STUDY PROTOCOLS
Effects of multicomponent training on the intrinsic capacity of community-dwelling older adults: quasi-experimental study protocol
Efeitos do treinamento multicomponente na capacidade intrínseca de idosos residentes na comunidade: protocolo de estudo quase-experimental
 Sarah Giulia Bandeira Felipe
Clarissa Biehl Printes
Fabiane de Oliveira Brauner
Douglas Kazutoshi Sato
Sarah Giulia Bandeira Felipe
Clarissa Biehl Printes
Fabiane de Oliveira Brauner
Douglas Kazutoshi Sato
Effects of multicomponent training on the intrinsic capacity of community-dwelling older adults: quasi-experimental study protocol
Geriatrics, Gerontology and Aging, vol. 18, e0000104, 2024
Sociedade Brasileira de Geriatria e Gerontologia, SBGG
Received: 27 November 2023
Revised document received: 22 January 2024
Accepted: 03 January 2024
Abstract
Objective: This is a protocol for assessing the effects of multicomponent exercise on the intrinsic capacity of older adults.
Methods: Older adults (≥ 60 years old) will be selected for a multicomponent training program in Porto Alegre, RS, Brazil to evaluate the 5 domains of intrinsic capacity: vitality (handgrip strength, body mass index, and nutrition) sensory perception (self-reported questions), psychology (the 15-item Geriatric Depression Scale), cognition (the Montreal Cognitive Assessment) and locomotion (the sit-to-stand test and the Timed Up and Go test). The composite intrinsic capacity score will be obtained by summing the domains, with total scores ranging from 0 to 10 points. After 12 weeks of the multicomponent exercise intervention, the participants will be reassessed. Student’s t-test and ANOVA will be used to compare the effects of different types of training on intrinsic capacity. This study was approved by the research ethics committee of the involved institution.
Expected results: After the 12-week multicomponent exercise intervention, we expect scores for composite intrinsic capacity and its domains, especially locomotion, to increase.
Relevance: The risk of dependence, falls, and mortality increases with reduced intrinsic capacity, indicating a need for interventions to limit these negative outcomes. Multicomponent exercise, a simple, widely recommended, and effective strategy with good adherence, is designed to prevent intrinsic capacity decline in older people and improve their health and functionality.
Keywords: Intrinsic capacity+ older adults+ exercise.
Resumo
Objetivo: Protocolo para avaliar os efeitos de exercícios multicomponentes na capacidade intrínseca de idosos.
Metodologia: Pessoas idosas (≥ 60 anos) cadastradas em um programa de treinamento multicomponente de Porto Alegre (RS) serão selecionados para avaliação da capacidade intrínseca nos seus cinco domínios: vitalidade (teste de força de preensão manual (FPM), índice de massa corpórea (IMC) e nutrição) sensorial (perguntas autorrelatadas), psicológico (Escala de Depressão Geriátrica, GDS-15), cognitivo (MoCA teste) e locomotor (teste de sentar e levantar e TUG). A pontuação composta da capacidade intrínseca será realizada por meio da soma dos domínios em escore de 0 a 10 pontos. Ao fim de 12 semanas de intervenção com exercícios multicomponentes, os participantes serão reavaliados. Para comparar os efeitos do treinamento multicomponente na capacidade intrínseca composta e por domínio serão utilizados os testes t de Student e ANOVA para comparar os efeitos de diversos tipos de treinamento. Este estudo foi aprovado pelo Comitê de Ética em Pesquisa sob parecer nº 5.517.315.
Resultados esperados: Ao fim de 12 semanas de intervenção com os exercícios multicomponentes, esperamos um aumento na pontuação composta da capacidade intrínseca e em seus domínios, especialmente o locomotor.
Relevância: O risco de dependência, quedas e mortalidade aumenta com o declínio da capacidade intrínseca, suscitando a necessidade de implementar intervenções para limitar esses desfechos negativos. A prática de exercícios multicomponentes é uma estratégia simples, eficaz, com boa adesão e amplamente recomendada para evitar o declínio da capacidade intrínseca e melhorar a saúde e a funcionalidade das pessoas idosas.
Palavras-Chaves: Capacidade intrínseca, idosos, exercício físico.
INTRODUCTION
In older adult care, preserving functionality is essential, regardless of the patients’ current health status or illnesses. The World Health Organization 1 defines healthy aging as the process of optimizing and maintaining functional capacity, facilitating well-being in old age. This capacity is determined by a combination of intrinsic capacity (IC), environmental characteristics, and the interaction between them. 1
IC is conceptualized as the full range of a person’s physical and mental faculties. 2, 3 It is a multidimensional health indicator analyzed from the perspective of five domains: locomotion capacity (physical movement), 4, 5, 6, 7 sensory perception (vision and hearing), 8, 9 psychology, vitality (energy and balance) 10, 11, 12 and cognition. 6, 13, 14, 15, 16
Previous studies have shown that IC decline is prevalent among older adults, 17, 18 mainly in the locomotion domain. 17 It has also been shown that the risk of dependence, falls, and mortality increases with declining IC. 18, 19, 20 Furthermore, higher IC scores have been associated with a lower risk of one-year mortality and functional dependence among hospitalized older adults. 21
One intervention that effectively manages IC decline is regular exercise. Guidelines for older adults indicate that any type of exercise leads to improved health, and the exertion level should be compatible with individual ability. 22 Exercise programs suggested for this population should combine exercise modalities with aerobic, resistance, flexibility, and balance training, 23 what we call multicomponent exercise.
A clinical trial in Japan found that both aerobic and strength training benefited IC in older adults. 24 Similarly, a Spanish study found that a 12-week multicomponent exercise program improved IC in community-dwelling older adults, especially the locomotion, cognition, and vitality domains.
Although the above-mentioned studies have found effects on individual IC domains and composite IC, they were conducted with older adults with subjective memory problems, 24 mild cognitive impairment, and pre-frailty/frailty, 25 which impedes application of the findings to the general population. Therefore, evidence about multicomponent exercise interventions in all IC domains is still limited, especially in Brazil. As far as we know, this will be the first Brazilian study on multicomponent exercise to involve community-dwelling older adults who are apparently robust and are neither pre-frail nor cognitively impaired.
According to the literature, lifestyle behaviors, including exercise, are strongly associated with IC maintenance. 26, 27, 28 Furthermore, few studies have addressed IC changes over time, and no global IC index has been validated in clinical practice and research, which shows the need for further research into measurement techniques and IC interventions in different settings. 29
The main objective of this protocol is to evaluate the effects of a multicomponent training program on the IC of community-dwelling older adults.
METHODS
This will be a 12-week, time-series, prospective quasi-experimental study, with initial and final assessments, as shown in Figure 1.
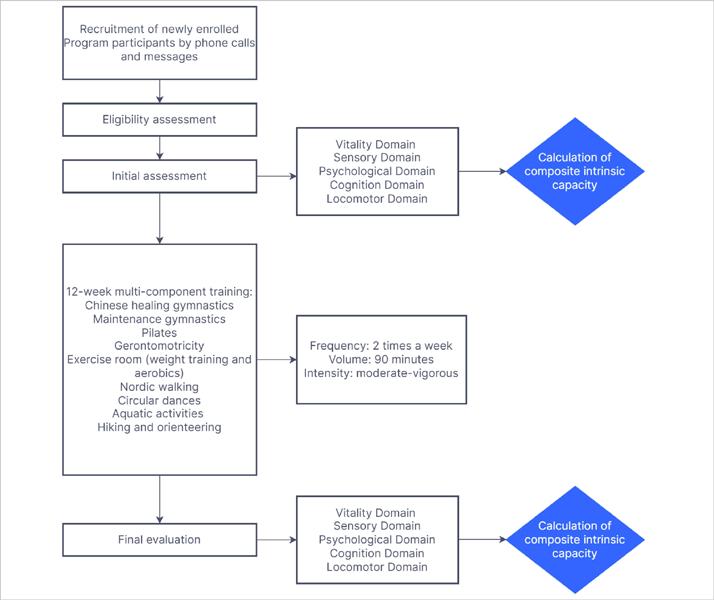
FIGURE 1
Study stage flowchart.
The study will be conducted in the Porto Alegre, Rio Grande do Sul, Brazil.
The non-probabilistic convenience sample will be calculated following Sánchez-Sánchez et al. 25 The sigma value will be the IC difference between the 2 groups (0.48), which with a type I error of 0.05 and a type II error of 20.00% (80.00% statistical power), results in a sample of 24 older adults. However, to minimize possible losses, we will add 30.00% to this figure, resulting in a total of 31 participants.
Participants will be recruited through telephone calls, text messages, social media newsletters, and in person by the research team at the program’s location.
Inclusion criteria
-
Age ≥ 60 years
-
Assessment and reassessment of the 5 domains: cognition, vitality, psychology, locomotion, and sensory perception
-
Program attendance at least twice a week (24 sessions in 12 weeks)
-
Train in 2 modalities for 90 minutes per day
Exclusion criteria
-
Physical or cognitive disabilities that prevent or limit assessment
-
Stroke sequelae
-
Parkinson’s or Alzheimer’s disease
-
History of hand, hip, or knee surgery in the last 12 months
-
≥ 15 absences from the program
Data collection procedures
When entering the program, participants will undergo an orientation in which the team examines the medical certificate and verifies the inclusion criteria, after which the participants provide written informed consent. The initial assessment will then be scheduled, which will consist of a general investigation, collecting sociodemographic and clinical data. The following scales will be applied: the Escala de Depressão Geriátrica (Geriatric Depression Scale), 30 the International Physical
Activity Questionnaire, 31, 32Short Form 6 dimensions, 33 the Escala de Independência Funcional (Functional Independence Scale), 34 and the Montreal Cognitive Assessment.
The following variables will be measured in the physical assessment: weight (kg), height (cm), BMI (kg/m 2), body fat percentage (%), muscle mass (%), visceral fat (%), basal metabolic rate (kcal), body age (years), handgrip strength (kgf) and leg strength (number of repetitions), functional mobility (seconds), abdominal perimeter (cm), waist circumference (cm), thigh circumference ( cm), calf circumference (cm), systolic and diastolic blood pressure (mmHg), heart rate (bpm), flexibility (cm), and balance (seconds). The details of this assessment are shown in the supplementary material ( https://doi.org/10.7910/DVN/UI5SGL).
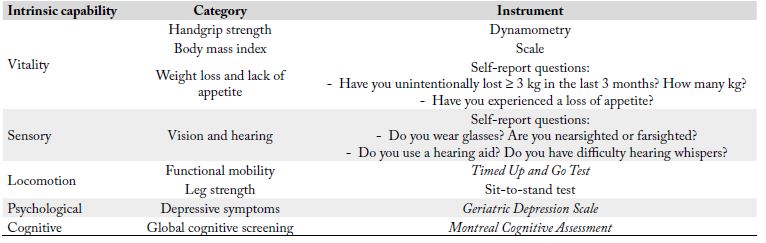
The IC domains will be assessed as shown in Table 1.
Intrinsic capacity calculation
Since there is still no consensus in the literature about total/ composite IC scores consisting of all its dimensions, we decided to use that proposed by López-Ortiz et al., 35 in which the composite IC can range from 0 (worst IC) to 10 (best IC).
Locomotion domain
For the Timed Up and Go test, 36 1 and 0 points will be assigned to results < and > 10 seconds, respectively. For the sit-to-stand test, 34, 37 0 and 1 points will be assigned to repetitions < and ≥ the limit (according to age and sex), respectively. Based on values of 0 or 1 for each variable, the locomotion score will be obtained by adding the results of the Timed Up and Go and sit-to-stand tests, so the final locomotion domain score will vary from 0 to 2.
Vitality domain
BMI values < 22 kg/m 2 and > 27 kg/m 2 will receive a score of 0, while those between 22 and 27 kg/m 2 will receive a score of 1. 38 Regarding handgrip strength, values < 27 kgf for men and 16 kgf for women will receive 0 points, while those ≥ 27 kgf for men and 16 kgf for women will receive 1 point. 39 Weight loss will be scored as follows: 0 points for ≥ 3 kg in the last 3 months, and 1 point < 3 kg or no weight loss. For the appetite loss variable, affirmative and negative answers will receive 0 and 1 points, respectively. Based on the points (0 or 1) for each variable, the vitality score will result from the sum of the BMI, handgrip strength, weight loss, and loss of appetite values. Thus, the final vitality domain score will range from 0 to 4.
Cognition domain
After applying the Montreal Cognitive Assessment, 40, 41 scores below and above the cut-off point will receive 0 and 1 points, respectively, according to education level. Thus, inal scores for the cognition domain will vary between 0 and 1.
Psychology domain
For the Escala de Depressão Geriátrica, 30 scores from 11-15, 6-10, and 0-5, will receive 0, 0.5, and 1 points, respectively. Thus, final scores for the psychological domain will vary from 0 to 1.
Sensory perception domain
This domain will be assessed through self-report questions in 2 categories: vision and hearing. 3 For vision, participants who are nearsighted or farsighted and wear prescription glasses will receive 0 points, and those who are/do not will receive 1 point. For hearing, those with difficulty hearing whispers and use a hearing aid will receive 0 points, and those who do not will receive 1 point. The final score for the sensory perception domain, which is the sum of the vision and hearing scores, will range from 0 to 2.
The composite IC score will be calculated by adding the results of each domain, totaling 10 points.
We will perform additional analyses by determining a composite z-score for the composite IC score, which will be the sum of the individual z-scores for locomotion, vitality, psychological, and cognition domains, divided by 4. The sensory perception domain score will not be incorporated into the composite score due to the categorical nature of the scale used to assess it.
The next step will be to prescribe the exercises and begin the intervention protocol.
Intervention
The 12-week multicomponent training program includes individual and group sessions (10–20 participants) of 45 minutes, 5 times a week, in the following modalities: weight training, aerobic exercises, circular dance, Chinese healing gymnastics, Pilates matwork, “gerontomotricity”, hiking, fitness gymnastics, water activities, and Nordic walking. The exercises are prescribed according to American College of Sports Medicine 42 and Brazilian Ministry of Health guidelines. 43
The modalities will be recommended on a personalized basis, considering the physical needs and preferences of each older adult. The complexity of the exercises will be increased according to the participants’ perceived adaptation. Each modality is described in detail in the supplementary material ( https://doi.org/10.7910/DVN/UI5SGL).
The participants will also receive health education through lectures with experts, covering various topics, such as chronic disease control, healthy eating, how to be less sedentary, and adhering to medication regimens. The objective is to encourage a more balanced lifestyle and promote healthy aging.
Intervention-related adverse events will be classified as mild (muscle pain, fatigue), moderate (muscle strain, dislocation), or severe (fracture). Measures to prevent these events will be implemented.
Intervention follow-up
At the end of the intervention period (12 weeks), all participants will undergo a final assessment, in which variables from the initial assessment, physical variables, and variables related to the IC construct will be measured. Participants will be asked about the type of activities they participated in, their weekly frequency of participation, and their level of satisfaction with the project.
Statistical analysis
The data will be analyzed in GraphPad Prism 8.4, and an intention-to-treat approach will be used, including all initially enrolled participants, regardless of intervention adherence. Quantitative variables will be expressed as descriptive statistics, and qualitative variables will be expressed as frequency and proportion.
The effects of multicomponent training on composite IC and individual IC domains will be compared using paired Student’s t-tests. To determine the effects of different types of training on composite IC and individual IC domains, ANOVA with Bonferroni post-test will be used. Finally, the association between weekly exercise frequency and IC score will be determined using the Pearson correlation test. A significance level of 5% will be used in all tests.
This study has been approved by the Pontifícia Universidade Católica do Rio Grande do Sul Research Ethics Committee (decision 5517315, certificate 60234322.1.0000.5336), following the provisions of National Health Council Resolution 466 of 2012. All participants will provide written informed consent prior to enrollment.
RELEVANCE AND EXPECTED RESULTS
According to the World Health Organization, IC decline should be identified to understand aging more comprehensively and scientifically. 44 By using composite IC scores, targeted interventions can be developed to promote healthy aging in the community. 25
Nevertheless, assessing IC is still challenging due to the variety of ways each domain can be measured and the lack of consensus about the composite IC index. This also extends to interventions, since there are many multi-domain approaches with limited reference values in practice. Furthermore, some older adults do not benefit from very complex interventions due to their physical and cognitive limitations, which must be considered when developing exercise programs. 45
Thus, we believe that a simple multicomponent exercise intervention will be an effective strategy for maintaining and optimizing IC in older adults. Furthermore, longitudinal monitoring, exercise personalization, and individual support should increase adherence and involvement, as well as the social component.
Only one intervention study has used a composite IC score in its analysis, 45 which shows the relevance of this study, since we will use a comprehensive IC score, in addition to verifying the intervention’s effects on individual domains. Therefore, we expect our intervention to improve scores for both composite IC score and individual domains.
Our main study limitation is the lack of a control group or randomization, which prevents comparison with an equivalent group that did not receive the intervention. The intervention’s 12-week duration is also short, so the findings will not include its long-term impact. Unblinding could also introduce social motivation biases and influence active participation, impacting the validity of results for individual interventions.
ACNKOWLEDGEMENTS
The authors would like to thank Pontifícia Universidade Católica do Rio Grande do Sul and CAPES.
REFERENCES
World Health Organization. Decade of healthy ageing: baseline report. Geneva: WHO; 2020. Available from: https://www.who.int/publications/i/item/9789240017900. Accessed Aug 10, 2023.
World Health Organization. World report on ageing and health. Geneva: WHO; 2015. Available from: https://apps.who.int/iris/handle/10665/186463. Accessed Aug 10, 2023.
World Health Organization. Integrated care for older people: guidelines on community-level interventions to manage declines in intrinsic capacity. Geneva: WHO; 2017. Available from: https://apps.who.int/iris/handle/10665/258981. Accessed Aug 10, 2023.
Woodward M. Principles of geriatric medicine and gerontology. Australas J Ageing. 2006;25(3):169. https://doi.org/10.1111/j.1741-6612.2006.00177.x
Owsley C, Allman RM, Gossman M, Kell S, Sims RV, Baker PS. Mobility impairment and its consequences in the elderly. In: Clair JM, Allman R. The gerontological prism. New York: Taylor & Francis Group; 2018. p. 305-10.
Cesari M, Carvalho IA, Thiyagarajan JA, Cooper C, Martin FC, Reginster JY, et al. Evidence for the domains supporting the construct of intrinsic capacity. J Gerontol A Biol Sci Med Sci. 2018;73(12):1653-60. https://doi.org/10.1093/gerona/gly011.
Campbell CL, Cadar D, McMunn A, Zaninotto P. Operationalization of intrinsic capacity in older people and its association with subsequent disability, hospital admission and mortality: results from the english longitudinal study of ageing. J Gerontol A Biol Sci Med Sci. 2023;78(4):698-703. https://doi.org/10.1093/gerona/glac250
Paraskevoudi N, Balcı F, Vatakis A. “Walking” through the sensory, cognitive, and temporal degradations of healthy aging. Ann N Y Acad Sci. 2018;1426(1):72-92. https://doi.org/10.1111/nyas.13734
Gates GA, Mills JH. Presbycusis. Lancet. 2005;366(9491):1111-20. https://doi.org/10.1016/S0140-6736(05)67423-5
Wood C, Magnello ME, Jewell T. Measuring vitality. J R Soc Med. 1990;83(8):486-9. https://doi.org/10.1177/014107689008300803
Ryan RM, Frederick C. On energy, personality, and health: subjective vitality as a dynamic reflection of well-being. J Pers. 1997;65(3):529-65. https://doi.org/10.1111/j.1467-6494.1997.tb00326.x
Giudici KV, Souto Barreto P, Soriano G, Rolland Y, Vellas B. Defining vitality: associations of three operational definitions of vitality with disability in instrumental activities of daily living and frailty among elderly over a 3-year follow-up (MAPT Study). J Nutr Health Aging. 2019;23(4):386-92. https://doi.org/10.1007/s12603-019-1175-0
Murman DL. The impact of age on cognition. Semin Hear. 2015;36(3):111-21. https://doi.org/10.1055/s-0035-1555115
Fiske A, Wetherell JL, Gatz M. Depression in older adults. Annu Rev Clin Psychol. 2009;5:363-89. https://doi.org/10.1146/annurev.clinpsy.032408.153621
Schillerstrom JE, Royall DR, Palmer RF. Depression, disability and intermediate pathways: a review of longitudinal studies in elders. J Geriatr Psychiatry Neurol. 2008;21(3):183-97. https://doi.org/10.1177/0891988708320971
Smith L, Shin JI, Butler L, Barnett Y, Oh H, Jacob L, et al. Physical multimorbidity and depression: A mediation analysis of influential factors among 34,129 adults aged ≥50 years from low- and middle-income countries. Depress Anxiety. 2022;39(5):376-86. https://doi.org/10.1002/da.23250
Ma L, Chhetri JK, Zhang L, Sun F, Li Y, Tang Z. Cross-sectional study examining the status of intrinsic capacity decline in community-dwelling older adults in China: prevalence, associated factors and implications for clinical care. BMJ Open. 2021;11(1):e043062. https://doi.org/10.1136/bmjopen-2020-043062
Prince MJ, Acosta D, Guerra M, Huang Y, Jacob KS, Jimenez-Velazquez IZ, et al. Intrinsic capacity and its associations with incident dependence and mortality in 10/66 Dementia Research Group studies in Latin America, India, and China: a population-based cohort study. PLoS Med. 2021;18(9):e1003097. https://doi.org/10.1371/journal.pmed.1003097
Stolz E, Mayerl H, Freidl W, Roller-Wirnsberger R, Gill TM. Intrinsic capacity predicts negative health outcomes in older adults. J Gerontol A Biol Sci Med Sci. 2022;77(1):101-5. https://doi.org/10.1093/gerona/glab279
Liu S, Yu X, Wang X, Li J, Jiang S, Kang L, et al. Intrinsic capacity predicts adverse outcomes using integrated care for older people screening tool in a senior community in Beijing. Arch Gerontol Geriatr. 2021;94:104358. https://doi.org/10.1016/j.archger.2021.104358
Zeng X, Shen S, Xu L, Wang Y, Yang Y, Chen L, et al. The impact of intrinsic capacity on adverse outcomes in older hospitalized patients: a one-year follow-up study. Gerontology. 2021;67(3):267-75. https://doi.org/10.1159/000512794
Nelson ME, Rejeski WJ, Blair SN, Duncan PW, Judge JO, King AC, et al. Physical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc. 2007;39(8):1435-45. https://doi.org/10.1249/mss.0b013e3180616aa2
Galloza J, Castillo B, Micheo W. Benefits of exercise in the older population. Phys Med Rehabil Clin N Am. 2017;28(4):659-69. https://doi.org/10.1016/j.pmr.2017.06.001
Huang CH, Umegaki H, Makino T, Uemura K, Hayashi T, Kitada T, et al. Effect of various exercises on intrinsic capacity in older adults with subjective cognitive concerns. J Am Med Dir Assoc. 2021;22(4):780-6.e2. https://doi.org/10.1016/j.jamda.2020.06.048
Sánchez-Sánchez JL, Barreto PS, Antón-Rodrigo I, Ramón-Espinoza F, Marín-Epelde I, Sánchez-Latorre M, et al. Effects of a 12-week Vivifrail exercise program on intrinsic capacity among frail cognitively impaired community-dwelling older adults: secondary analysis of a multicentre randomised clinical trial. Age Ageing. 2022;51(12):afac303. https://doi.org/10.1093/ageing/afac303
Muneera K, Muhammad T, Althaf S. Socio-demographic and lifestyle factors associated with intrinsic capacity among older adults: evidence from India. BMC Geriatr. 2022;22(1):851. https://doi.org/10.1186/s12877-022-03558-7
Zhou M, Kuang L, Hu N. the association between physical activity and intrinsic capacity in chinese older adults and its connection to primary care: China Health and Retirement Longitudinal Study (CHARLS). Int J Environ Res Public Health. 2023;20(7):5361. https://doi.org/10.3390/ijerph20075361
Arias-Casais N, Amuthavalli Thiyagarajan J, Rodrigues Perracini M, Park E, Van den Block L, Sumi Y, et al. What long-term care interventions have been published between 2010 and 2020? Results of a WHO scoping review identifying long-term care interventions for older people around the world. BMJ Open. 2022;12(1):e054492. https://doi.org/10.1136/bmjopen-2021-054492
Gonzalez-Bautista E, Andrieu S, Gutiérrez-Robledo LM, García-Chanes RE, Souto Barreto P. In the quest of a standard index of intrinsic capacity. A critical literature review. J Nutr Health Aging. 2020;24(9):959-65. https://doi.org/10.1007/s12603-020-1503-4
Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey M, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1982;17(1):37-49. https://doi.org/10.1016/0022-3956(82)90033-4
Marshall A, Bauman A. The international physical activity questionnaire: summary report of the reliability & validity studies. IPAQ Executive Committee; 2001.
Craig CL, Marshall AL, Sjöström M, Bauman AE, Booth ML, Ainsworth BE, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35(8):1381-95. https://doi.org/10.1249/01.MSS.0000078924.61453.FB
Brazier J, Usherwood T, Harper R, Thomas K. Deriving a preference-based single index from the UK SF-36 Health Survey. J Clin Epidemiol. 1998;51(11):1115-28. https://doi.org/10.1016/S0895-4356(98)00103-6
Rikli RE, Jones CJ. Development and validation of a functional fitness test for community-residing older adults. J Aging Phys Act. 1999;7(2):129-61. https://doi.org/10.1123/japa.7.2.129
López-Ortiz S, Lista S, Peñín-Grandes S, Pinto-Fraga J, Valenzuela PL, Nisticò R, et al. Defining and assessing intrinsic capacity in older people: a systematic review and a proposed scoring system. Ageing Res Rev. 2022;79:101640. https://doi.org/10.1016/j.arr.2022.101640
Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39(2):142-8. https://doi.org/10.1111/j.1532-5415.1991.tb01616.x
Rikli RE, Jones CJ. Development and validation of criterion- referenced clinically relevant fitness standards for maintaning physical independence in later years. Gerontologist. 2013;53(2):255-67. https://doi.org/10.1093/geront/gns071
Lipschitz, DA. Screening for nutritional status in the elderly. Prim Care. 1994;21(1):55-67. https://doi.org/10.1016/S0095-4543(21)00452-8
Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16-31. https://doi.org/10.1093/ageing/afy169
Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695-9. https://doi.org/10.1111/j.1532-5415.2005.53221.x
Freitas S, Simões MR, Alves L, Santana I. Montreal cognitive assessment: validation study for mild cognitive impairment and Alzheimer disease. Alzheimer Dis Assoc Disord. 2013;27(1):37-73. https://doi.org/10.1097/WAD.0b013e3182420bfe
Nelson ME, Rejeski WJ, Blair SN, Duncan PW, Judge JO, King AC, et al. Physical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc. 2007;39(8):1435-45. https://doi.org/10.1249/mss.0b013e3180616aa2
Brasil. Ministério da Saúde. Secretaria de Atenção Primária à Saúde. Departamento de Promoção da Saúde. Guia de atividade física para a população brasileira. Brasília: Ministério da Saúde; 2021. Available from: https://bvsms.saude.gov.br/bvs/publicacoes/guia_atividade_fisica_populacao_brasileira.pdf. Accessed Dec 27, 2023.
Zhou Y, Ma L. Intrinsic capacity in older adults: recent advances. Aging Dis. 2022;13(2):353-9. https://doi.org/10.14336/AD.2021.0818
Liao X, Shen J, Li M. Effects of multi-domain intervention on intrinsic capacity in older adults: A systematic review of randomized controlled trials (RCTs). Exp Gerontol. 2023;174:112112. https://doi.org/10.1016/j.exger.2023.112112
Notes
This study received no specific funding from agencies in the public, commercial, or non-profit sectors.
This study was approved by the Research Ethics Committee of the Pontifical Catholic University of Rio Grande do Sul -PUCRS, following the provisions of resolution 466/2012.
This quasi-experimental study protocol was reported inspired in the TREND Statement, since there is no specific guideline for reporting study protocols for this design.
Author notes
Correspondence data Rafael Reimann Baptista – Avenida Ipiranga, 6.681 – Partenon – CEP: 90619-900 – Porto Alegre (RS), Brasil. Email: rafael.baptista@pucrs.br
Conflict of interest declaration
The authors declare no conflict of interest