HEALTH-RELATED QUALITY OF LIFE AMONG SMOKING RELAPSERS.
La calidad de vida relacionada con la salud en fumadores que han recaído.
HEALTH-RELATED QUALITY OF LIFE AMONG SMOKING RELAPSERS.
Psicothema, vol. 30, no. 1, pp. 27-32, 2018
Colegio Oficial de Psicólogos del Principado de Asturias
Received: 15 February 2017
Accepted: 26 July 2017
Abstract: Background: Previous studies have shown that smoking is associated with health-related quality of life (HRQoL) impairment. In order to evaluate HRQoL in a sample of Spanish relapsers, a cross-sectional study was conducted. Method: The sample was made up of 775 smokers who had relapsed after a period of abstinence. HRQoL was evaluated using the Euro-Qol questionnaire (EQ-5D); through the descriptive profile, the EQ-5D index and the visual analogue scale (EQ-VAS). Results: Higher nicotine dependence was related to worse HRQL. According to the EQ-VAS, higher daily cigarette consumption and more years smoking were related to worse perceived health. In the EQ-5D those who had quit smoking in the previous year perceived worse health. Mobility and anxiety / depression are the dimensions affected by smoking. Those who are more nicotine dependent (OR = 2.29) and have been smoking for longer (OR = 4.12) are more likely to have mobility problems; and those who are nicotine dependent (OR = 1.85) and relapsed more than a year ago (OR = 0.63), are more likely to experience anxiety/depression. Conclusions: Nicotine dependence demonstrated a determining effect on HRQOL deterioration in smokers who have relapsed.
Keywords: Health-related quality of life (HRQoL), smoking, relapse.
Resumen: Antecedentes: estudios previos demuestran que fumar produce un deterioro de la calidad de vida relacionada con la salud (CVRS). Para evaluar la CVRS en fumadores españoles que han recaído se realizó un estudio transversal. Método: la muestra estaba formada por 775 fumadores que habían recaído tras un período de abstinencia. La CVRS se evaluó mediante el cuestionario Euro-Qol 5D (EQ-5D), utilizando el perfil descriptivo, el índice EQ-5D y la escala visual-analógica (EQ-EVA). Resultados: a mayor dependencia de la nicotina peor CVRS. En la EQ- EVA, a mayor consumo diario de cigarrillos y más años consumiendo, peor estado de salud percibido. En el EQ-5D los que dejaron de fumar en el último año son los que perciben peor estado de salud. Movilidad y ansiedad/depresión son las dimensiones afectadas en esta muestra de fumadores que han recaído. Es más probable que tengan problemas en movilidad los que tienen dependencia (OR = 2,29) y llevan más años fumando (OR = 4,12), y es más probable que presenten ansiedad/depresión los dependientes (OR = 1,85) y los que recayeron hace más de un año (OR = 0,63). Conclusiones: la dependencia de la nicotina mostró un efecto determinante en el deterioro de la CVRS en fumadores que han recaído.
Palabras clave: calidad de vida relacionada con la salud (CVRS), fumar, recaída.
Smoking is the most significant avoidable cause of morbidity, disability, and premature mortality in developed countries, so reduction of cigarette smoking continues to be one of the highest public health priorities (American Cancer Society, 2016; U. S. Department of Health and Human Services [USDHHS], 2014). Despite the serious health consequences, and the fact that the majority of people know the risks, smoking cessation is difficult to achieve, as is continuous abstinence for the majority of those who try to give up the habit (Brandon, Vidrine, & Litvin, 2007; Hughes, Keely, & Naud, 2004; Piasecki, 2006). Therefore, as also occurs in other addictive behaviours, a large number of those who achieve abstinence end up relapsing quite soon after quitting (Hajek, Stead, West, Jarvis, & Lancaster, 2013). Although most relapses occur during the first month after quitting, after this period, their incidence decreases but they never cease to occur (Piñeiro & Becoña, 2013), even after several years (Míguez & Becoña, 2008). This implies that most smokers will require several attempts to quit before consolidating their abstinence (Brandon et al., 2007).
Several studies have pointed out the multiple effects of tobacco use on health, as well as the benefits of smoking cessation (Centers for Disease Control and Prevention, 2008; Mons et al., 2015; USDHHS, 2014). In contrast, knowledge about how smoking affects other aspects of health status like health-related quality of life (HRQoL), a relevant measure to study the health of the population (Herdman, 2000), is scarce.
Despite the fact that a reduction in HRQoL among smokers has been found in different studies across populations of diverse socioeconomic and cultural groups (e.g., Becoña et al., 2013; De Miguel et al., 2010; Mulder, Tijhuis, Smit, & Kromhout, 2001; Sarna, Bialous, Cooley, Jun, & Feskanich, 2008; Vogl, Wenig, Leidl, & Pokhrel, 2012), findings across the studies are inconsistent. Whereas some studies have found strong associations for general health and/or mental dimensions (Becoña et al., 2013; Guimaraes et al., 2011; Mulder et al., 2001; Schmitz, Kruse, & Kugler, 2003); no differences in HRQoL between smokers and non-smokers has also been observed (Bellido-Casado et al., 2004; Funahashi et al., 2011). The different selection criteria and sample characteristics, as well as the instruments used to assess quality of life, could be partly responsible for these differences.
Moreover, the effect of tobacco on smokers’ HRQoL may vary as a function of different smoking-related variables (e. g., number of cigarettes smoked, nicotine dependence). For instance, heavy smokers show lower HRQoL scores (Mulder et al., 2001; Sarna et al., 2008; Wilson, Chittleborough, Kirke, Grant, & Ruffin, 2004). Davila et al. (2011) and Schmitz et al. (2003) found that dependent smokers reported poorer quality of life than non-dependent smokers. Other variables studied to a lesser degree are age of regular smoking initiation, age at which smokers quit smoking, stages of change, and quit attempts. Bass, Wilson, and Griffith (2004) found that smokers who initiate smoking before the age of 15 have lower HRQoL, and Gasperini et al. (2016) pointed out that a higher age at which smokers quit smoking is associated with lower scores in HRQoL. Grau, Font-Mayolas, Gras, Suñer, and Noguera (2007) found that smokers who were in stages of change close to quitting smoking indicated worse perceived physical health, and smokers who had no intention of quitting presented worse mental health. Finally, McClave, Dube, Strine, and Mokdad (2009) indicated that certain HRQoL characteristics were worse among smokers who unsuccessfully attempted to quit. They also found better HRQoL among former smokers than among smokers who did not made quit attempts.Therefore, studies indicate than non-smokers have better HRQoL than smokers, and that former smokers have better HRQoL than people who continued smoking. What has not been evaluated yet is how it affected the HRQoL of smokers who made attempts to quit smoking, achieved abstinence for some time and, finally, relapsed. We considered that this research may involve progress in both research and clinical practice, because relapse is common during the process of giving up smoking, and HRQoL is an important motivational variable to stop smoking.
In view of the above, we carried out the current research to identify HRQoL impairment among a sample of Spanish smokers from the general population who had relapsed in the past 5 years. To our knowledge, this is the first study to examine HRQoL in this population. Therefore, the aim of this study was, firstly, to describe HRQoL in relapsers from general population. Secondly, to identify the variables that are related to HRQoL impairment, both at the general level and in the different dimensions, that is, the profile of the relapsers presenting a worse HRQoL.
Method
Participants
The sample was made up of 775 daily smokers, 363 men (46.8%) and 412 (53.2%) women, from the general Spanish population. Participants were recruited according to the following criteria: (1) having smoked in the last 10 years for at least one year daily and uninterruptedly; (2) smoking at least 10 cigarettes per day; (3) having quit smoking in the last 5 years for at least one month uninterruptedly and having relapsed; and (4) at the time of the assessment, smoking at least one month since the relapse.
Procedure
A cross-sectional study was performed in which data were collected anonymously from 1017 smokers from the general population by means of an ad hoc questionnaire. The questionnaires of 242 participants were eliminated due to incomplete data. Participants were recruited through “snowball” method.
Instruments
A self-administered questionnaire about sociodemographics (age, gender, marital status, education, and employment status) and smoking-related variables was used in this study. Participants answered questions about number of cigarettes smoked per day, number of years smoking, quit attempts in the last 5 years, days without smoking, relapses, stages of change, and nicotine dependence. The degree of motivation to give up smoking was assessed with the Stages of Change Questionnaire (Prochaska, DiClemente, & Norcross, 1992). For the assessment of nicotine dependence, we used the Fagerström Test for Nicotine Dependence (FTND; Heatherton, Kozlowski, Frecker, & Fagerström, 1991; Spanish version of Becoña & Vázquez, 1998), a six-item scale with scores ranging from 0 to 10. A score of 6 or more indicates nicotine dependence.
Data on the HRQoL were obtained using the EuroQoL Group Health Questionnaire (EQ-5D; EuroQoL Group, 1990; Spanish adaptation of Badia, Roset, Montserrat, Herdman, & Segura, 1999). This generic measurement instrument of HRQoL consists of two parts. The first provides descriptive information about five health dimensions: mobility, self-care, usual activities (work, studies, household tasks), pain/discomfort and anxiety/depression. For each dimension, individuals choose the level of severity, among three possibilities, that best reflects their health status on the day they fill in the questionnaire; each health status is assigned a single value (tariff) using a standardized formula anchored on a scale ranging from 0 (being dead) and 1 (full health) (EQ-5D Index).
The second part of the EQ-5D is a Visual Analogue Scale (VAS) ranging from 0 (worst health status imaginable) to 100 (best health status imaginable). Respondents indicate on the scale the point that best represents their global health status on the assessment day. The VAS provides quantitative information about the global health status perceived by the individual, complementary to the descriptive system of the self-assessment of health status by dimensions.
Average completion time of the questionnaires was 10 minutes.
Data analysis
All analyses were conducted with SPSS version 20.0, with a p-value of < .05 considered significant. A descriptive statistics analysis was made of the total sample (N = 775) to analyze the sociodemographic and tobacco consumption characteristics. We used chi-square test to analyze differences between respondent categories in the EQ-5D profile data, and t-tests to analyze the EQ- 5D Index and VAS scores. Cramers’s V coefficients and Cohen’s d were calculated to estimate the effect size.
We used linear regression to analyze the variables that predicted a worse perception of QoL on the EQ VAS and EQ- 5D. Age, number of cigarettes smoked at the evaluation moment, total score in the Fageström test, number of years of consumption, and number of days of abstinence were introduced as independent variables. Moreover, to examine predictors of the presence of problems in each of the five dimensions of the EQ-5D, binary logistic regression analyses with forward stepwise selection were performed. All significant variables in bivariate analyses were introduced as independent variables: age (<50), sex, marital status (with partner / non-partner), education level (university / non-university), work situation number of cigarettes smoked at the evaluation moment (<25), Fageström score (dependent / non- dependent), years of consumption (<25), number of quit attempts within the last year (none / one or more), relapse time (last year / 2 to 5 years), and the other quality of life dimensions (mobility, personal care, daily activities, pain and anxiety / depression).
Results
Sociodemographic and tobacco consumption characteristics
Mean age of the sample is 42 years (SD = 10.83). Of them, 53.2% are women, 58.6% are married or living with a partner, 35.3% have university studies, and the majority (71.2%) are employees.
Participants smoked an average of 15.60 cigarettes /day (SD = 6.49, range 10 -60). They had been smoking an average of 23.85 years (SD = 10.46), 29.9% smoked 20 or more cigarettes (heavy smokers), 16.8% presented nicotine dependence, and 50.2% were in the stage of contemplation.
The average number of days they were abstinent, adding all their attempts, was 238 days (SD = 393.39). Considering the relapse moment, 37.5% had relapsed in the past year, and 62.5% more than one and less than five years ago.
Quality of life, sociodemographic and smoking-related variables
The percentage of individuals who reported some or severe problems on the EQ-5D domains varied: pain and discomfort (28.6%); anxiety and depression (23.7%); usual activity (8.8%); mobility (5.8%); and self-care (0.8%). There were significant differences as a function of age in mobility, χ² (2, 775) = 12.91, p ≤ .005, V = 0.13, with people over 60 having more problems.
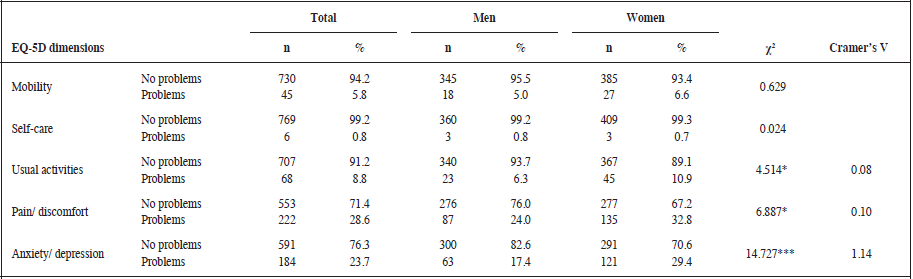
* p ≤ .05;*** p ≤ .001
Regarding gender, women (Table 1) reported more impairment than men in performance of usual activities, and more pain/ discomfort and anxiety/depression.
Regarding EQ-5D Index and VAS (Table 2), the mean EQ-5D index was 0.89 (SD = 0.15) and the mean VAS score was 75.91 (SD = 15.36). Respect to sociodemographic characteristics, significantly lower scores in both index were obtained by gender (women), age (50 years old or more), marital status (divorced/ separated/widowed), education level (without university studies), and work situation (does not work). Respect to smoking related variables, it was found significant differences in nicotine dependence and number of quit attempts within the last year in the mean EQ-5D index. Differences in mean VAS score were significant in number cigarettes per day, nicotine dependence, and years of consumption.
Predictors of quality of life
The linear regressions show that nicotine dependence was the only one predictor of HRQoL, as measured with the EQ-5D index (R2 = 0.022) and the VAS (R2 = 0.059). Higher levels of dependence correspond to worse HRQoL.
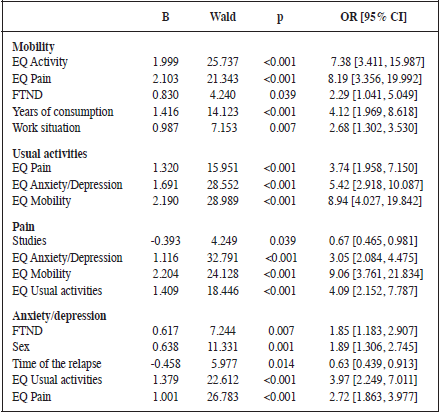
Logistic regression analysis (Table 3) showed that mobility and anxiety/depression are affected by smoking-related variables. Specifically, nicotine dependence (OR = 2.29) and more years of consumption (OR = 4.12) increase the likelihood of having mobility problems. In addition, nicotine dependence (OR = 1.85) and having relapsed more than one year ago (OR = 0.63) increased the likelihood of presenting anxiety/depression.
Discussion
The aim of this study was to investigate self-perceived HRQoL in a sample of smokers with a relapse history. Taking into account the dimensions of the EQ-5D, the results showed that pain/discomfort and anxiety/depression are the dimensions in which participants presented more problems, especially in the case of women.
Taking into account the mean score of the EQ-5D index and the EQ VAS, the sociodemographic profile of the relapsers who present worse HRQoL is characterized as being female, being 50 or older, lower educational level, being divorced/separated or widowed, and not to work. Regarding smoking-related variables, nicotine dependence is the main variable associated with a worse HRQoL. Poor HRQoL on the EQ VAS is also related to more years of consumption and higher daily consumption.
The high percentage of the presence of anxiety/depression coincides with studies that suggest that smokers are more prone to suffer these symptoms than non-smokers (De Lossada & Rejas, 2016; Schmitz et al., 2003). Likewise, it has been well-documented that the prevalence of smoking is extremely high in people who experience anxiety and depression (Dierker, Avenevoli, Stolar, & Merikangas, 2002; Fergusson, Goodwin, & Horwood, 2003).
One of the most important results of this study is that women have worse HRQoL than men, both in general index and in pain/ discomfort and anxiety/depression dimensions. Women that smoke are at higher risk of mortality due to lung cancer than never- smokers or ex-smokers women (Pirie et al., 2013). In addition, women have other specific negative consequences because of smoking, such as reproductive problems, increased risk of cervix cancer and premature menopause (USDHHS, 2014). Moreover, the association between depressive disorders and smoking is more frequent among women (Husky et al., 2008), since they use it for mood management (Fidler & West, 2009) and have higher expectations of negative affect reduction due to smoke (Baker, Piper, McCarthy, Majeskie, & Fiore, 2004). Women may have greater difficulties than men to quit (Perkins & Scott, 2008) and depressive symptoms could play a significant role (Weinberger, Pilver, Desai, Mazure, & McKee, 2013).
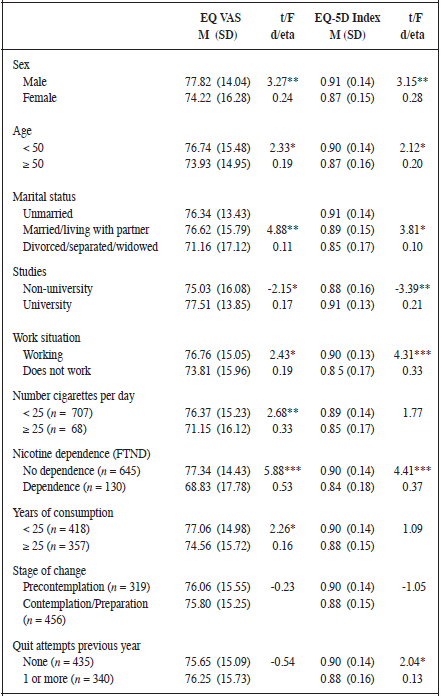
* p ≤ .05; ** p ≤ .01;*** p ≤ .001
Regarding to smoking-related variables, a significant dose- response relationship between cigarette consumption and HRQoL was previously noted (e.g., Mulder et al., 2001; Vogl et al., 2012), with progressively lower scores for smokers with higher consumption. This data may be indicating the existence of a strong dose-response relationship between cigarette consumption and severe diseases (Royal College of Physicians, 2007).
Respect to predictors of HRQoL, mobility and anxiety/ depression are affected by smoking-related variables. Nicotine dependence and more of years of consumption predict impairment in mobility. More smoking years and nicotine dependence are related to physical health deterioration (e.g., fatigue, respiratory problems) (Schmitz et al., 2003) which will significantly affect the person mobility. Otherwise, nicotine dependence and having relapsed more than a year ago increase the likelihood of presenting anxiety / depression. This result is in line with previous studies that indicate the existence of greater nicotine dependence in people with mood problems (Weinberger et al., 2016) and, as in the investigation of Grau et al. (2007), smokers with worse mental health have lower intention of quitting.
Although in this study we have explored the different smoking- related variables that the literature has linked to HRQoL, nicotine dependence remains as the explanatory variable of anxiety/depression in the regression models. In previous studies, nicotine dependence was also related to impairment of the mental component of HRQoL (Becoña et al., 2013; Schmitz et al., 2003). As other authors have informed (Breslau, Killey, & Andreski, 1993; Schmitz et al., 2003), these data could be partially attributed to the rates of psychiatric comorbidity (in particular, affective and anxiety disorders), which are higher in nicotine-dependent smokers than in non-dependent ones.
The variability of QoL measures used (Goldenberg, Danovitch, & IsHak, 2014) become difficult to make quantitative comparisons of the results due to the nature and content of the QoL instrument employed. Precisely, one of the challenges in QoL is the use of instruments with a universal definition of the construct that allows comparing the results at the international and cross-cultural levels (Benítez, 2016).
An important contribution of this study is that it is focused on relapsers. Having suffered relapses can undermine the motivation to quit if it is experienced as a failure. However, relapse can also be seen as a learning experience to increase motivation, based on the notion that “I know that I can manage to quit smoking”. In fact, in our sample, we observed higher motivation to quit among those who have tried to quit smoking more recently because, out of those who were at preparation stage, 63.1% quit smoking in the past year. Previous studies (McClave et al., 2009) show that HRQoL was worse among smokers who unsuccessfully attempted to quit than among smokers who made no attempts to quit.
Limitations in the present study indicate that our results should be interpreted with some caution. First, the cross-sectional design of the study does not allow establishing causal relations. Likewise, the sampling method used limits the representativeness of the sample and, therefore, the generalization of the results. In addition, information on tobacco consumption and HRQoL were based on self-report and not confirmed by collateral informants. As a result, recall bias or tendency to provide socially acceptable responses (i.e., underestimation of consumption) is a potential limitation. Furthermore, no pre-relapse assessments were carried out, which does not allow us to know how relapses affected HRQoL.
Despite these limitations, the strengths of this study are the large sample size of relapsers. Moreover, few studies have examined the association between smoking and HRQoL by means of the EQ-5D scores and, to our knowledge, this is the first one that evaluates impairment of HRQoL in relapsers, providing information both at a global level and by dimensions.
In conclusion, the present study contributes to improving knowledge about association between smoking and HRQoL. Taking into account that the average smoker must make several quit attempts before achieving long-term abstinence (Hughes et al., 2004), more investigations are required about the impact of relapses. Future studies should provide comparative data on HRQoL among relapsers, smokers who unsuccessfully attempted to quit, and smokers who never tried to quit.
Acknowledgements
This research was supported by Spanish Ministerio de Economía y Competitividad (References: PSI2012-31196) and FEDER (European Regional Development Fund).
References
American Cancer Society (2016). Cancer Facts and Figures 2016. Atlanta, GA: American Cancer Society.
Badia, X., Roset, M., Montserrat, R., Herdman, M., & Segura, A. (1999). La versión española del EuroQol: descripción y aplicaciones [The Spanish version of the EuroQol: Description and applications]. Medicina Clínica (Barcelona), 112 (Suppl. 1), 79-86.
Baker, T. B., Piper, M. E., McCarthy, D. E., Majeskie, M. R., & Fiore, M. C. (2004). Addiction motivation reformulated: An affective processing model of negative reinforcement. Psychological Review, 111, 33. doi:10.1037/0033-295X.111.1.33
Bass, P.F., Wilson, J.F., & Griffith, C.H. (2004). The association of health- related quality of life and age of initiation of smoking. The Journal of the Kentucky Medical Association, 102, 96-101.
Becoña, E., & Vázquez, F. (1998). The Fagerström Test for Nicotine Dependence in a Spanish sample. Psychological Reports, 83, 1455- 1458. doi:10.2466/pr0.1998.83.3f.1455
Becoña, E, Vázquez, M.I., Míguez, M.C, Fernández del Río, E., López, A., Martínez, U., & Piñeiro, B. (2013). Smoking habit profile and health-related quality of life. Psicothema, 25, 421-426. doi:10.7334/psicothema2013.73
Bellido-Casado, J., Martín-Escudero, J., Dueñas-Laita, A., Mena-Martín, F. J., Arzúa-Mouronte, D., & Simal-Blanco, F. (2004). The SF-36 Questionnaire as a measurement of health-related quality of life: Assessing short- and medium-term effects of exposure to tobacco versus the known long-term effects. European Journal of Internal Medicine, 15, 511-517. doi:10.1016/j.ejim.2004.06.015
Benítez, I. (2016). La evaluación de la calidad de vida: retos metodológicos presentes y futuros [The assessment of quality of life: Present and future methodological challenges]. Papeles del Psicólogo, 37, 69-73.
Brandon T. H., Vidrine J. I., & Litvin E. B. (2007). Relapse and relapse prevention. Annual Review of Clinical Psychology, 3, 257-284. doi:0.1146/annurev.clinpsy.3.022806.091455
Breslau, N., Killey, M.M., & Andreski, P. (1993). Vulnerability to psychopathology in nicotine-dependent smokers: An epidemiologic study of young adults. American Journal of Psychiatry, 150, 941-946. doi:10.1176/ajp.150.6.941
Centers for Disease Control and Prevention (2008). Cigarette smoking among adults- United States, 2007. Morbidity and Mortality Weekly Report, 57, 1221-1226.
Davila, E.P., Zhao, W., Byrne, M., Hooper, M.W., Messiah, A., Caban- Martinez, A., Dietz, N., Huang, Y., & Lee D.J. (2011). Health-related quality of life and nicotine dependence, Florida, 2007. American Journal of Health Behavior, 35, 280-289. doi:10.5993/AJHB.35.3.3
De Lossada, A., & Rejas, J. (2016). Calidad de vida relacionada con la salud en la población general española fumadora: una aproximación desde la Encuesta Nacional de Salud [Health-related quality of life in the general Spanish smoking population: An approach from the National Survey of Health]. Semergen, 42, 431-439. doi:10.1016/j.semerg.2015.09.003
De Miguel, J., Esteban M. M., Puente L., Hernández V., Carrasco P., Alvarez-Sala L. A., & Jiménez R. (2010). Relationship between tobacco consumption and health-related quality of life in adults living in a large metropolitan area. Lung, 188, 393-399. doi:10.1007/s00408-010-9256-1
Dierker, L. C., Avenevoli, S., Stolar, M., & Merikangas, K. R. (2002). Smoking and depression: An examination of mechanisms of comorbidity. American Journal of Psychiatry, 159, 947-953. doi:10.1176/appi.ajp.159.6.947
EuroQoL Group (1990). EuroQoL: A new facility for the measurement of health-related quality of life. Health Policy, 16, 199-208.
Fergusson, D. M., Goodwin, R. D., & Horwood, L. J. (2003). Major depression and cigarette smoking: Results of a 21-year longitudinal study. Psychological Medicine, 33, 1357-1367. doi:10.1017/S0033291703008596
Fidler, J. A., & West, R. (2009). Self-perceived smoking motives and their correlates in a general population sample. Nicotine & Tobacco Research, 11, 1182-1188. doi:10.1093/ntr/ntp120
Funahashi, K., Takahashi, I., Danjo, K., Matsuzaka, M., Umeda, T., & Nakaji, S. (2011). Smoking habits and health-related quality of life in a rural Japanese population. Quality of Life Research, 20, 199-204. doi:10.1007/s11136-010-9748-8
Gasperini, B., Barbadoro, P, Cherubini, A., Pierre, F., D’Errico, M. M., Di Stanislao, F., … Prospero, E. (2016). The earlier the better: Health- related quality of life is inversely related to age of smoking cessation in older former Italian smokers. Aging Clinical and Experimental Research (Epub ahead of print). doi:10.1007/s40520-016-0608-4
Goldenberg, M., Danovitch, I., & IsHak, W.W. (2014). Quality of life and smoking. The American Journal on Addictions, 23, 540-562. doi:10.1111/j.1521-0391.2014.12148.x
Grau, A., Font-Mayolas, S., Gras, M. E., Suñer, R., & Noguera, J. (2007). Calidad de vida relacionada con la salud y consumo de tabaco [Health-related quality of life and tobacco consumption]. Intervención Psicosocial, 16, 79-92. doi:10.4321/S1132-05592007000100007
Guimaraes, M., Berti, M., Luiz, C., Golbaum, M., Carandina, L., & Goi, M.C. (2011). Health-related behavior and quality of life among the elderly: A population-based study. Revista de Saúde Pública, 45, 485- 493. doi:10.1590/S0034-89102011000300006
Hajek, P., Stead, L.F., West, R., Jarvis, M., & Lancaster, T. (2013). Relapse prevention interventions for smoking cessation. Cochrane Database of Systematic Reviews, 8, CD003999. doi:10.1002/14651858.CD003999.pub3
Heatherton, T. F., Kozlowski, L. T., Frecker, R. C., & Fagerström,K. O. (1991). The Fagerström Test for Nicotine Dependence: A revision of the Fagerström Tolerance Questionnaire. British Journal of Addictions, 86, 1119-1127. doi:10.1111/j.1360-0443.1991.tb01879.x
Herdman, M. (2000). La medición de la calidad de vida relacionada con la salud [The measurement of health-related quality of life]. Medicina Clínica, 114 (Suppl. 3), 22-25.
Hughes J. R., Keely J., & Naud, S. (2004). Shape of the relapse curve and long-term abstinence among untreated smokers. Addiction, 99, 29-38. doi:10.1111/j.1360-0443.2004.00540.x
Husky, M. M., Mazure, C. M., Paliwal, P., & McKee, S. A. (2008). Gender differences in the comorbidity of smoking behavior and major depression. Drug and Alcohol Dependence, 93, 176-179. doi:10.1016/j.drugalcdep.2007.07.015
McClave, A. K., Dube, S. R., Strine, T. W., & Mokdad, A. H. (2009). Associations between health-related quality of life and smoking status among a large sample of U.S. adults. Preventive Medicine, 48, 173-179. doi:10.1016/j.ypmed.2008.11.012
Míguez, M. C., & Becoña, E. (2008). Abstinence from smoking ten years after participation in a randomized controlled trial of a self-help program. Addictive Behaviors, 33, 1369-1374. doi:10.1016/j.addbeh.2008.06.015
Mons, U., Müezzinler, A., Gellert, C., Schöttker, B., Abnet, Ch. C., Bobak, M.,… CHANCES Consortium (2015). Impact of smoking and smoking cessation on cardiovascular events and mortality among older adults: Meta-analysis of individual participant data from prospective cohort studies of the CHANCES Consortium. British Medical Journal, 350:h1551. doi:10.1136/bmj.h1551
Mulder, I., Tijhuis, M., Smit, H., & Kromhout, D. (2001). Smoking cessation and quality life: The effect of amount of smoking and time since quitting. Preventive Medicine, 33, 653-660. doi:10.1006/pmed.2001.0941
Perkins, K. A., & Scott, J. (2008). Sex differences in long-term smoking cessation rates due to nicotine patch. Nicotine & Tobacco Research, 10, 1245-1251. doi:10.1080/14622200802097506
Piasecki, T. M. (2006). Relapse to smoking. Clinical Psychology Review, 26, 196-215. doi:10.1016/j.cpr.2005.11.007
Piñeiro, B., & Becoña, E. (2013). Relapse situations according to Marlatt’s taxonomy in smokers. Spanish Journal of Psychology 16, E91, 1-12. doi:10.1017/sjp.2013.91
Pirie, K., Peto, R., Reeves, G. K., Green, J., Beral, V., & Million Women Study Collaborators (2013). The 21st century hazards of smoking and benefits of stopping: A prospective study of one million women in the UK. The Lancet, 381, 133-141. doi:10.1016/S0140-6736(12)61720-6
Prochaska, J.O., Diclemente, C.C., & Norcross, J.C. (1992). In search on how people change. Applications in addictive behaviors. American Psychologist, 47, 1102-1114. doi:10.1037/0003-066X.47.9.1102
Royal College of Physicians (2007). Harm reduction in nicotine addiction: Helping people who can’t quit. A report by the Tobacco Advisory Group of the Royal College of Physicians. London: RCP.
Sarna, L., Bialous, S.A., Cooley, M.E., Jun, H.J., & Feskanich, D. (2008). Impact of smoking and smoking cessation on health-related quality of life in women in the Nurses’ Health Study. Quality of Life Research, 17, 1217-1227. doi:10.1007/s11136-008-9404-8
Schmitz, N., Kruse, J., & Kugler, J. (2003). Disabilities, quality of life, and mental disorders associated with smoking and nicotine dependence. American Journal of Psychiatry, 160, 1670-1676. doi:10.1176/appi.ajp.160.9.1670
U.S. Department of Health and Human Services (2014). The health consequences of smoking-50 years of progress. A report of the Surgeon General. Rockville, MD: U. S. Departament of Health and Human Services, Public Health Services, Office of Surgeon General.
Vogl, M., Wenig, C. M., Leidl, R., & Pokhrel, S. (2012). Smoking and health-related quality of life in English general population: Implications for economic evaluations. BMC Public Health, 12, 203. doi:10.1186/1471-2458-12-203.
Weinberger, A. H., Kashan, R. S., Shpigel, D. M., Esan, H., Taha, F., Lee, C. J., …, Goodwin, R. D. (2016). Depression and cigarette smoking behavior: A critical review of population-based studies. The American Journal of Drug and Alcohol Abuse, 1-16. doi:10.3109/00952990.2016.1171327
Weinberger, A. H., Mazure, C. M., Morlett, A,. & McKee, S. A. (2013). Two decades of smoking cessation treatment research on smokers with depression: 1990-2010. Nicotine & Tobacco Research, 15, 1014-1031. doi:10.1093/ntr/nts213
Wilson, D. H., Chittleborough, C. R., Kirke, K., Grant, J. F., & Ruffin, R. E. (2004). The health-related quality of life of male and female heavy smokers. Social and Preventive Medicine 49(6), 406-412. doi:10.1007/s00038-004-3075-1