VIEWPOINT
The geriatric 5Ms, artificial intelligence, and Hannah Arendt’s critique: ethical reflections within contemporary gerontology
 Andréia Pain
Ivan Aprahamian
Andréia Pain
Ivan Aprahamian
The geriatric 5Ms, artificial intelligence, and Hannah Arendt’s critique: ethical reflections within contemporary gerontology
Geriatrics, Gerontology and Aging, vol. 19, e0000298, 2025
Sociedade Brasileira de Geriatria e Gerontologia, SBGG
Received: 08 February 2025
Accepted: 24 April 2025
Abstract: The intersection of geriatrics, artificial intelligence (AI), and ethics presents a growing challenge in the field of aging medicine. The Geriatric 5Ms framework — Mind, Mobility, Medications, Multicomplexity, and Matters Most — guides current clinical practice in the approach to older patients. The integration of AI into geriatrics has the potential to improve diagnostic accuracy, optimize therapies, and individualize interventions. However, the automation of clinical decision-making carries inherent ethical risks, potentially reducing the patient to a set of data and weakening the physician-patient relationship. Hannah Arendt’s critique of the bureaucratization of thought and the banality of evil warns of the dangerous alienation of healthcare professionals in the face of uncritical reliance on algorithms. This article proposes a critical approach to the use of AI in geriatrics, emphasizing the need for a balance between technology and clinical judgment. The regulation of these technologies should prioritize equity, personalized care, and professional autonomy, ensuring that technological innovation reinforces — rather than replaces — patient-centered medical practice.
Keywords: Aging, artificial intelligence, ethics.
Geriatrics and gerontology, as interdisciplinary fields, seek to understand and address the complex demands of aging while promoting person-centered care. Advances in technology, particularly artificial intelligence (AI), have introduced new tools to optimize medical practice, enabling more accurate diagnoses, continuous monitoring, and personalized care. However, the growing integration of AI into geriatrics raises ethical concerns that directly relate to Hannah Arendt’s critique of the bureaucratization of thought and the banality of evil.1,2 Arendt argued that unquestioning adherence to impersonal systems can erode moral responsibility, a phenomenon that parallels the automation of medical decision-making, particularly in the care of older adults. In this context, analyzing the Geriatric 5Ms — Mind, Mobility, Medications, Multicomplexity, and Matters Most — becomes essential for assessing AI’s impact and ensuring that this technology strengthens rather than replaces professional autonomy and the humanization of care.3
The Geriatric 5Ms framework offers a comprehensive approach to guide the care of older adults, addressing areas from cognitive function assessment to multiple chronic disease management while respecting personal values and preferences.3 AI has the potential to considerably contribute to each of these domains, assisting in the early detection of cognitive decline, helping prevent falls by analyzing mobility patterns, optimizing medication regimens, managing multimorbidity, and identifying treatment priorities based on the patient’s medical history.4 However, the indiscriminate adoption of these technologies carries an inherent risk of replacing critical analysis with automated decisions, potentially reducing older adults to mere data points and weakening the interpersonal relationship that characterizes good medical practice.
Arendt’s warning about the dangers of bureaucratized thinking and unquestioning obedience to impersonal norms is particularly relevant to contemporary medicine. In Eichmann in Jerusalem: A Report on the Banality of Evil, Arendt argues that modern evil does not manifest solely in deliberately cruel acts but also in individuals’ inability to question the systems in which they operate.1 In geriatric care, this is reflected in the growing reliance on strict protocols and algorithms for clinical decision-making. If healthcare professionals abandon their clinical judgment in favor of automated guidelines, they might risk becoming mere system operators, neglecting the individuality of their patients.
Hyper-bureaucratization, a central element of Arendt’s critique, is increasingly evident in modern medicine. The time dedicated to filling out electronic medical records often surpasses the time spent actively listening to patients. Additionally, clinical protocols established by hospital management and insurers frequently prioritize financial efficiency over quality of care. When AI is introduced into this scenario, there is a risk that physicians may become overly reliant on algorithmic recommendations, disregarding nuances that only clinical experience and human interaction can provide.5
The application of AI in geriatrics can bring undeniable advancements, but it is crucial that this technology be used as a means rather than an end. In the Mind pillar, for instance, AI algorithms can analyze subtle patterns in language and behavior to detect cognitive decline before it becomes evident. However, AI should complement, not replace, the nuanced subjective clinical assessments that consider the emotional and social factors impacting an older adult’s cognition. Regarding Mobility, sensors and smart devices can predict fall risks by analyzing balance and gait, but the decisions on subsequent interventions must consider the patient’s life context, autonomy, and preferences. In Medications, AI systems can flag potentially dangerous drug interactions, but the selection of the optimal treatment regimen still requires individualized analysis, considering factors such as treatment adherence and subjective side effects.6
Equity in healthcare access must also be considered. AI is trained on vast datasets that often harbor implicit biases. Studies have demonstrated that medical algorithms can perpetuate existing racial and socioeconomic disparities because they reflect the biases present in the data they are built upon.6 In geriatrics, this could mean that older adults from certain groups, such as racial minorities or those with lower socioeconomic status, may be underdiagnosed or receive suboptimal treatments due to algorithmic shortcomings. The literature indicates that AI can amplify existing disparities in healthcare access, making it essential to implement regulatory and monitoring mechanisms for these technologies.7,8 In addition, it would be beneficial to consult publications from the World Health Organization (WHO)/Pan American Health Organization (PAHO) that discuss how ageism can influence the development and application of AI models, thereby reinforcing the ethical imperative for designing technology that is both inclusive and unbiased.9
Another central issue in discussions about AI in geriatrics is the humanization of care. The traditional patient-physician relationship, based on active listening and empathy, is increasingly being replaced by consultations through digital platforms. While telemedicine and AI tools offer benefits such as improved access to care, there is a qualitative loss when medical interactions become impersonal. Observing facial expressions, analyzing non-verbal communication, and exercising clinical intuition are fundamental aspects of medical practice that no AI can fully replicate. Studies have demonstrated that humanized care is a crucial factor in treatment adherence and patient recovery, reinforcing the need to balance technology with human presence (Figure 1).6
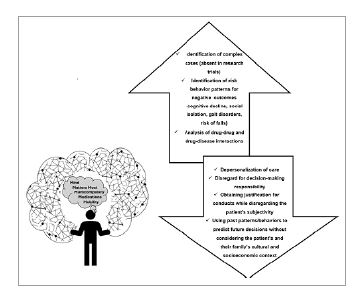
Figure 1
Challenges and benefits of artificial intelligence in geriatrics: between the personalization and dehumanization of care.
If Arendt were alive today, she would likely warn us of the danger of granting AI absolute decision-making power, relinquishing critical thought in favor of automated efficiency. The greatest threat lies not in technology replacing physicians, but rather in the risk of physicians ceasing to think, blindly trusting algorithms.1,2,10 AI can and should be used to enhance analytical capabilities, reduce diagnostic errors, and tailor treatments. However, its implementation should not undermine professional autonomy. Regulating these technologies should be regarded as an ethical imperative, ensuring that they enhance patient care rather than dehumanize it.
The future of geriatrics will depend on how we choose to integrate AI into the care of older adults. Several key principles are essential to ensure that this technology will be used ethically and effectively. First, AI should be seen as a support tool, not a replacement for human clinical judgment. Second, continuous monitoring of algorithms is necessary to prevent biases that could perpetuate existing inequalities. Third, medical education should incorporate critical training on AI, equipping professionals to interpret and question its recommendations. Finally, humanized care must be preserved, ensuring that the physician-patient relationship remains central in geriatric practice.3
Additionally, AI can play a crucial role in identifying treatment response patterns in complex older patients outside clinical trials or in better selecting highly complex patients for more inclusive clinical trials. This technology enables the inclusion of high-risk patients by identifying multiple concurrent factors with questionable collinearity in clinical terms, providing a more comprehensive and realistic analysis of geriatric conditions. Consequently, treatment advances become more representative and applicable to the older population, ensuring that the particularities and complexities of aging are adequately addressed in clinical practice.11
Beyond these challenges, another fundamental concern emerges: Geriatrics has historically been a less profitable area for technological development, as the difficulty in fitting symptoms and clinical conditions into strict protocols has limited the development of standardized solutions. This factor contributes to the exclusion of more complex older adults from critical clinical trials, particularly in the fields of cardiology, oncology, and psychiatry. Essential aspects such as frailty, cognition, nutrition, functionality, and multimorbidity have historically been overlooked in scientific research, hindering the development of truly effective strategies for this population. Therefore, the integration of AI into geriatrics must be coupled with active efforts to ensure that the particularities of aging are considered when developing new technologies and clinical guidelines.12
AI has the potential to revolutionize geriatrics by enhancing the efficiency and precision of care. However, its implementation must be guided by ethics and critical reflection. If medicine becomes excessively mechanized and depersonalized, we might risk losing what is most essential in the care of older adults: recognizing their individuality, history, and dignity. As Arendt taught us, the absence of critical thinking is the greatest danger of modernity. To prevent medicine from falling into the banality of evil, it is crucial to ensure that technology continues to serve humanity, rather than the other way around.1,13
REFERENCES
Arendt H. Eichmann em Jerusalém: um relato sobre a banalidade do mal. 4a ed. São Paulo: Companhia das Letras; 1999.
Arendt H. A condição humana. Rio de Janeiro: Forense Universitária; 2004.
Molnar F, Frank CC. Optimizing geriatric care with the GERIATRIC 5Ms. Can Fam Physician. 2019;65(1):39. PMID: 30674512.
Topol E. Deep medicine: how artificial intelligence can make healthcare human again. New York: Basic Books; 2019.
Obermeyer Z, Powers, BW, Vogeli C, Mullainathan S. Dissecting racial bias in an algorithm used to manage the health of populations. Science. 2019;366(6464):447-53. https://doi.org/10.1126/science.aax2342
Zulman DM, Sussman JB, Chen X, Cigolle CT, Blaum CS, Hayward RA. Examining the evidence: a systematic review of the inclusion and analysis of older adults in randomized controlled trials. J Gen Intern Med. 2011;26(7):783-90. https://doi.org/10.1007/s11606-010-1629-x
Schwartz JB. Representative enrolment of older adults in clinical trials: the time is now. Lancet Healthy Longev. 2023;4(7):e301-e303. https://doi.org/10.1016/S2666-7568(23)00088-0
Tip sheet: the 5ms of geriatrics. HealthInAging.org; 2020. Available from: https://www.healthinaging.org/tools-and-tips/tip-sheet-5ms-geriatrics. Accessed in Feb. 02, 2025.
World Health Organization. Ageism in artificial intelligence for health: policy brief. Geneva: WHO; 2022. Available from: https://www.who.int/publications/i/item/9789240040793. Accessed in Feb. 02, 2025.
Abadir P, Chellappa R. Artificial intelligence in geriatrics: riding the inevitable tide of promise, challenges, and considerations. J Gerontol A Biol Sci Med Sci. 2024;79(2):glad279. https://doi.org/10.1093/gerona/glad279
Ma B, Yang J, Wong FKY, Wong AKC, Ma T, Meng J, et al. Artificial intelligence in elderly healthcare: a scoping review. Ageing Res Rev. 2023;83:101808. https://doi.org/10.1016/j.arr.2022.101808
Harari YN. Homo Deus: uma breve história do amanhã. São Paulo: Companhia das Letras; 2016.
Chomsky N. Inteligência artificial: o futuro da humanidade? São Paulo: WMF Martins Fontes; 2021.
Notes
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Not applicable.
Not applicable.
This paper is a viewpoint, so none of the standard guidelines apply.
Author notes
Correspondence data Virgílio Garcia Moreira – Rua Enaldo Cravo Peixoto, 215 – CEP: 20540-106 – Rio de Janeiro (RJ), Brazil. E-mail: virgilio.garcia.moreira@gmail.com
Conflict of interest declaration
The authors declare no conflicts of interest.