differences were significant. The fact that the participants in the ACT group were worse in the pre- treatment could have facilitated their improvement. In a previous study in which BA was applied (Fernández et al., in press; 2011), those people with greater emotional difficulties also benefited more from the treatment. Furthermore, studies typically show that the patients that improve most are those with a clinically diagnosable disorder rather than those with more generic distress. In the other variables, the two therapies proved to be equally efficacious.
Both therapies had the same objectives: to reduce inflexible avoidance of thoughts, feeling and memories related to the oncological process and to encourage involvement in rewarding activities, each therapy following a different procedure. In the BA, the recuperation of rewarding activities implies abandoning of avoidance behaviour. Consequently, an integrated approach was taken throughout the therapy when working on the two conditions. The intervention related to avoidance and activation was always determined by a functional analysis of the participants’ difficulties. However, the ACT focused primarily on reducing experiential avoidance and most of the therapy time was dedicated to this objective. Only later in the therapy was attention paid to activation and commitment in line with the subject’s values. Furthermore, in the ACT, functional analysis did not play as important a role as it did in the BA.
The two therapies studied were both superior to no treatment. This appears to indicate that the efficacy of the treatment depends, not so much on how avoidance and activation is treated, but rather on the ability of the therapy used to provoke a significant change in the two conditions. In light of the differences found between the experimental groups, the question arises as to whether ACT is more efficacious than BA in the treatment of cancer survivors with emotional problems in general, or, more specifically, in those whose main problem is anxiety. In the study carried out by González- Fernández et al. (2017), avoidance was related both to anxiety and depression whilst low degrees of activation were associated more specifically with depression. The participants in this study showed a greater presence of anxiety than of depression. It is, therefore, possible that the greater efficacy of ACT was related to the greater emphasis of this therapy on reducing avoidance. Similarly, BA may be more efficacious than ACT in the treatment of survivors with depression.
Despite the value of the results of the present study, we believe it is necessary to analyse the relative efficacy of the two therapies in greater depth. To do so, it may be useful to include the following: follow-up data, assessment using other procedures, standardized self-report instruments, studies involving larger samples and an analysis of the specific difficulties of the patients involved in each of the therapies. Furthermore, randomized controlled trials comparing the efficacy of the therapies with psychological- placebo interventions and with other efficacious therapies would be of particular interest.
The results of this study show, firstly, the efficacy of BA and ACT, applied on a group basis, in the treatment of the most prevalent emotional problems in cancer survivors and, secondly, the key role played by avoidance and activation in the onset, maintenance and treatment of these problems. We believe these results to be important due to their relevance for clinical practice. They can contribute to a more efficient application of psychological treatments and also provide a greater insight into the active principles of those treatments. This latter aspect is of fundamental importance, since a knowledge of these principals is what, ultimately, will make it possible to progress in the implementation of treatments which adapt to and resolve the emotional problems of each individual.
Acknowledgements
This study has been financed by the Ficyt (Ref. BP13141) and by the Ministry of Economy and Competitiveness of the Spanish Government (Projects I+D+I. Ref. PSI2014-55594-P).
References
Arch, J.J., & Mitchell, J.L. (2016). An Acceptance and Commitment Therapy (ACT) group intervention for cancer survivors experiencing anxiety at re-entry. Psycho-Oncology, 25(5), 610-615. http://dx.doi.org/10.1002/pon.3890
Armento, M.E., & Hopko, D.R. (2007). The Environmental Reward Observation Scale (EROS): Development, validity, & reliability. Behavior Therapy, 38(2), 107-119. http://dx.doi.org/10.1016/j.beth.2006.05.003
Barraca, J., & Pérez-Álvarez, M. (2010). Adaptación española del Environmental Reward Observation Scale (EROS) [Spanish adaptation of the Environmental Reward Observation Scale (EROS)]. Ansiedad y Estrés, 16(1), 95-107.
Barraca, J., Pérez-Álvarez, M., & Lozano, J.H. (2011). Avoidance and Activation as Keys to Depression: Adaptation of the Behavioral Activation for Depression Scale in a Spanish Sample. The Spanish Journal of Psychology, 14(2), 998-1009. http://dx.doi.org/10.5209/rev_SJOP.2011.v14.n2.45
Berrocal, C., Rivas, T., Venditti, F., & Bernini, O. (2016). On the contribution of psychological flexibility to predict adjustment to breast cancer. Psicothema, 28(3), 266-271. doi:10.7334/psicothema2015.271
Bond, F.W., Hayes, S.C., Baer, R.A., Carpenter, K.M., Guenole, N., Orcutt, H.K., et al. (2011). Preliminary psychometric properties of the Acceptance and Action Questionnaire - II: A revised measure of psychological inflexibility and experiential avoidance. Behavior Therapy, 42(4), 676-688. http://dx.doi.org/10.1016/j.beth.2011.03.007
Cataldo, J.K., & Brodsky, J.L. (2013). Lung cancer stigma, anxiety, depression and symptom severity. Oncology, 85(1), 33-40. http://dx.doi.org/10.1159/000350834
Fernández, C., Villoria, E., Fernández, P., González, S., & Pérez M. (in press). Effects of Behavioral Activation on the quality of life and emotional state of lung cancer and breast cancer patients during chemotherapy treatment. Behavior Modification.
Fernández, C., Villoria, E., Amigo, I., Padierna, C., Gracia, J.M., & Fernández, R. (2011). Terapia de activación conductual en pacientes con cáncer [Behavioral activation treatment for cancer patients]. Anales de Psicología, 27(2), 278-291.
González, S., Fernández, C., Padierna, C., Besteiro, J.L., & Pérez, M. (in press). Activación conductual en cáncer: revisión de tratamientos y evidencias [Behavioral activation in cancer: Review of treatments and evidences]. Revista Argentina de Clínica Psicológica.
González-Fernández, S., Fernández-Rodríguez, C., Mota-Alonso, M.J., García- Teijido, P., Pedrosa, I., & Pérez-Álvarez, M. (2017). Emotional state and psychological flexibility in breast cancer survivors. European Journal of Oncology Nursing, 30, 75-83. http://dx.doi.org/10.1016/j.ejon.2017.08.006
Hayes, S.C., Strosahl, K., & Wilson K.G. (2014). Terapia de aceptación y compromiso. Proceso y práctica del cambio consciente (Mindfulness) [Acceptance and Commitment Therapy. The Process and Practice of Mindful Change]. Bilbao: Desclée de Brouwer.
Hopko, D.R., & Lejuez, C.W. (2007). A Cancer Patient’s Guide to Overcoming Depression & Anxiety. Getting Through Treatment & Getting Back to Your Life. Oakland: New Harbinger Publications.
Hopko, D.R., Bell, J.L., Armento, M., Robertson, S., Mullane, C., Wolf, N., et al. (2008). Cognitive-behavior therapy for depressed cancer patients in a medical care setting. Behavior Therapy, 39(2), 126-136. http://dx.doi.org/10.1016/j.beth.2007.05.007
Hulbert-Williams, N.J., Storey, L., & Wilson, K.G. (2015). Psychological interventions for patients with cancer: psychological flexibility and the potential utility of Acceptance and Commitment Therapy. European Journal of Cancer Care, 24(1), 15-27. http://dx.doi.org/10.1111/ecc.12223
Kanter, J.W., Baruch, D.E., & Gaynor, S. T. (2006). Acceptance and Commitment Therapy and Behavioral Activation for the Treatment of Depression: Description and Comparison. The Behavior Analyst, 29(2), 161-185. http://dx.doi.org/10.1007/BF03392129
Kanter, J.W., Mulick, P.S., Busch, A.M., Berlin, K.S., & Martell, C.R. (2007). The Behavioral Activation for Depression Scale (BADS): Psychometric properties and factor structure. Journal of Psychopathology and Behavioral Assessment, 29(3), 191-202. http://dx.doi.org/10.1007/s10862-006-9038-5
Katz, M.R., Kopek, N., Waldron, J., Devins, G.M., & Tomlinson, G. (2004). Screening for depression in head and neck cancer. Psychooncology, 13(4), 269-280. http://dx.doi.org/10.1002/pon.734
Kuhnt, S., Brähler, E., Faller, H., Härter, M., Keller, M., Schulz, H., et al. (2016). Twelve-Month and Lifetime Prevalence of Mental Disorders in Cancer Patients. Psychotherapy and Psychosomatics, 85(5), 289-296. http://dx.doi.org/10.1159/000446991
Martell, C.R., Dimidjian, S., & Herman-Dunn, R. (2013). Activación conductual para la depresión. Una guía clínica [Behavioral activation for depression: A clinician’s guide]. Bilbao: Desclée de Brouwer.
Mitchell, A.J., Ferguson, D.W., Gill, J., Paul, J., & Symonds, P. (2013). Depression and anxiety in long-term cancer survivors compared with spouses and healthy control: A systematic review and meta-analysis. The Lancet Oncology, 14(8), 721-732. http://dx.doi.org/10.1016/S1470-2045(13)70244-4
Nieto, E., & Barraca, J. (2017). Behavioral activation versus cognitive restructuring to reduce automatic negative thoughts in anxiety generating situations. Psicothema, 29(2), 172-177. doi:10.7334/psicothema2016.325
Rost, A.D., Wilson, K., Buchanan, E., Hildebrandt, M.J., & Mutch, D. (2012). Improving Psychological Adjustment Among Late-Stage Ovarian Cancer Patients: Examining The Role of Avoidance in Treatment. Cognitive and Behavioral Practice, 19(4), 508-517. http://dx.doi.org/10.1016/j.cbpra.2012.01.003
Ruiz, F.J., Langer, A.I., Luciano, C., Cangas, A.J., & Beltrán, I. (2013). Measuring experiential avoidance and psychological inflexibility: The Spanish version of the Acceptance and Action Questionnaire - II. Psicothema, 25(1), 123-129. doi:10.7334/psicothema2011.239
Steel, Z., Marnane, C., Iranpour, C., Chey, T., Jackson, J.W., Patel, V., et al. (2014). The global prevalence of common mental disorders: A systematic review and meta-analysis 1980-2013. International Journal of Epidemiology, 43(2), 476-493. http://dx.doi.org/10.1093/ije/dyu038
Walker, J., Postma, K., McHugh, G.S., Rush, R., Coyle, B., Strong, V., et al. (2007). Performance of the Hospital Anxiety and Depression Scale as a screening tool for major depressive disorder in cancer patients. Journal of Psychosomatic Research, 63(1), 83-91. http://dx.doi.org/10.1016/j.jpsychores.2007.01.009
Zigmond, A.S., & Snaith, R.P. (1983). The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica, 67(6), 361-370. http://dx.doi.org/10.1111/j.1600-0447.1983.tb09716.x
Notes