ORIGINAL ARTICLE
Received: 07 May 2023
Accepted: 10 February 2024
DOI: https://doi.org/10.53886/gga.e0000043_EN
Abstract
Objective: To describe the psychotropic drug deprescription process in older patients of a geriatric psychiatry outpatient clinic.
Methods: We conducted a quasi-experimental study of people aged ≥ 60 years who were treated at Hospital São Lucas’ Geriatric Psychiatry Outpatient Clinic, which is affiliated with Pontifícia Universidade Católica do Rio Grande do Sul, Brazil. Data on 150 older people were collected from March 2021 to August 2022 and were evaluated by the pharmacists. The inclusion criteria were age ≥ 60 years, being a patient of the hospital’s Geriatric Psychiatry Outpatient Clinic, use of at least one psychotropic drug, and agreeing to participate in the study. Those unable to report their medications and those who only came to the first appointment were excluded.
Results: Overall, deprescription of at least one psychotropic drug was indicated in 61.3% (n = 92) of the participants, and it was effectively implemented in 68.5% (n = 63) of this group. Deprescribing, which was more frequent in the youngest age group (60–69 years) (p = 0.049), was indicated for 37.4% (n = 136) of psychotropic drugs, 67.6% (n = 92) of which were effectively deprescribed. The main classes indicated for deprescription were hypnotics and sedatives (90.0%; n = 18) and anxiolytics (73.3%; n = 11).
Conclusions: At least 1 psychotropic drug was indicated for deprescription in the majority of the patients, and in most cases it was effectively implemented. One-third of the prescribed psychotropic drugs were indicated for deprescription, and more than half were successfully deprescribed.
Keywords: Aged, deprescriptions, drugs, psychotropic drugs.
INTRODUCTION
The world’s population is aging at a rapid pace. In 2020, people over the age of 60 years accounted for 13.5% of the world’s population, and this proportion is expected to nearly double by 2100.1 Since organic, biochemical, psychological, and behavioral changes occur during the aging process,2,3 longevity and its consequences pose new challenges to health systems. In addition to extensive clinical attention, older people should also receive adequate mental health care.4,5
Mental disorders are highly prevalent in the geriatric population, affecting approximately 15% of older adults.3 Depression and dementia are the most common mental disorders in this age group. However, other disorders also occur, such as anxiety, alcohol abuse, manias, and sedative dependence.4 Depression affects approximately 28% of older adults, with 10% to 25% showing depressive symptoms of varying severity, whereas the prevalence of anxiety disorders is 11.4% to 12.3% in this age group.6 These conditions lead to high rates of psychotropic drug use among older adults.5,7
Most drugs indicated for mental disorders produce adverse reactions, to which older patients are more susceptible. Therefore, many of these drugs are considered potentially inappropriate medications (PIMs) for older people, making it necessary to regularly check and analyze care planning and polypharmacy.4,5,8 Some antidepressants have high anticholinergic properties, also causing sedation and orthostatic hypotension, while drugs used to treat anxiety and insomnia have long-term physical effects on older adults, leading to drowsiness and an increased risk of falls and fractures.9
As a contributor to mental health care, the deprescription process can be integrated into clinical practice to assess and prevent medication-induced harm in older people.10 Studies have shown that having a pharmacist on the multidisciplinary team further reduces the use of PIMs by older mental health service patients.7,11 Medication review may prevent possible drug-drug interactions and adverse drug reactions, reducing potential health risks.12
In mental health care, deprescribing practices by an interdisciplinary team can expand care services and promote mental well-being among older adults.9 Therefore, we aimed to describe the psychotropic drug deprescription process among older patients of a geriatric psychiatry outpatient clinic.
METHODS
We conducted a quasi-experimental study as part of the Aging and Mental Health Program, which is a program to monitor and provide mental health care services for people aged ≥ 60 years. The program was developed jointly by Hospital São Lucas’ Department of Psychiatry and Pontifícia Universidade Católica do Rio Grande do Sul (PUCRS) through its School of Medicine’s Psychiatry Training Center and Institute of Geriatrics and Gerontology. The Hospital São Lucas is a teaching hospital affiliated with PUCRS, and both institutions are located in Porto Alegre, southern Brazil.
The study population consisted of people aged ≥ 60 years who were treated at the Hospital São Lucas’ Geriatric Psychiatry Outpatient Clinic. The inclusion criteria were age ≥ 60 years, receiving services at the Hospital São Lucas’ Geriatric Psychiatry Outpatient Clinic, use of ≥ 1 psychotropic drug, and agreeing to participate in the study by providing written informed consent. Individuals who were unable to report their medications and those who only attended the first appointment were excluded.
Data on 150 older patients were collected between March 2021 and August 2022. All stages of the multidisciplinary team’s deprescribing process, which consisted of physicians and pharmacists, have been previously published in detail as a methodological protocol.12 The current study focused only on the deprescription of psychotropic drugs, disregarding other drug classes.
Each patient in the geriatric psychiatry outpatient clinic was initially seen by a psychiatrist and assessed using a general questionnaire to collect data on sociodemographic characteristics, lifestyle habits, medications, and general health. Screening instruments for anxiety, depression, sleep quality, and cognition were also applied. Psychiatric diagnoses were classified according to the DSM-5.13 The patients were subsequently evaluated by pharmacists from the multidisciplinary team.
During the evaluation, the pharmacists administered a questionnaire to collect as much information as possible about the patient’s medications. The pharmacists also collected data on lifestyle habits, such as tobacco, alcohol, and caffeine use, history of adverse drug reactions, and adherence to drug therapy using the Treatment Adherence Measure.14 This instrument was included in the study questionnaire by permission from the authors.
Based on the pharmacists’ evaluation, the patients’ drugs were classified according to the Anatomical Therapeutic Chemical classification system.15 Patients were assessed for polypharmacy, which was defined as the use of ≥ 5 regular medications.16 Medications with ≥ 2 active substances were considered ≥ 2 different medications. Medications with the same active substance at different doses were also considered different medications. The Beers Criteria were used to determine which psychotropic drugs were PIMs,17 and potential drug-drug interactions were identified through the drugs.com website.18
After the medication review, the pharmacists, together with the medical team, reviewed and discussed all the individual aspects of the patient’s health and identified psychotropic drugs for potential deprescription. Indications were discussed with the psychiatrists and shared decisions were made about which drugs should be discontinued. The reasons for deprescribing PIMs included unnecessary use and potential adverse drug reactions or drugdrug interactions.
During the return appointment, the physician was responsible for initiating and guiding appropriate deprescription. To this end, the physicians used deprescribing strategies and algorithms.10,12,19,20,21,22 Medications were either reduced gradually (gradual withdrawal) or stopped abruptly (abrupt withdrawal). While guiding the deprescribing process, the patient’s real possibilities and individual preferences about pharmacological changes were observed. Considering these factors, deprescription was adjusted to the patient’s individual characteristics.
In subsequent clinical visits, the multidisciplinary team closely monitored the older patients’ health status. If treatment changes were required, new interventions were developed and implemented. The patients were monitored closely throughout the outpatient follow-up period.
The data were analyzed using IBM SPSS Statistics 22 (IBM, Armonk, NY, USA). The variables were expressed as frequencies, means, and SD. Associations between categorical variables were analyzed using Pearson’s chi-square test. In specific cases, the chi-square test for linear trend was used (ordinal variables). P-values < 0.05 was considered significant.
This study is linked to the Aging and Mental Health Program, which was previously approved by the PUCRS Research Ethics Committee (decision 89158218.5.0000.5336). All patients or their legal representatives provided written informed consent to participate.
RESULTS
A total of 150 older patients were included in the study, whose mean age was 71.5 (SD, 7.86, range: 60-89) years. Most participants were women, had 9 to 12 years of education, lived with a partner, and were retired (Table 1). Regarding clinical characteristics, most patients had ≥ 1 comorbidity (89.1%), were on polypharmacy (77.4%), had good medication adherence (78.8%), and were diagnosed with mood or anxiety disorders (45.3% and 44.7%, respectively) (Table 2).
The relationship between the participants’ sociodemographic characteristics and deprescription indication and implementation for ≥ 1 medication.
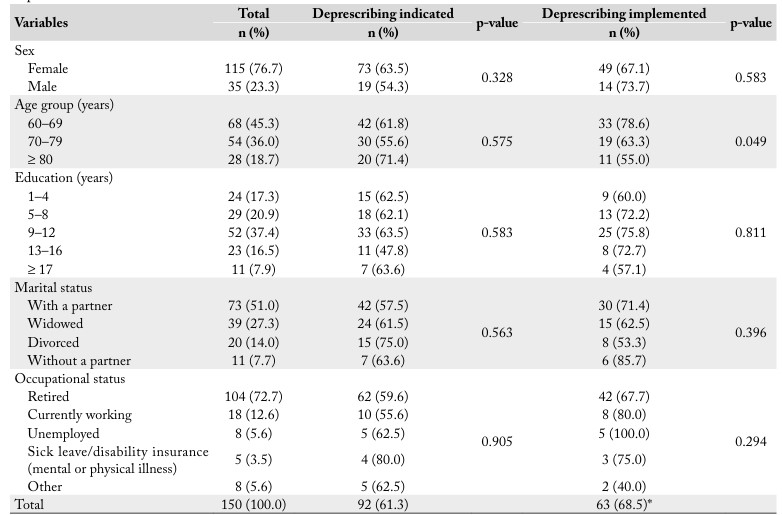
The total for each variable may not reach n = 150 due to sample losses. *n = 92.
The relationship between the participants’ clinical characteristics and deprescription indication and implementation for ≥ 1 medication.
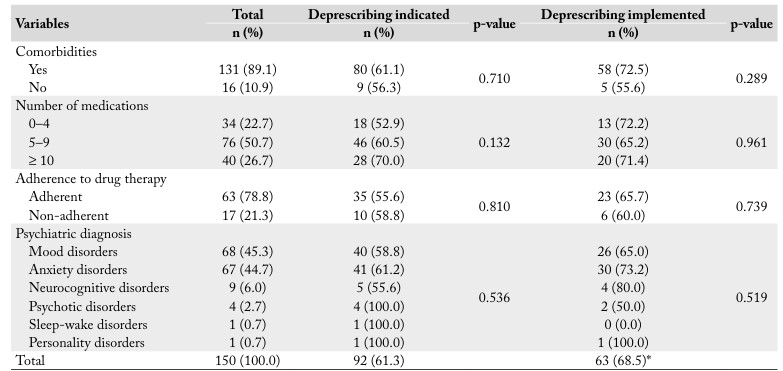
The total for each variable may not reach n = 150 due to sample losses. *n = 92.
Overall, at least 1 psychotropic drug was indicated for deprescription in 61.3% (n = 92) of the participants, and it was effectively implemented in 68.5% (n = 63) of these patients. Age was the only significant sociodemographic or clinical difference between participants for whom deprescribing was indicated vs those in whom it was implemented. Deprescribing was more frequently implemented in the youngest age group (60 – 69 years) (p = 0.049) (Tables 1, 2).
A total of 1149 regular medications were used by the study population. Regarding the main drug classes, antidepressants (14.4%) were the most commonly used agents, followed by agents that act on the renin-angiotensin system (7.9%), and lipid-modifying agents (7.5%).
Of all regular medications, 31.7% (n = 364) were psychotropic drugs, of which 50 different types were identified. Antidepressants (45.6%), antipsychotics (19.8%), and antiepileptics (15.7%) were the main psychotropic drug groups (Table 3). The most frequently used psychotropic drugs were sertraline (8.0%), quetiapine (7.4%), escitalopram (7.1%), trazodone (6.9%), and mirtazapine (6.6%). The mean number of psychotropic drugs used by each patient was 2.4 (SD, 1.25).
Classes of prescribed psychotropic drugs in relation to deprescription.
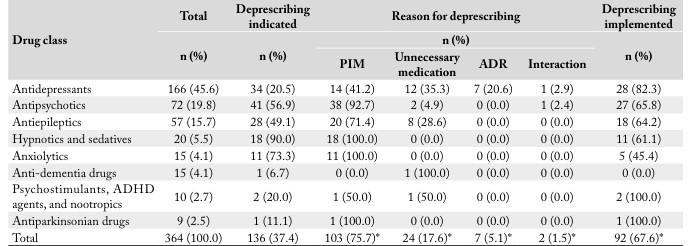
ADHD: attention deficit hyperactivity disorder; ADR: adverse drug reaction; PIM: potentially inappropriate medication. *n=136.
Deprescribing was indicated for 37.4% (n = 136) of psychotropic drugs, of which the main classes were hypnotics and sedatives (90.0%; n = 18) and anxiolytics (73.3%; n = 11). In both of these classes, all drugs were classified as PIMs. Among all drug classes, identification as a PIM was the main reason for deprescribing (75.7%) (Table 3). Deprescription of ≥ 1 PIM was indicated in 52% (n = 78) of the patients.
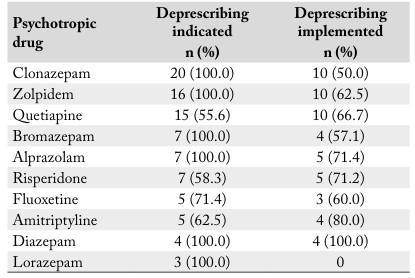
Deprescribing was indicated in 100% of the patients who were using zolpidem, clonazepam, bromazepam, diazepam, alprazolam, and lorazepam, and it was highly indicated in others, such as fluoxetine (71.4%), amitriptyline (62.5%), risperidone (58.3%), and quetiapine (55.6%). Diazepam was the only psychotropic drug to be effectively deprescribed in all cases (100%), whereas ≥ 50.0% of the others were also effectively deprescribed (Table 4).
The main psychotropic drugs for which deprescribing was indicated and implemented.
Overall, of the psychotropic drugs indicated for deprescribing, 67.6% (n = 92) were effectively deprescribed. Psychostimulants, attention deficit hyperactivity disorder agents, nootropics, antiparkinsonian drugs, and antidepressants had the highest rates of successful deprescription (Table 3). The drugs were withdrawn abruptly in 62.0% (n = 57) of the cases and withdrawn gradually in 38.0% (n = 35) of the cases. The highest rate of gradual withdrawal was for hypnotics and sedatives (72.7%), followed by anxiolytics (60.0%). In contrast, antipsychotics (74.1%) and antidepressants (71.4%) were withdrawn abruptly in most cases. All antiparkinsonian drugs, psychostimulants, attention deficit hyperactivity disorder agents and nootropics were withdrawn abruptly.
DISCUSSION
Aiming to reduce the inappropriate use of psychotropic drugs by older people, a deprescribing strategy was used in a geriatric psychiatry outpatient clinic. At least 1 psychotropic drug was indicated for deprescribing in more than half of the patients, and it was effectively implemented in 68.5% of this group. Although deprescription was most indicated among those aged ≥ 80 years, this group had the lowest rate of success. The youngest age group (60-69 years) had a significantly higher prevalence of successful deprescribing. The oldest old are more likely to develop serious complications from PIMs, and it is essential to identify these drugs more rigorously, given the wide range of reasons for deprescribing.23,24 However, the oldest old are more resistant to lifestyle changes, including discontinuing their medications. The rate of successful deprescribing may have been significantly higher among the youngest group because they accept new drug therapies more easily and are more motivated to take care of their health and follow medical recommendations.25
Indications for deprescribing were more numerous among older patients with comorbidities, as was the success rate. The number of indications for deprescribing also increased with the number of medications used. Older people with chronic diseases must often see various specialists, resulting in the use of several prescription medications. Use of a higher number of medications is associated with an increased risk of polypharmacy.26 In an effort to minimize this harm, reducing unnecessary or inappropriate psychotropic drugs was recommended, leaving only drugs crucial to the patient’s health.
As a result of multidisciplinary discussion, including medication review, more than one-third of the psychotropic drugs were indicated for deprescribing among these patients. The physicians accepted most indications. These results are consistent with previous studies that have demonstrated the importance of a pharmacist-led medication review in a multidisciplinary team.27,28,29 In a Slovenian study involving psychogeriatric outpatients, pharmacists proposed 374 psychopharmacotherapy interventions (61.5% drug discontinuations, 28.6% drug initiations, and 10.9% dose adjustments) and the physicians accepted 45.2% of them. The interventions reduced the total number of medications per patient, PIMs, potential drug-drug interactions, and resulted in greater adherence to treatment guidelines.7
The medical team does not always implement deprescription interventions. In some cases, although eligible for deprescribing, psychotropic drugs are the only option with the desired efficacy to treat an older patient’s specific condition. In these situations, regular patient monitoring is essential.12 Another barrier to deprescribing among older patients is patient resistance, which can be due to medication dependence or fear of interrupting or replacing treatment.20 The drug classes most indicated for deprescribing in our sample were hypnotics/sedatives and anxiolytics, due to their classification as PIMs. However, despite being highly indicated, they had the lowest rate of successful deprescription. One explanation for this could be that the main drugs in these classes are benzodiazepines, whose long-term use can cause tolerance, dependence, and withdrawal symptoms, making deprescribing difficult.21,22
Regarding the withdrawal regimen, most psychotropic drugs were stopped abruptly; only 38.0% were reduced gradually. The main drug classes to be gradually withdrawn were hypnotics and sedatives, followed by anxiolytics. The most recommended method is slow and gradual withdrawal, which requires structured steps for drug discontinuation. Gradual withdrawal is usually preferred in cases of diagnostic doubt, medications commonly associated with discontinuation or withdrawal syndromes, and physician and/or patient uncertainty.21 In contrast, antipsychotics and antidepressants were stopped abruptly in most cases. This was probably because lowdose antipsychotics were often prescribed for insomnia, with no need for gradual withdrawal. Antidepressants were withdrawn abruptly in most cases but were replaced by another drug with similar action.10,21,22
Another finding was the high prevalence of polypharmacy, which was expected since it is common among older patients.8,16 The average of 2.4 psychotropic drugs per patient also indicated “psychiatric polypharmacy.” This term refers to the concurrent use of ≥ 2 psychotropic drugs from different classes or within the same class.7,11 A study of older patients with mental disorders at 2 primary care units in Marília, São Paulo, Brazil found that they were taking an average of 3.3 psychotropic drugs.30 Psychiatric polypharmacy is increasing in all age groups, but it is particularly critical in older adults because many of these medications are considered PIMs and are potentially harmful to health.2 These risks can be added to those of common polypharmacy, thus increasing the likelihood of adverse drug reactions, drug-drug interactions, intoxication, medication errors, and medication non-adherence.26
One strength of this study is that, before implementing the deprescribing process, the pharmacists developed a methodological protocol that described all necessary steps.12 Meanwhile, the pharmacists emphasized the importance of deprescribing to the medical team through lectures and group discussion. During implementation, all physicians recognized the importance of deprescribing for the health of their older patients and managed to incorporate it into their routine outpatient care without problems. Based on this increased awareness, new prescriptions considered patient safety according to the concept of quaternary prevention, an approach based on avoiding iatrogenic harm to patients.31 Beneficial relationships were developed among multidisciplinary team members, since the roles of all health professionals were recognized and respected in clinical discussions. This collaboration facilitated the implementation of deprescription and ensured quality treatment for patients.
Some study limitations should be addressed, such as the scarce literature on psychotropic drug deprescription in older adults. Most studies have investigated specific drug classes in isolation and have included other age groups, precluding proper comparison of the results and validation of the evidence. The characteristics of the study population are another limitation, since all participants attended a geriatric psychiatry outpatient clinic, that is, the study focused mainly on individuals with sufficient financial resources to access mental health services. Therefore, the results may not be representative of the entire Brazilian population.
CONCLUSIONS
Adequate mental health care, combined with a comprehensive medication review, can reduce the large number of inappropriate psychotropic drugs used by older people. Deprescription was indicated for at least 1 psychotropic drug in the majority of older patients in this study, and in most cases it was effectively implemented. One-third of the patients’ psychotropic drugs were indicated for deprescription, and more than half of those indicated were successfully deprescribed.
The results of this study contribute to several aspects of geriatric care, such as description of a multiprofessional prescription strategy, the prescribing process for different classes of drugs, and deprescription success rates.
REFERENCES
Alves JED. Envelhecimento populacional continua e não há perigo de um geronticídio, artigo de José Eustáquio Diniz Alves. EcoDebate. 2020. Disponível em: https://www.ecodebate.com.br/2020/06/19/envelhecimento-populacional-continua-e-nao-ha-perigo-de-um-geronticidio-artigo-de-jose-eustaquio-dinizalves/. Acessado em Fev 05, 2024.
Silva E, Santos E, Pucci SHM. O impacto da qualidade de vida na saúde mental do idoso. Revista Ibero-Americana de Humanidades, Ciências e Educação. 2021;7(10):481-511. https://doi.org/10.51891/rease.v7i10.2588
World Health Organization. Mental health of older adults. Geneva: WHO; 2017. Available from: https://www.who.int/news-room/fact-sheets/detail/mental-health-of-older-adults/. Accessed Dec 07, 2022.
D’Agostin MB, Budni J. Psicogeriatria: modificações farmacocinéticas e farmacodinâmicas associadas ao envelhecimento. Inova Saúde. 2019;9(2). https://doi.org/10.18616/inova.v9i2.3595
Dantas DG, Portugal KSCM, Batista JPS, Mendes CMM, Ribeiro IAP, Marques LL. Uso de psicofármacos por idosos institucionalizados: aspectos epidemiológicos e frequência de queda. Rev Enferm Atual In Derme. 2019;88(27):1-7. https://doi.org/10.31011/reaid-2019-v.89-n.27-art.463
Petrova NN, Khvostikova DA. Prevalence, structure, and risk factors for mental disorders in older people. Adv Gerontol. 2021;11:409-15. https://doi.org/10.1134/S2079057021040093
Stuhec M, Zorjan K. Clinical pharmacist interventions in ambulatory psychogeriatric patients with excessive polypharmacy. Sci Rep. 2022;12:11387. https://doi.org/10.1038/s41598-022-15657-x
Santos GK, Dias QJN, Martins TS. Revisão sistemática sobre a atenção farmacêutica ao idoso no uso da polifarmácia. Braz J Dev. 2021;7(9):93225-40. https://doi.org/10.34117/bjdv7n9-471
Estrela M, Herdeiro MT, Ferreira PL, Roque F. The use of antidepressants, anxiolytics, sedatives and hypnotics in europe: focusing on mental health care in portugal and prescribing in older patients. Int J Environ Res Public Health. 2020;17(22):8612. https://doi.org/doi:10.3390/ijerph17228612.
Moraes EN. A arte da (des)prescrição no idoso: a dualidade terapêutica. Belo Horizonte: Folium; 2018.
Stuhec M, Bratović N, Mrhar A. Impact of clinical pharmacist’s interventions on pharmacotherapy management in elderly patients on polypharmacy with mental health problems including quality of life: a prospective non-randomized study. Sci Rep. 2019;9(1):16856. https://doi.org/10.1038/s41598-019-53057-w
Linkievicz NM, Engroff P, Cataldo Neto A, Sgnaolin V. The process of deprescribing in older adults: a methodological protocol. Geriatr Gerontol Aging. 2022;16:e0220021. https://doi.org/10.53886/gga.e0220021
Associação de Psiquiatria Americana. manual diagnóstico e estatístico de transtornos mentais: DSM-V. 5. ed. Porto Alegre: Artmed, 2014.
Delgado AB, Lima ML. Contributo para a validação concorrente de uma medida de adesão aos tratamentos. Psicologia Saúde & Doenças. 2001;2(2):81-100.
World Health Organization Collaborating Centre for Drug Statistics Methodology. International language for drug utilization research. Geneva: WHO; 2022. Available from: https://www.whocc.no/. Accessed Dec 07, 2022.
Varghese D, Ishida C, Koya HH. Polypharmacy. In: StatPearls. Treasure Island: StatPearls Publishing, 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532953/. Accessed Dec 07, 2022.
By the 2023 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2023 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2023;71(7):2052-81. https://doi.org/10.1111/jgs.18372
Drugs.com. Find drugs & conditions Available from: https://www.drugs.com/. Accessed Dec 07, 2022.
Scott IA, Hilmer SN, Reeve E, Potter K, Le Couteur D, Rigby D, et al. Reducing inappropriate polypharmacy: the process of deprescribing. JAMA Intern Med. 2015;175(5):827-34. https://doi.org/10.1001/jamainternmed.2015.0324
Reeve E. Deprescribing tools: a review of the types of tools available to aid deprescribing in clinical practice. J Pharm Pract Res. 2020;50(1):98-107. https://doi.org/10.1002/jppr.1626
Sgnaolin V, Engroff P, Linkievicz NM, Morrone FB. Desprescrição de psicofármacos. In: Cataldo Neto A, Sgnaolin V, Gauer GJC, Furtado NR, orgs. Psiquiatria para estudantes de medicina. 3ª ed. Porto Alegre: EDIPUCRS, 2021. p. 569-85.
Farrell B. Deprescribing guidelines and algorithms. Deprescribing.org.; 2018. Available from: https://deprescribing.org/resources/deprescribing-guidelines-algorithms/. Accessed Dec 07, 2022.
Curtin D, Gallagher P, O’Mahony D. Deprescribing in older people approaching end-of-life: development and validation of STOPPFrail version 2. Age Ageing. 2021;50(2):465-71. https://doi.org/doi:10.1093/ageing/afaa159
Furtado NL, Zottich APN, Bernardina BAD, Perusse CB, Anjos JPT, Bachetti LG, et al. Polifarmácia na população longeva: os limites entre a medicação incontingente e as repercussões fisiopatológicas. Brazilian Journal of Health Review. 2021;4(5):23224-40. https://doi.org/10.34119/bjhrv4n5-396
Clyne B, Cooper JA, Boland F, Hughes CM, Fahey T, Smith SM, et al. Beliefs about prescribed medication among older patients with polypharmacy: a mixed methods study in primary care. Br J Gen Pract. 2017;67(660):e507-e518. https://doi.org/10.3399/bjgp17X691073
Ye L, Yang-Huang J, Franse CB, Rukavina T, Vasiljev V, Mattace-Raso F, et al. Factors associated with polypharmacy and the high risk of medication-related problems among older community-dwelling adults in European countries: a longitudinal study. BMC Geriatr. 2022;22(1):841. https://doi.org/10.1186/s12877-022-03536-z
Kiesel EK, Drey M, Pudritz YM. Influence of a ward-based pharmacist on the medication quality of geriatric inpatients: a before-after study. Int J Clin Pharm. 2022;44(2):480-8. https://doi.org/10.1007/s11096-021-01369-1
Hatano M, Mizuno T, Arakawa Y, Inagaki R, Kato A, Matsuzaki H, et al. Efficacy of a pharmacist team clinical medication review in older adults: a prospective and retrospective observational study. Biol Pharm Bull. 2022;45(8):1166-71. https://doi.org/10.1248/bpb.b22-00245
Potter EL, Lew TE, Sooriyakumaran M, Edwards AM, Tong E, Aung AK. Evaluation of pharmacist-led physician-supported inpatient deprescribing model in older patients admitted to an acute general medical unit. Australas J Ageing. 2019;38(3):206-10. https://doi.org/10.1111/ajag.12643
Marin MJS, Maftum MA, Lacerda MR. Elderly people with mental disorders: experiencing the use of psychotropic medicines. Rev Bras Enferm. 2018;71(suppl 2):888-96. https://doi.org/10.1590/0034-7167-2016-0159
Jamoulle M. Quaternary prevention, an answer of family doctors to overmedicalization. Int J Health Policy Manag. 2015;4(2):61-4. https://doi.org/10.15171/ijhpm.2015.24
Notes
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal Nível Superior – Brazil (CAPES) – Finance Code 001.
This study is linked to the Aging and Mental Health Program, which was previously approved by the PUCRS Research Ethics Committee (decision CAAE 89158218.5.0000.5336). All patients or their legal representatives provided written informed consent to participate. The “SPIRIT-Outcomes checklist” from the Equator Network was followed in study.
Author notes
Correspondence data Natascha Melo Linkievicz – Avenida Ipiranga, 6681, prédio 40, 8º andar, sala 804 – Partenon – CEP 90619-900 – Porto Alegre (RS), Brazil. E-mail: nataschamel@gmail.com
Conflict of interest declaration
The authors declare no conflicts of interest.
