ORIGINAL ARTICLE
Received: 10 December 2023
Accepted: 01 February 2024
DOI: https://doi.org/10.53886/gga.e0000110_EN
Abstract
Objective: To analyze the impact of intrinsic capacity on 30-month mortality among older adults living in long-term care facilities (LTCFs).
Methods: Prospective cohort study with survival analysis conducted from July 2020 to December 2022 among older adults living in Brazilian LTCFs. At baseline (T0), 209 older residents were evaluated for demographic profile, clinical data (diagnosed diseases and current medications), intrinsic capacity according to ICOPE (cognitive capacity, psychological capacity, hearing capacity, visual capacity, vitality, and locomotor capacity domains), functional capacity (Katz Index of Independence in Activities of Daily Living), and frailty (FRAIL scale). At 30 months, mortality in the sample was assessed.
Results: At T0, the mean age of residents was 82 (SD, 11.21) years; 65.07% were female, 94.26% were white, and 88.04% had multimorbidity. Overall, 54.07% (n = 113) of residents exhibited changes in four or more domains of intrinsic capacity, with locomotor capacity being the most commonly impaired domain (82.78%); 43.54% were completely dependent for basic activities of daily living, and 42.58% were frail. At 30-month follow-up, 33.49% (n = 70) of residents had died. Survival analysis revealed a statistically significant association between death and impairment in four or more domains of intrinsic capacity (p = 0.044).
Conclusion: Impairment in four or more domains of intrinsic capacity is associated with death in LTCF residents.
Keywords: Aged, aging, frailty, homes for the aged.
Resumo
Objetivo: Analisar o efeito da Capacidade Intrínseca na mortalidade de 30 meses em residentes idosos de Instituição de Longa Permanência.
Metodologia: Estudo de coorte prospectivo realizado de julho de 2020 a dezembro de 2022 com análise de sobrevivência de idosos residentes de ILPIs brasileiras. Na avaliação inicial (MO) foram avaliados 209 idosos residentes quanto aos dados demográficos e clínicos (doenças diagnosticadas e medicações utilizadas); capacidade intrínseca segundo ICOPE nos domínios cognição, psicológico, audição, visão, vitalidade e locomotor; capacidade funcional pelas atividades básicas de vida diária (índice de Katz) e fragilidade (escala FRAIL). Após 30 meses, foi avaliada a ocorrência de óbito.
Resultados: Em MO, a média da idade dos residentes era de 82 anos (±11,21), 65,07% eram do sexo feminino, 94,26% de cor branca e 88,04% tinham multimorbidade. Apresentaram alteração em quatro ou mais domínios da capacidade intrínseca 54,07% (n = 113) dos residentes, sendo o domínio mais alterado a locomoção (82,78%). Eram totalmente dependentes para as atividades básicas de vida diária 43,54% dos idosos, e 42,58% eram frágeis. Após 30 meses de acompanhamento, 33,49% (n = 70) dos idosos evoluíram para óbito. Na análise da sobrevida para óbito, houve associação estatisticamente significativa do evento com alteração em quatro ou mais domínios da capacidade intrínseca (p = 0,044).
Conclusão: a alteração de quatro ou mais domínios da capacidade intrínseca está associada com óbito em residentes de ILPI.
Palavras-Chaves: Idoso, envelhecimento, fragilidade, instituição de longa permanência para idosos.
INTRODUCTION
As the population ages, a growing number of older adults will live with chronic noncommunicable diseases, dependence for basic activities of daily living (BADLs), and disabilities.1, 2 A Brazilian multicenter study showed that 23.2% of older adults reported difficulty with at least one BADL.3
Long-term care facilities (LTCFs) have emerged as a source of non-family care for older adults with greater functional dependence, a population which requires extended care. These are defined by the Brazilian National Health Surveillance Agency as “residential institutions intended for the collective housing of people aged 60 years or over, with or without family support, under conditions of freedom, dignity, and citizenship”.4
Residents of LTCFs are characterized by multimorbidity of chronic noncommunicable diseases, functional incapacity, and frailty.5
The World Health Organization (WHO) has published guidelines for the use of a screening tool for intrinsic capacity, defined as “the composite of all the physical and mental capacities that an individual can draw on”, consisting of six domains (locomotor capacity, vitality, visual capacity, hearing capacity, cognitive capacity, and psychological capacity). This tool, Integrated Care for Older People (ICOPE), was designed to assess older adults in primary-care settings.6, 7 The interactions between one’s intrinsic capacity and the environment in which one lives make up functional ability, defined as “the health-related attributes that enable people to be and to do what they have reason to value”.
The ICOPE screening tool assesses the six aforementioned domains; instruments have also been defined for monitoring the loss of intrinsic capacity and for implementing the ICOPE strategy in each country.8
Studies that used the ICOPE to assess intrinsic capacity in LTCF residents have found an association between mortality and impairment in the vitality domain,9 as well as an association of loss of intrinsic capacity with reduced function.10
The objective of this study was to analyze ICOPE-defined intrinsic capacity among institutionalized older adults in the state of São Paulo, Brazil, and its association with mortality.
METHODS
Longitudinal observational cohort study with survival analysis conducted from July 2020 to December 2022. In July 2020, 209 older adults living in 15 LTCFs in a city in the state of São Paulo, Brazil, underwent baseline assessment (T0).
The inclusion criteria were individuals of either sex, aged 60 years or older, who had lived in an LTCF for longer than 30 days and agreed to participate in the study voluntarily (or via authorization obtained from their health care proxy). The exclusion criteria were older adults who were unable to carry on a conversation and did not have an informant who could assist the investigators in obtaining demographic and clinical data; or refusal to participate (by the resident themselves or their proxy).
At baseline (T0), demographic and clinical data (diagnosed diseases and current medications) were collected from the LTCF medical record or obtained from the resident or caregiver.
Intrinsic capacity was assessed according to the ICOPE guidelines in the following domains:7
- 1. Cognitive capacity: cognitive decline was defined by a previous diagnosis of dementia of any etiology or by abnormalities on cognitive assessment. Participants were asked to remember three words (flower, door, rice). Next, orientation in time and space was assessed with the questions “What is the full date today?” and “Where are you now?”. Participants were then asked, “Do you recall the three words?”. If they made mistakes, were unable to answer any of the questions asked, or were unable to recall the three words, the cognitive domain was considered impaired.
- 2. Psychological capacity: participants were asked: “Over the past two weeks, have you been bothered by feeling down, depressed, or hopeless, or have you had little interest or pleasure in doing things?”. If they answered “yes” to either question, this domain was considered impaired.
- 3. Sensory – Visual impairment: participants were asked if they had any difficulties in watching television or reading. If they answered “yes” to either question, this domain was considered impaired.
- 4. Sensory – Hearing loss: a whisper test was performed.11 If the test was positive for either ear, this domain was considered impaired.
- 5. Vitality (malnutrition): participants were asked if they had unintentionally lost more than 4.5 kg (or 5% of their body weight) over the last 6 months or if they had experienced loss of appetite. If they answered “yes” to either question, this domain was considered impaired.
- 6. Locomotor capacity: the Timed Up and Go Test (TUGT) was performed. A time > 13.5 s was considered indicative of impairment.12
Functional capacity was assessed with the Katz Index of Independence in Activities of Daily Living.13 Ability to transfer from bed to chair, maintain continence, maintain personal hygiene, bathe, dress, and eat were assessed. One point was scored for each activity the participant was able to complete independently. They were then classified as independent (5 or 6 points), partially dependent (3 or 4), or dependent (0, 1 or 2) for BADLs.
The frailty syndrome was assessed using the FRAIL scale.14 The following aspects were evaluated: Fatigue (“Are you fatigued?”); Resistance (“Cannot walk up one flight of stairs?”); Aerobic (“Cannot walk one block?”); Illnesses (“Do you have more than 5 illnesses?” The illnesses considered for the scale are: hypertension; diabetes mellitus; cancer, other than squamous/basal cell carcinoma of the skin; congestive heart failure; coronary artery disease or acute myocardial infarction; chronic obstructive pulmonary disease or asthma; arthritis; stroke, chronic kidney disease); and Loss of weight (“Have you lost more than 5% of your weight in the past 6 months?”). Participants were then classified as frail (3 or more points) or nonfrail (0 to 2).
Polypharmacy was defined as taking five or more medications, while multimorbidity was defined as the presence of two or more diagnosed or reported diseases.15
Deaths occurring over the 30-month period from baseline assessment until December 2022 were recorded. Data were obtained from the LTCF and/or the municipal funeral service.
A descriptive analysis of the data was then conducted.
The accuracy of impairment in four or more domains of intrinsic capacity to independently predict 30-month mortality was assessed using Kaplan-Meier cumulative survival curves and the log-rank test for two categories (loss vs. no loss of intrinsic capacity).
The project and its Informed Consent Form were approved by the Research Ethics Committee of Faculdade de Medicina de Botucatu – Unesp (opinion number 4 640 571).
RESULTS
A total of 209 residents of 15 LTCFs were evaluated, of whom 65.07% were female and 94.26% were white. They had a mean age of 82 (SD, 11.21) years, 4 (SD, 1.62) diagnosed diseases, and were on 5 (SD, 2.11) medications for regular use. The most prevalent diseases were heart disease (49.28%), hypertension (41.15%), and dementia syndromes (39.71%). Overall, 88.04% of participants had multimorbidity and 59.81% had polypharmacy (Table 1).
Clinical and demographic profile of residents of long-term care facilities for older adults, 2023. n = 209.
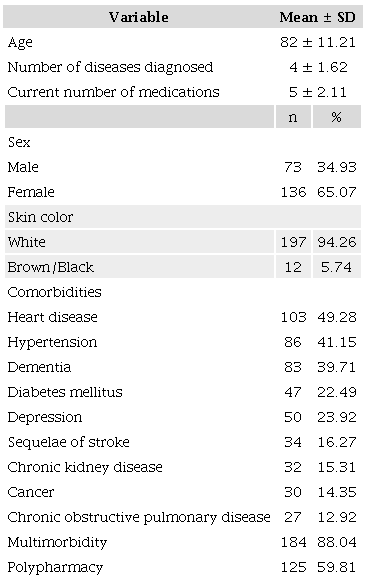
SD: standard deviation.
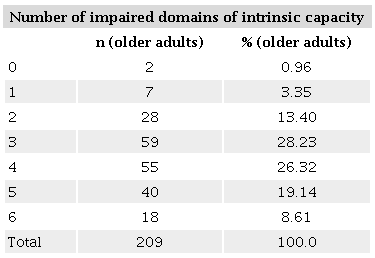
Of the 209 participants, 99.04% showed impairment in at least one domain of intrinsic capacity, and 54.07% (n = 113) in four or more domains. Changes in locomotor capacity (82.78%), psychological capacity (61.72%), visual capacity, and cognitive capacity (58.37% each) were most prevalent (Table 2).
Intrinsic capacity performance of residents of long-term care facilities for older adults, 2023. n = 209.
Regarding functional capacity, 43.54% of the participants were completely dependent for BADLs, with only 30.14% being independent. Just over half (50.23%) of the participants were dependent for three or more BADLs. Regarding frailty, 42.58% of the participants were frail.
During the 30 months of follow-up, data were obtained from all 209 residents evaluated at T0; of these, 33.49% (n = 70) died. The mean age at death was 83.04 (SD, 10.19) years, and the mean time to death was 332.30 (SD, 243.39) days.
Survival analysis revealed a statistically significant association between impairment in 4 or more domains of intrinsic capacity and death (p = 0.044; log-rank 4.06) (Figure 1).
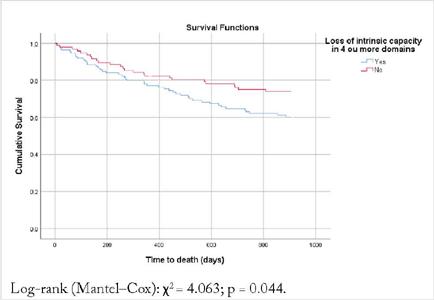
FIGURE 1
Kaplan–Meier curve of time to death, stratified by loss of intrinsic capacity, among residents of long-term care facilities for older adults, 2023. n = 209.
DISCUSSION
This study, to the best of our knowledge, is the first to evaluate intrinsic capacity using the ICOPE screening tool in LTCF residents in Brazil. We found that impairment in four or more ICOPE domains was associated with death within 30 months.
The ICOPE guidelines recommend first conducting a rapid assessment of the intrinsic capacity domains.16 If any domain screens abnormal, further examination at a later date is advised. This guideline was devised by the World Health Organization with the core objective of preventing, slowing, or reversing the declines that accompany aging. Studies conducted with community-dwelling older adults have described how to perform this first step.16, 17 However, there is a lack of information in other elder-care settings, such as hospital environments and LTCFs. Few published studies have evaluated intrinsic capacity in LTCF residents.9, 10
Older adults living in such facilities are characterized by female gender, very advanced age, frailty, and dependence for BADLs, as reported in other studies.9, 18 Multimorbidity has also been reported as particularly prevalent in this care setting.19 These demographic and clinical findings were corroborated in the population we evaluated and are consistent with previous work done by our group.5, 20
We observed a mortality rate of 33.49% at 30 months. This finding is similar to that of a study conducted in an LTCF in Belgium, which reported a mortality rate of 38.2% over 3 years.9 This high number of deaths can be explained by the clinical profile of this institutionalized population, which, as noted above, is characterized by multimorbidity, frailty, and functional dependence.5
When evaluating intrinsic capacity, we found the most affected domains to be locomotor, psychological, cognitive, and visual; this is consistent with a Mexican study of people over the age of 50 living in the community, in which the most commonly impaired domains were mobility, visual, and psychological.16 In the Mexico study, 87.8% of the population aged 50 or over had impairment of at least one domain, a prevalence that exceeded 90% in the group aged over 80. In our sample, almost all LTCF residents had at least one domain affected.
A study of LTCF residents in France, which found a mortality rate of 15.4% over 12 months of follow-up, showed that older adults who performed better on an intrinsic capacity composite score had lower risk of death.10 The authors observed that the absence of cognitive impairment was associated with lower odds of hospitalization, and better performance in the vitality domain, with a lower risk of mortality. The data presented by Sánchez-Sánchez et al.10 regarding risk of death are similar to those found in our study, in which worse performance on intrinsic capacity domains was associated with mortality.
Data from the Belgian SarcoPhAge cohort study, which followed 534 community-dwelling older adults, found a mortality rate of 29.4% after 10 years.21 Poor intrinsic capacity in the locomotor or psychological domains predicted a 2-to-3.5-fold higher mortality risk. These findings show that impairment in domains of intrinsic capacity can predict risk of death, both in the community and in residents of LTCFs.
One aspect not evaluated in the present study was the preservation of intrinsic capacity, which in community-dwelling older adults is associated with better performance in functional capacity domains.22, 23
Early identification of LTCF residents at risk of experiencing adverse health events is essential. Detection of changes in intrinsic capacity domains – even with screening tools – and the implementation of personalized interventions can improve the quality of care for older adults, even in institutional settings. In this context, the assessment of intrinsic capacity not only allows the care team to implement necessary interventions but also to ensure follow-up.
Limitations of our study include that part of the data collection was conducted during the COVID-19 pandemic, in which there was a recommendation to limit access to LTCFs.24 Despite the pandemic, of the 70 deaths we recorded, only three were due to SARS-CoV-2 infection. Another limitation is that our cohort may not be representative of the general population of LTCF residents in Brazil, due to the large regional differences observed across the country.25
Our study has several strengths, particularly its novelty, the inclusion of all domains of intrinsic capacity proposed by the WHO, the long follow-up period (30 months), and the fact that the individuals were followed within the LTCF setting.
CONCLUSION
In the present study of older adults living in LTCFs, almost all showed impairment in some domain of intrinsic capacity. Poor intrinsic capacity performance (impairment in four or more domains) was associated with mortality. Assessment of intrinsic capacity by the ICOPE screening tool in LTCFs allows rapid, wide-ranging detection of residents at risk.
Our findings require validation by further research. Additional studies are needed to replicate these results in other LTCF cohorts.
ACKNOWLEDGEMENTS
The authors would like to acknowledge and thank all long-term care facilities which contributed to this study by sharing information.
REFERENCES
Veras R. Envelhecimento populacional contemporâneo: demandas, desafios e inovações. Rev Saúde Pública. 2009;43(3):548-54. https://doi.org/10.1590/S0034-89102009005000025
Nunes BP, Batista SRR, Andrade FB, Souza Junior PRB, Lima-Costa MF, Facchini LA. Multimorbidade em indivíduos com 50 anos ou mais de idade: ELSI-Brasil. Rev Saúde Pública. 2018;52(Suppl 2):10s. https://doi.org/10.11606/s1518-8787.2018052000637
Giacomin KC, Duarte YAO, Camarano AA, Nunes DP, Fernandes D. Cuidado e limitações funcionais em atividades cotidianas – ELSI-Brasil. Rev Saúde Pública 52(Suppl 2), 9s. https://doi.org/10.11606/s1518-8787.2018052000650
Brasil. Ministério da Saúde. Agência Nacional de Vigilância Sanitária. Resolução de Diretoria Colegiada - RDC nº 502, de 27 de maio de 2021. Dispõe sobre o funcionamento de Instituição de Longa Permanência para Idosos, de caráter residencial. Available from: https://bvsms.saude.gov.br/bvs/saudelegis/anvisa/2020/rdc0502_27_05_2021.pdf. Accessed Aug 5, 2023.
Fonseca ARB, Silva PS, Carvalho TC, Arrage MA, Duarte SRS, Selegatto ALS, et al. Frailty and mortality in long-term care facilities for older people in Brazil: a survival analysis. Geriatr Gerontol Aging. 2021;15:e0210057. https://doi.org/10.53886/gga.e0210057
World Health Organization. Integrated care for older people: guidelines on community-level interventions to manage declines in intrinsic capacity. Geneva: World Health Organization; 2017. Available from: https://apps.who.int/iris/handle/10665/258981. Accessed Aug 13, 2023.
World Health Organization. Guidance for person-centred assessment and pathways in primary care. World Health Organization; 2019. Available from: https://apps.who.int/iris/bitstream/handle/10665/326843/WHO-FWC-ALC-19.1-eng.pdf?sequence=17&isAllowed=y. Accessed Aug 13, 2023.
Ferriolli E, Lourenço RA, Oliveira VP, Mello RGB, Ferretti-Rebustini REL, Jacob Filho W. Project ICOPE Brazil: a study on the intrinsic capacity of Brazilian older adults and accuracy of the screening tool proposed by the World Health Organization. Geriatr Gerontol Aging. 2023;17:e0230003. https://doi.org/10.53886/gga.e0230003
Charles A, Buckinx F, Locquet M, Reginster JY, Petermans J, Gruslin B, et al. Prediction of adverse outcomes in nursing home residents according to intrinsic capacity proposed by the World Health Organization. J Gerontol A Biol Sci Med Sci. 2020;75(8):1594-9. https://doi.org/10.1093/gerona/glz218
Sánchez-Sánchez JL, Rolland Y, Cesari M, Barreto PS. Associations Between intrinsic capacity and adverse events among nursing home residents: the INCUR study. J Am Med Dir Assoc. 2022;23(5):872-876.e4. https://doi.org/10.1016/j.jamda.2021.08.035
Reuben DB, Tinetti ME. Goal-oriented patient care--an alternative health outcomes paradigm. N Engl J Med. 2012;366(9):777-9. https://doi.org/10.1056/NEJMp1113631
Panel on Prevention of Falls in Older Persons, American Geriatrics Society and British Geriatrics Society. Summary of the updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J Am Geriatr Soc. 2011;59(1):148-57. https://doi.org/10.1111/j.1532-5415.2010.03234.x
Duarte YAO, Andrade CL, Lebrão ML. Katz index on elderly functionality evaluation. Rev Esc Enferm USP. 2007;41(2):317-25. https://doi.org/10.1590/s0080-62342007000200021
Aprahamian I, Cezar NOC, Izbicki R, Lin SM, Paulo DLV, Fattori A, et al. Screening for frailty with the FRAIL scale: a comparison with the phenotype criteria. J Am Med Dir Assoc. 2017;18(7):592-6. https://doi.org/10.1016/j.jamda.2017.01.009
Carvalho MFC, Romano-Lieber NS, Bergsten-Mendes G, Secoli SR, Ribeiro E, Lebrão ML, et al. Polifarmácia entre idosos do Município de São Paulo - Estudo SABE. Rev Bras Epidemiol. 2012;15(4):817-27. https://doi.org/10.1590/s1415-790x2012000400013
Gutiérrez-Robledo LM, García-Chanes RE, Pérez-Zepeda MU. Screening intrinsic capacity and its epidemiological characterization: a secondary analysis of the Mexican health and aging study. Rev Panam Salud Publica. 2021;45:e121. https://doi.org/10.26633/RPSP.2021.121
González-Bautista E, Souto Barreto P, Virecoulon Giudici K, Andrieu S, Rolland Y, Vellas B. Frequency of conditions associated with declines in intrinsic capacity according to a screening tool in the context of integrated care for older people. J Frailty Aging. 2021;10(2):94-102. https://doi.org/10.14283/jfa.2020.42
Vossius C, Selbæk G, Benth JS, Bergh S. Mortality in nursing home residents: a longitudinal study over three years. PLoS One. 2018;13(9):e0203480. https://doi.org/10.1371/journal.pone.0203480
Kemenesi G, Kornya L, Tóth GE, Kurucz K, Zeghbib S, Somogyi BA, et al. Nursing homes and the elderly regarding the COVID-19 pandemic: situation report from Hungary. Geroscience. 2020;42(4):1093-9. https://doi.org/10.1007/s11357-020-00195-z
Barros ENC, Valle AP, Braga PE, Viscondi JYK, Fonseca ARB, Vanni T, et al. COVID-19 in long-term care facilities in Brazil: serological survey in a post-outbreak setting. Rev Inst Med Trop São Paulo. 2020;63:e10. https://doi.org/10.1590/S1678-9946202163010
Sanchez-Rodriguez D, Demonceau C, Bruyère O, Cavalier E, Reginster JY, Beaudart C. Intrinsic capacity and risk of death: Focus on the impact of using different diagnostic criteria for the nutritional domain. Maturitas. 2023;176:107817. https://doi.org/10.1016/j.maturitas.2023.107817
Aliberti MJR, Bertola L, Szlejf C, Oliveira D, Piovezan RD, Cesari M, et al. Validating intrinsic capacity to measure healthy aging in an upper middle-income country: findings from the ELSI-Brazil. Lancet Reg Health Am. 2022;12:100284. https://doi.org/10.1016/j.lana.2022.100284
Beard JR, Si Y, Liu Z, Chenoweth L, Hanewald K. Intrinsic capacity: validation of a new WHO concept for healthy aging in a longitudinal Chinese study. J Gerontol A Biol Sci Med Sci. 2022;77(1):94-100. https://doi.org/10.1093/gerona/glab226
Villas Boas PJF, Bremenkamp MG, Roriz Filho JS, Kairalla MC, Gomes DCA, Mello RGB, et al. Recommendations for the prevention and control of coronavirus infections (SARS-CoV-2) in long term care facilities. Geriatr Gerontol Aging. 2020;14(2):134-7. https://doi.org/10.5327/Z2447-2123202020142ESP3
Lacerda TTB, Neves APM, Buarque GLA, Freitas DCCV, Tessarolo MMM, González N, et al. Geospatial panorama of long-term care facilities in Brazil: a portrait of territorial inequalities. Geriatr Gerontol Aging. 2021;15:e0210060. https://doi.org/10.53886/gga.e0210060
Notes
Financial support disclosure statements: Pró-Reitoria de Pesquisa, São Paulo State University — UNESP — PIBIC (grant number 1078/2020)
The study protocol was approved by the Research Ethics Committee of Faculdade de Medicina de Botucatu – Unesp (opinion number 4 640 571).
Author notes
Correspondence data Paulo José Fortes Villas Boas – Rua General Telles, 1519 – CEP: 18602-120 – Botucatu (SP), Brazil. E-mail: paulo.boas@unesp.br
Conflict of interest declaration
The authors declare no conflicts of interest.
