ORIGINAL ARTICLE
Path analysis of urinary incontinence in older adults living in nursing homes
 Samuel de Jesus Fidyk
Maria Liz Cunha de Oliveira
Lílian Barbosa Ramos
Anna Karla Carneiro Roriz
Sandra Maria Lima Ribeiro
Letícia do Nascimento Maximiano Ferreira
Samuel de Jesus Fidyk
Maria Liz Cunha de Oliveira
Lílian Barbosa Ramos
Anna Karla Carneiro Roriz
Sandra Maria Lima Ribeiro
Letícia do Nascimento Maximiano Ferreira
Path analysis of urinary incontinence in older adults living in nursing homes
Geriatrics, Gerontology and Aging, vol. 18, e0000051, 2024
Sociedade Brasileira de Geriatria e Gerontologia, SBGG
Received: 23 July 2023
Accepted: 16 November 2023
Abstract
Objective: To investigate the factors associated with urinary incontinence in older adults living in nursing homes.
Methods: This exploratory, cross-sectional, observational, and quantitative study used exploratory and path analysis (PA). Eighty-six older adults living in nursing homes in the city of Salvador, Brazil, and the city of Brasília, Brazil, were included. Data were collected from January to March 2020, before the Covid-19 pandemic. The following variables were evaluated: sex, age group, functional performance, global cognitive function, comorbidities, and health conditions. We considered urinary incontinence for older adults who answered affirmatively to the “In the last 12 months, have you had an involuntary loss of urine?”. Data were initially analyzed by descriptive analysis and nonparametric statistical tests. A PA was performed using generalized structural equation modeling to investigate the relationship between the variables of interest and the direct and indirect effects of the independent variables and UI according to the theoretical model. Subsequently, the statistical distributions of the variables and the connections were defined for the regression estimation. After the analysis, the model was respecified, excluding the variables and paths that were not statistically significant to determine the best model. The final model was designed after statistical adjustments, corroborating or not with the theoretical model.
Results: Urinary incontinence was associated with educational level, marital status, hypertension, one or more difficulties in basic activities of daily living, mood, insomnia, loss of appetite, fecal incontinence, and difficulty swallowing. In the PA, depression and difficulty swallowing were directly associated with urinary incontinence, and urinary incontinence was directly and significantly associated with insomnia and fecal incontinence.
Conclusion: Given the variety of social and health components associated with urinary incontinence, it is necessary to assess, prevent, treat, and rehabilitate this condition in Brazilian nursing homes. Interventions in urinary incontinence demand integrated actions in functional, clinical, and mental health aspects to promote the well-being of older adults living in nursing homes.
Keywords: Urinary incontinence+ physical functional performance+ depression+ health services for the aged+ long-term care.
INTRODUCTION
The mechanisms of urine storage and bladder emptying involve a coordinated action between the nerve centers and muscles involved in these processes.1,2 The absence of coordination or the abnormal function of these processes characterize disorders. In these cases, cognitive and mobility disorders, as well as their association with other diseases, can lead to urinary incontinence (UI).¹ As these disorders are more prevalent with aging, older adults are the group most affected by UI and its associated harmful factors.2,3
Abrams et al.4 describe involuntary loss of urine as a manifestation triggered by morphological changes in the bladder observed with aging, such as decreases in bladder elasticity and ureteric jet velocity, leading to uninhibited detrusor contractions.4,5,6 In addition, pelvic floor disorders may cause incontinence, such as contractile dysfunction and involuntary reflexes of the external anal sphincter.6 UI has multiple predisposing factors and outcomes, meaning that interventions in this condition demand adequate assessment, planning, and multifactorial action.5
In the setting of older adults living in nursing homes, UI has received greater attention from researchers with the aim of documenting the health profile of this population and developing interventions. Unlike older adults living in the community, those living in nursing homes are more dependent and frailer, presenting greater clinical complexit y.7 A survey conducted with 551 Chinese older adults living in nursing homes aged 75 years or older found a UI prevalence of 24.3%, and this condition was associated with constipation, immobility, use of wheelchair, cardiovascular disease, and pelvic and spinal surgeries.7 Guimarães et al. found a high prevalence of depressive symptoms in Brazilian older adults living in nursing homes, which was significantly associated with UI.8 Therefore, UI is associated with clinical and functional vulnerability and mental health conditions in this age group.
Huang et al. found that UI in older adults living in nursing homes was significantly associated with a higher risk of mortality (OR = 1.20), varying according to region, cognitive status, and follow-up period.9 Participants residing in Asian countries had a higher risk of mortality compared with residents of Western countries (OR = 2.20 vs OR = 1.18), as well as individuals without dementia compared with those with dementia (OR = 1.35 vs OR = 1.17) and those who were followed up for more than 1 year compared with those who were followed up for shorter periods (OR = 1.30 vs OR = 1.16). In view of these findings, early detection and intervention of UI are of utmost importance for older adults living in nursing homes.
These studies show that investigating the factors associated with UI in older adults living in nursing homes is essential, as it supports the development of prevention and health care strategies aimed at promoting the well-being and health of this population. The prevention of UI is justified to avoid the undesirable consequences of UI, such as mood disorders, the need to purchase pads, and the risk of associated conditions such as urinary tract infections.7,8,9
Studies on UI in Brazilian and other Latin American populations are scarce. Therefore, this study aimed to investigate the factors associated with UI in Brazilian older adults living in nursing homes, with emphasis on sociodemographic factors, functional performance, mood, morbidities, and health conditions. Exploratory and path analysis (PA) were performed. PA methods provide biological and clinical insights, thus maximizing interpretation and the development of hypotheses. This statistical approach incorporates biological knowledge and helps to understand the heterogeneity of the relationships between variables.10
METHODS
This was an exploratory, cross-sectional, observational, and quantitative study assessing the prevalence of self-reported UI in older adults living in nursing homes.
Three nursing homes participated in the study, 1 located in the city of Brasília, Brazil, and 2 in the city of Salvador, Brazil. Of the initial total sample of 185 residents (90 from Brasília and 95 from Salvador), only 86 were included in the study. The loss of potential participants was higher in Brasília: of 90 older adults, 70 were potentially eligible, but only 22 were investigated. In Salvador, of 95 participants, a total of 75 were potentially eligible, and 64 were investigated. The study was initiated in January but had to be interrupted in March because of the Covid-19 pandemic.
The 3 participating nursing homes were selected based on the following inclusion criteria:
-
a. being public or philanthropic;
-
b. being in the same physical space for at least 2 years;
-
c. having a technical manager available for participating in the activities;
-
d. agreeing to participate in the study.
In both cities, 4 institutions met all the inclusion criteria. Two institutions from Brasília and 3 from Salvador provided informed consent, but only 1 in Brasília and 2 in Salvador were included due to limitations imposed by the Covid-19 pandemic.
As for the inclusion criteria of participants, they had to have been living in the nursing home for at least 6 months and had to agree to participate in the study. There were no restrictions on age and sex. The exclusion criteria were sensory difficulties and difficulty understanding the questions; aphasia, agnosia, or speech and language problems that could hinder communication; and bedridden individuals or individuals with untreated psychiatric morbidities. These criteria were employed due to the self-report nature of the questions used for the evaluations.
Initially, visits to the nursing homes were scheduled to establish rapport, explain the purpose of the study, and to come to an agreement on the process of data collection. After the visits, timelines were established with the managers of the nursing homes for conducting individual interviews with the participants. The interviews were conducted from January to early March of 2020, before the Covid-19 pandemic, with the participation of a team of 15 undergraduate and graduate students in each city.
To conduct the assessments, all participants were informed about the objectives of the study and received guidance on the signing of the Informed Consent Form, in accordance with Ordinance No. 466 of 2012 of the Ministry of Health. The study was approved by the Research Ethics Committee of the Federal University of Bahia (CAAE: 18561419.5.1001.5023, assessment number: 3.793.529) and the Catholic University of Brasília (CAAE: 18151019.1.1001.0029, assessment number: 3.621.190).
After consenting to participate in the study, individual interviews were scheduled to be conducted in a calm and silent environment at the institution where the participant lived, at previously agreed times compatible with the institution’s routine.
Participants were assessed using the following instruments:
-
Sociodemographic questionnaire with questions about age, sex, education, and marital status.
-
Self-report health questionnaire with questions about chronic diseases (by number: 0, 1, 2, or more self-reported diseases; and type: hypertension, diabetes, stroke, cardiovascular disease, Parkinson’s disease, osteoporosis); health conditions (loss of appetite, memory problems, skin injuries, hospitalization, difficulty chewing solid foods, and difficulty swallowing food); and number of medications taken (0 to 4 medications; 5 medications or more), collected from the participants’ medical records.
-
To identify participants with UI, the following question was used: “In the last 12 months, have you had UI (or involuntary loss of urine)?”. Older adults who answered affirmatively were classified as incontinent and those who answered negatively as without incontinence.
-
Mini Mental State Examination to assess global cognitive status.11 The cutoff points adopted for classifying participants with cognitive decline were: 13 for low literacy levels; 18 for people with 1 to 8 years of formal education; and 26 for people with 9 years or more of formal education.12
-
Four-item Geriatric Depression Scale (GDS), based on the 15-item scale adapted for the Brazilian population by Almeida and Almeida13 from the 30-item scale originally created by Yesavage et al.14 to screen for depression in older adults. The score ranges from 0 to 15 points, with 6 points or more suggesting depression. In this study, we used the short version of the GDS, which contains 4 items and patients can score from 0 to 4. This version was developed by Castelo et al.15 and contains the following questions: “Are you basically satisfied with your life?”, “Do you feel that your life is empty?”, “Are you afraid that something bad is going to happen to you?”, and “Do you feel happy most of the time?”. The cutoff point for an answer compatible with depression was 1 point, with a sensitivity of 84.20% and specificity of 74.70%. In the present study, participants were classified into 3 groups: individuals who scored 0, 1 point, and 2 points or more.
-
Katz Index of Independence in Activities of Daily Living to assess the absence or presence of difficulties in basic activities of daily living (BADLs) related to self-care (going to the toilet, eating, moving, getting around, bathing, personal hygiene).16,17 Participants were classified as “without limitations” or “with 1 limitation or more”.
-
Insomnia Scale to determine the prevalence of dyssomnia in the study population. The questionnaire is composed of 4 questions directly related to insomnia (with a single affirmative answer being enough to consider the presence of this sleep disorder) and a question related to daytime sleepiness.18
The data were initially analyzed by descriptive analysis and nonparametric statistical tests to compare groups of older adults with or without self-reported UI as a function of independent variables (sociodemographic, mood, global cognitive performance, morbidities, and health conditions). Subsequently, a PA was performed using generalized structural equation modeling to investigate the relationship between the variables of interest and the direct and indirect effects of the independent variables and UI according to the theoretical model (Figure 1). The PA method was selected because it presents the possible relationships between the variables, even if in an exploratory model.
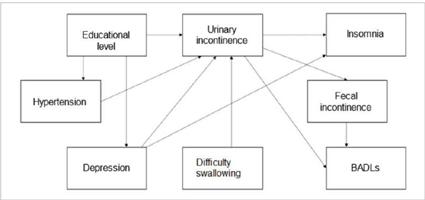
FIGURE 1
Theoretical model of factors associated with urinary incontinence in older adults residing in nursing homes.
In the proposed model, latent variables were not included, thus, only a structural model with observed variables was performed. Subsequently, the statistical distributions of the variables and the connections were defined for the regression estimation. After the estimation, the model was respecified, excluding the variables and paths that were not statistically significant to define the best model. After statistical adjustments, corroborating or not with the theoretical model, the final model was designed (Figure 2). The analyses were performed on STATA version 14, with the significance level set at p < 0.05.
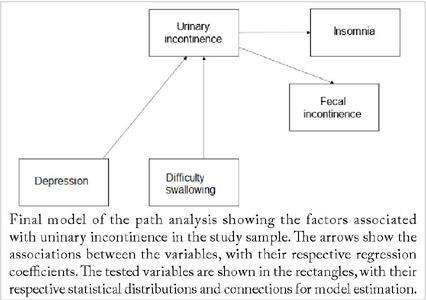
FIGURE 2
Pathway analysis of the associated factors with urinary incontinence older adults residing in nursing homes.
RESULTS
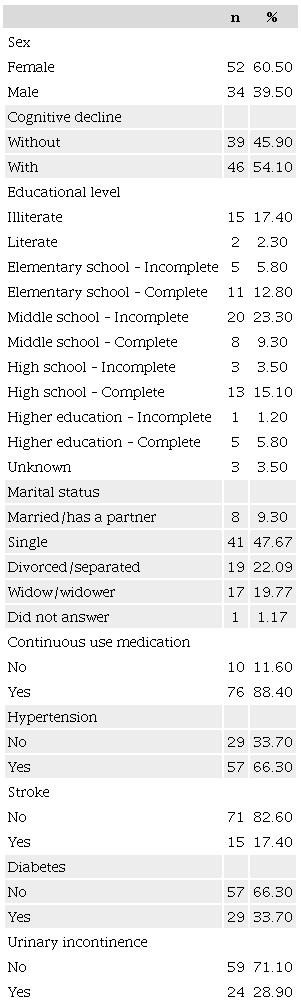
A total of 86 older adults were included in the study. Most of them were women (60.50%), had dropped out of middle school (23.30%), were single (47.70%), and had hypertension (66.30%). The prevalence of self-reported UI in the study population was 28.90% (Table 1).
The sociodemographic and health variables that were associated with UI in older adults living in nursing homes were educational level, limitations in BADLs, depressive symptoms, and number of sleep-related disorders (Table 2). No associations were observed between UI, age group, and sex. As shown in Table 2, regarding health variables and self-reported chronic diseases, there was an association between UI and hypertension, fecal incontinence, and difficulty swallowing. There were no statistically significant associations with the other variables.
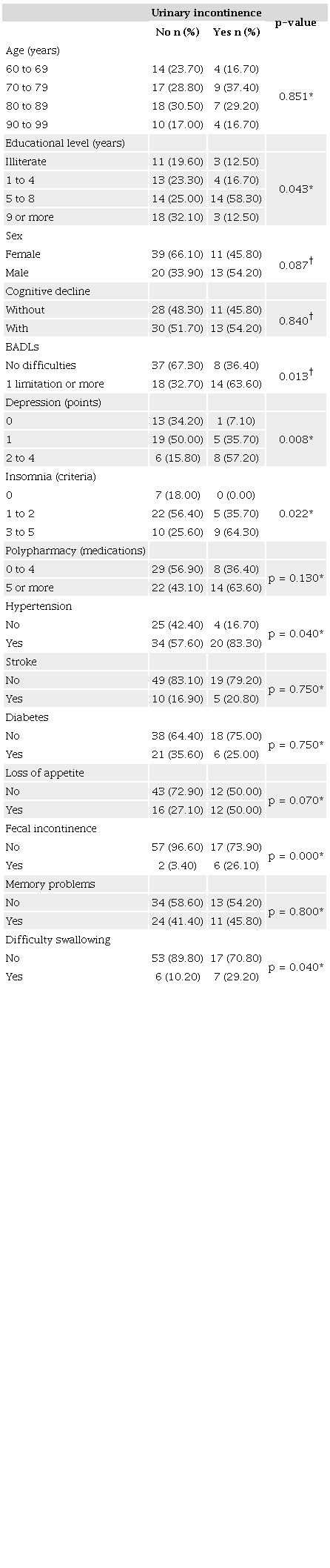
* Fisher’s exact test; † Chi-square test; p<0.05. BADLs: Basic activities of daily living.
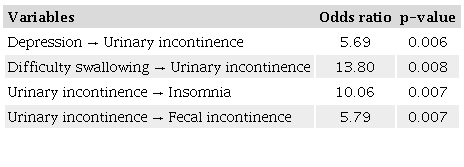
The PA was tested based on the theoretical model proposed in Figure 1. After estimation and respecification of the theoretical model, the education, hypertension, and BADL variables, as well as the direct path from depression to insomnia, were excluded, as they were not statistically significant. Figure 2 shows the representation of the final model after the adjustments, with the relationships and regression coefficients between the variables. Depression and difficulty swallowing had a direct and significant effect on UI, and UI had a direct and significant effect on insomnia and fecal incontinence.
Table 3 shows the exponentiated regression coefficients (odds ratio [OR]). The OR of having UI versus not having it was 5.7 times higher in older adults with depression than in those without depression, and 13.8 times higher in older adults with difficulty swallowing than in those without it. In addition, in older adults with UI, the OR of having insomnia was 5.8 times higher than not having it, and the OR of having fecal incontinence was 10 times higher than not having it. Mediation analysis of the variables was not statistically significant; thus, no indirect associations were found in the tested model.
DISCUSSION
In the present study, there was a higher prevalence of UI in participants who had dropped out of middle school, were hypertensive, had limitations in BADLs, insomnia, difficulty swallowing, fecal incontinence, and a greater number of depressive symptoms. In the PA, an exploratory model that determines the relationships between variables and the way they affect each other through the flow of variables, depression and difficulty swallowing were significantly associated with UI, and UI was directly associated with insomnia and fecal incontinence. These findings suggest that UI in older adults living in nursing homes is a complex problem that requires assessment, prevention, treatment, and rehabilitation in Brazilian nursing homes.
Based on the data presented, it is not possible to establish cause-and-effect relationships, only associations. Therefore, the data is exploratory and based on a small, nonprobabilistic sample, which does not allow generalizations. Conducting a study with older adults living in nursing homes in Brazil is challenging for several reasons: obtaining research authorization from institutions; securing funding to conduct the research; ensuring the availability of the teams to assist researchers and the availability of participants; using instruments with high sensitivity to correctly assess the health conditions of older adults living in nursing homes; and establishing evaluation schedules that do not disrupt the activities of the institutions. In addition, the Covid-19 pandemic significantly impacted the conduct of this study. For all these reasons, the study represents the collaborative efforts of the research team to describe exploratory data on UI.
Some of our findings were similar to those of Carneiro et al.19A higher prevalence of UI was observed in high school dropouts in both studies. This can be explained by the fact that those with higher educational levels have greater knowledge of risks and basic health care, especially prophylactic care, as well as higher income, which could be a protective factor against their admission to public or philanthropic institutions. However, contrary to Carneiro et al.,19 we did not observe an association between sex and UI, probably because of sample characteristics that should be better investigated.
In addition, hypertensive participants were identified as the group most affected by UI. Several studies attribute this finding to the medication of choice in the treatment of hypertension. Thiazide diuretics are commonly recommended for older adults undergoing drug treatment. Their use can trigger urinary symptoms, such as frequent or urgent urination. In our sample, the use of diuretics was highly prevalent in hypertensive participants, which may have increased the rates of UI in this group. However, it is important to consider the impact of diuretic use in conjunction with other chronic diseases and the potential interaction with other medications, as this could enhance the effects of diuretics.
Some limitations in BADLs were identified in the group of older adults with UI.20 A previous study described limitations in BADLs as a criterion of physical frailty, in which UI associated with limitations in BADLs is related to reduced social interaction and sexual life.7 Furthermore, Huion et al. observed significant differences between dependent and independent older adults regarding UI.5 Dependent individuals lost a large amount of urine daily, while independent individuals lost tiny amounts, such as drops and splashes, 3 to 4 times a month.
Depressive symptoms were identified in those with UI. Guimarães et al. also found a significant association between depressive symptoms and UI.8 The authors showed that UI leads to social isolation, driven by feelings of incapacity. In the present study, the unidirectional relationship between depressive symptoms and UI observed in the PA should be further explored, especially regarding the pathophysiological pathways shared between the two conditions and the influence of external variables that were not investigated.
Sleep-related disorders were more frequent in older adults with UI. As reported by other studies, this is due to urge incontinence and nocturia.21 In our study, according to the PA, sleep disorders were directly associated with UI, suggesting that these disorders could be prevented in older adults living in nursing homes by treating UI.
The association between UI and fecal incontinence is a noteworthy finding, as it may contribute to worsening quality of life and nutritional status.22 According to Ribeiro et al.,23 the combination of chronic diseases with the excessive use of medications to treat them has been shown to cause double incontinence.23 This theory is further supported by the pathophysiological similarities between both conditions. Another hypothesis is related to the pelvic apparatus and the muscles that control the urogenital and anal region. Managing such cases is challenging due to dementia and mobility restrictions.23 This type of associated disorder is relevant and requires great care.
Difficulty swallowing was also associated with UI, probably because of the similarity in autonomic fibers present in both the gastrointestinal and genitourinary tracts, both of which have smooth muscles.24,25 Therefore, when UI is related to neurological injuries, it may be associated with swallowing disorders.
Although our findings are in line with the literature, we used a self-report questionnaire to evaluate the presence of UI and excluded participants with sensory and communication disorders. It is possible that the prevalence of UI could be higher in a more comprehensive sample. Nevertheless, our findings remain relevant given the extensive collection and investigation of functionality and health variables in Brazilian older adults. Additionally, the presentation of a PA improves our understanding of the relationships between these variables.
Finally, future studies with a nationally representative, robust sample including both public and private institutions would significantly contribute to this topic. Achieving this requires a collaborative effort from researchers in the aging field, as well as support from funding bodies and agencies. Currently, studies involving Brazilian older adults residing in nursing homes are limited in scale and receive inadequate investment.
CONCLUSION
UI is a clinical condition associated with sociodemographic factors, mood, functional performance, and health conditions. Integrated actions of prevention, recovery, and promotion of health are necessary, with a focus on the functional, clinical, and mental health aspects of older adults living in nursing homes. This is one of a small number of studies on the population living in public nursing homes in Brazil, and it suggests that the prevalence of UI (and its associations) is very similar to that of nursing homes in other countries. This could positively impact public policies.
ACKNOWLEDGEMENTS
We would like to thank the research team, as well as the Conselho Nacional de Desenvolvimento Científico e Tecnológico for funding the research and Brazilian older people for participating in the study.
REFERENCES
Jachan DE, Müller-Werdan U, Lahmann NA. Impaired mobility and urinary incontinence in nursing home residents: a multicenter study. J Wound Ostomy Continence Nurs. 2019;46(6):524-9. https://doi.org/10.1097/WON.0000000000000580
Soler R, Gomes CM, Averbeck MA, Koyama M. The prevalence of lower urinary tract symptoms (LUTS) in Brazil: Results from the epidemiology of LUTS (Brazil LUTS) study. Neurourol Urodyn. 2018;37(4):1356-64. https://doi.org/10.1002/nau.23446
Reis RB, Cologna AJ, Martins ACP, Paschoalin EL, Tucci Jr S, Suaid HJ. Incontinência urinária no idoso. Acta Cir Bras. 2003;18(suppl 5):47-51. https://doi.org/10.1590/S0102-86502003001200018
Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U, et al. The standardisation of terminology of lower urinary tract function: report from the standardisation sub-committee of the International Continence Society. Am J Obstet Gynecol. 2002;187(1):116-26. https://doi.org/10.1067/mob.2002.125704
Huion A, De Witte N, Everaert K, Halfens RJG, Schols JMGA. Care dependency and management of urinary incontinence in nursing homes: a descriptive study. J Adv Nurs. 2021;77(4):1731-40. https://doi.org/10.1111/jan.14702
Marques LM. Prevalência e fatores associados à incontinência urinária em idosos residentes na comunidade. Ouro Preto: Universidade Federal de Minas Gerais; 2005.
Tai H, Liu S, Wang H, Tan H. Determinants of urinary incontinence and subtypes among the elderly in nursing homes. Front Public Health. 2021;9:788642. https://doi.org/10.3389/fpubh.2021.788642
Guimarães LA, Brito TA, Pithon KR, Jesus CS, Souto CS, Souza SJN, et al. Sintomas depressivos e fatores associados em idosos residentes em instituição de longa permanência. Ciênc Saúde Coletiva. 2019;24(9):3275-82. https://doi.org/10.1590/1413-81232018249.30942017
Huang P, Luo K, Wang C, Guo D, Wang S, Jiang Y, et al. Urinary incontinence is associated with increased all-cause mortality in older nursing home residents: a metaanalysis. J Nurs Scholarsh. 2021;53(5):561-7. https://doi.org/10.1111/jnu.12671
Klem L. Path analysis. In: Grimm LG, Yarnold PR, eds. Reading and understanding multivariate statistics. Washington: American Psychological Association, 1995. p. 65-97.
Brucki SMD, Nitrini R, Caramelli P, Bertolucci PHF, Okamoto IH. Sugestões para o uso do mini-exame do estado mental no Brasil. Arq Neuropsiquiatr. 2003;61(3B):777-81. https://doi.org/10.1590/S0004-282X2003000500014
Bertolucci PHF, Brucki SMD, Campacci SR, Juliano Y. O Mini-Exame do Estado Mental em uma população geral: impacto da escolaridade. Arq Neuropsiquiatr. 1994;52(1):1-7. https://doi.org/10.1590/S0004-282X1994000100001
Almeida O P, Almeida SA. Confiabilidade da versão brasileira da Escala de Depressão em Geriatria (GDS) versão reduzida. Arq Neuropsiquiatr. 1999;57(2B):421-6. https://doi.org/10.1590/S0004-282X1999000300013
Yesavage JA, Brink TL Rose TL et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiat Res 1983;17:37-49.
Castelo MS, Coelho Filho JM, Siqueira Neto JI et al Escala de Depressão Geriátrica com quatro itens: um instrumento válido para rastrear depressão em idosos em nível primário de saúde. Revista Brasileira de Geriatria e Gerontologia, 2007; 1:28-33.
Duarte YAO, Andrade CL, Lebrão ML. O Índex de Katz na avaliação da funcionalidade dos idosos. Rev Esc Enferm USP. 2007;41(2):317-25. https://doi.org/10.1590/S0080-62342007000200021
Lino VTS, Pereira SRM, Camacho LAB, Ribeiro Filho ST, Buksman S. Adaptação transcultural da Escala de Independência em Atividades da Vida Diária (Escala de Katz). Cad Saúde Pública. 2008;24(1):103-12. https://doi.org/10.1590/S0102-311X2008000100010
Teixeira-Salmela LF, Magalhães LC, Souza AC, Lima MC, Lima RCM, Goulart F. Adaptação do Perfil de Saúde de Nottingham: um instrumento simples de avaliação da qualidade de vida. Cad Saúde Pública. 2004;20(4):905-14. https://doi.org/10.1590/S0102-311X2004000400004
Carneiro JA, Ramos GCF, Barbosa ATF, Medeiros SM, Lima CA, Costa FM, et al. Prevalência e fatores associados à incontinência urinária em idosos não institucionalizados. Cad Saúde Coletiva. 2017;25(3):268-77. https://doi.org/10.1590/1414-462X201700030295
Soares MFN, Maia LC, Costa SM, Caldeira AP. Functional dependence among older adults receiving care from Family Health Strategy teams. Rev Bras Geriatr Gerontol. 2019;22(5):e190147. https://doi.org/10.1590/1981-22562019022.190147
Bicalho MB, Lopes MHBM. The impact of urinary incontinence of the lives of wives of men with incontinence: an integrative review. Rev Esc Enferm USP. 2012;46(4):1009-14. https://doi.org/10.1590/s0080-62342012000400032
Rose A, Thimme A, Halfar C, Nehen HG, Rübben H. Severity of urinary incontinence of nursing home residents correlates with malnutrition, dementia and loss of mobility. Urol Int. 2013;91(2):165-9. https://doi.org/10.1159/000348344
Ribeiro DC, Souza JRN, Zatti RA, Dini TR, Moraes JR, Faria CA. Double incontinence: associated factors and impact on the quality of life of women attended at a health referral service. Rev Bras Geriatr Gerontol. 2019;22(6):e190216. https://doi.org/10.1590/1981-22562019022.190216
Leung FW, Schnelle JF. Urinary and fecal incontinence in nursing home residents. Gastroenterol Clin North Am. 2008;37(3):697-707. https://doi.org/10.1016/j.gtc.2008.06.005
Rocha EA, Mehta N, Távora-Mehta MZP, Roncari CF, Cidrão AAL, Elias Neto J. Disautonomia: uma condição esquecida – parte II. Arq Bras Cardiol. 2021;116(5):981-98. https://doi.org/10.36660/abc.20200422
Notes
This study was supported by Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) — MCTIC/CNPq (420859/2018-7) and by the Undergraduate Research Program of the Catholic University of Brasília.
The study was approved by the Research Ethics Committee of the Federal University of Bahia (CAAE: 18561419.5.1001.5023, assessment number: 3.793.529) and the Catholic University of Brasília (CAAE: 18151019.1.1001.0029, assessment number: 3.621.190).
The authors did not report using standards guidelines (STROBE).
Author notes
Correspondence data Henrique Salmazo da Silva – QS 7, LT 01, sala S009 – Águas Claras – CEP: 71966-700 – Brasília (DF), Brazil. E-mail: henriquesalmazo@yahoo.com.br
Conflict of interest declaration
The authors declare no conflicts of interest.